Download presentation
Presentation is loading. Please wait.

1
T₃: Triiodothyronine T₄: Thyroxine
Thyroid Disorders T₃: Triiodothyronine T₄: Thyroxine

3
I. Hyperthyroidism (Thyrotoxicosis)
Characterized by hypermetabolism of all body systems & increased serum levels of free thyroid hormones. More common in women. Rare in children Less common than hypothyroidism

4
Thyroid Storm: Exaggerated form of hypertoxicosis. Medical emergency Prompt treatment May be precipitated by : -Infection -Trauma - Surgery -Embolism -Diabetic ketoacidosis -Others…

5
Subclinical Hyperthyroidism:
Suppressed TSH level w/ NL thyroid hormone levels. Symptoms are NOT always present esp. in elderly. Pathophysiology: See p

6
Treatment Goals of Hyperthyroidism:
Reverse S/S, normalize thyroid hormone levels, min. deleterious S/Es of T₄ on organ systems, prevent thyroid storm, & improve overall functional capacity. Reverse hyperthyroid complaints. Reverse hyperthyroid physical findings. Normalize free T₄, T₃, & TSH levels. Reduce goiter size.

7
Improve cardiac function & prevent systemic
embolism. 7) Preserve bone density& prevent osteoporosis. 8) Improve emotional well being& quality of life. 9) Support placenta development & maintenance of pregnancy. 10) Promote normal growth, & physical & mental development.
 Preserve bone density& prevent osteoporosis. 8) Improve emotional well being& quality of life. 9) Support placenta development & maintenance. of pregnancy. 10) Promote normal growth, & physical & mental development.")
8
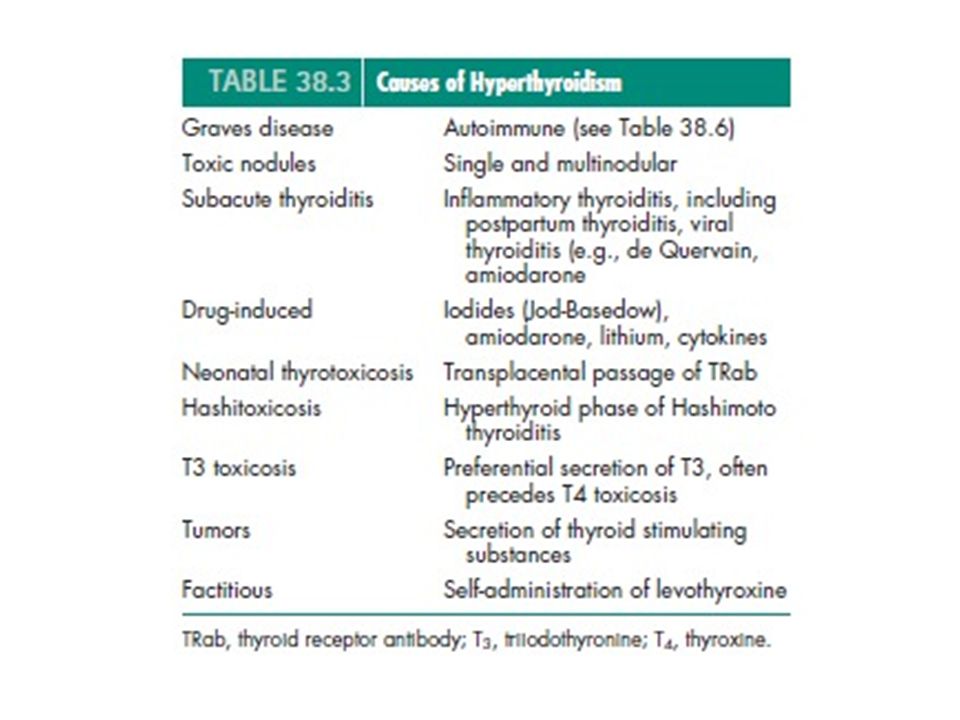
Causes of Hyperthyroidism: (table38.3 p.993)
Graves disease: -Autoimmune -May occur w/ other autoimmune disorders. -Most common cause -Charact. by hyperthyroid. & one or more of the following: * Goiter * Exophthalmos * Dermopathy

9
2) Toxic Nodules: -Single & multinodular -Autonomous: independent of TSH control. -May be caused by: *Iodine deficiency *Genetic abnormality *Immune System

10
3) Subacute Thyroiditis: - Inflammatory thyroiditis, i. e
3) Subacute Thyroiditis: - Inflammatory thyroiditis, i.e.Postpartum(PPT), viral (i.e. de Quervain). - Hyperthyroid. from leakage of thyroid hormones into circulation due to inflamed gland & NOT increased synthesis. -Hypothyroidism may follow.
 Subacute Thyroiditis: - Inflammatory thyroiditis, i.e.Postpartum(PPT), viral (i.e. de Quervain). - Hyperthyroid. from leakage of thyroid hormones into circulation due to inflamed gland & NOT increased synthesis. -Hypothyroidism may follow.")
11
4) Drug Induced: -Iodides (Jod-Basedow), Amiodarone, Lithium, Cytokines 5) Neonatal thyrotoxicosis (Graves): -Transplacental passage of TRab causing the infant to be extremely ill w/in delivery hrs. -Self-limiting.

12
6) Hashitoxicosis: -Hyperthyroid phase of Hashimoto thyroiditis 7) T₃ toxicosis: -Preferential secretion of T₃, often precedes T₄ toxicosis. 8) Tumors: -Secretion of thyroid stimulating substances. 9) Factitious: -Self-administration of levothyroxine
 Tumors: -Secretion of thyroid stimulating substances. 9) Factitious: -Self-administration of levothyroxine .")
15
Clinical Presentation & Diagnosis:
- Characteristics of Graves Dz. p.997 Table 38.6 -SxS of Hyperthyroidism & Hypothyroidism p.995 Table 38.4 - Thyroid Function Tests (TFTs) p
 p")
16
Diagnosis of Hyperthyroidism :
Confirmed w/ abnormally high levels of FT₄ or TT₃ & undetectable TSH. 2) +Antibodies, opthalmopathy, or dermopathy confirms the diagnosis of Graves. 3) RAIU in Graves but is NOT cost-effective 4) TT₃ & + TRab are essential for atypical presentation, i.e. in elderly.
 +Antibodies, opthalmopathy, or dermopathy. confirms the diagnosis of Graves. 3) RAIU in Graves but is NOT cost-effective. 4) TT₃ & + TRab are essential for atypical presentation, i.e. in elderly.")
17
5) Subacute Thyroiditis (PPT,…), Diagnosis is confirmed by:
5) Subacute Thyroiditis (PPT,…), Diagnosis is confirmed by: *Low or undetectable RAIU. * TH levels. *Suppressed or undetectable TSH level. * ESR * No Thyroid Ab. * Leukocytosis, gland tenderness, & S/S of hyper or hypothyroidism.
 Subacute Thyroiditis (PPT,…), Diagnosis is confirmed by: *Low or undetectable RAIU. * TH levels. *Suppressed or undetectable TSH level. * ESR * No Thyroid Ab. * Leukocytosis, gland tenderness, & S/S of hyper or hypothyroidism.")
25
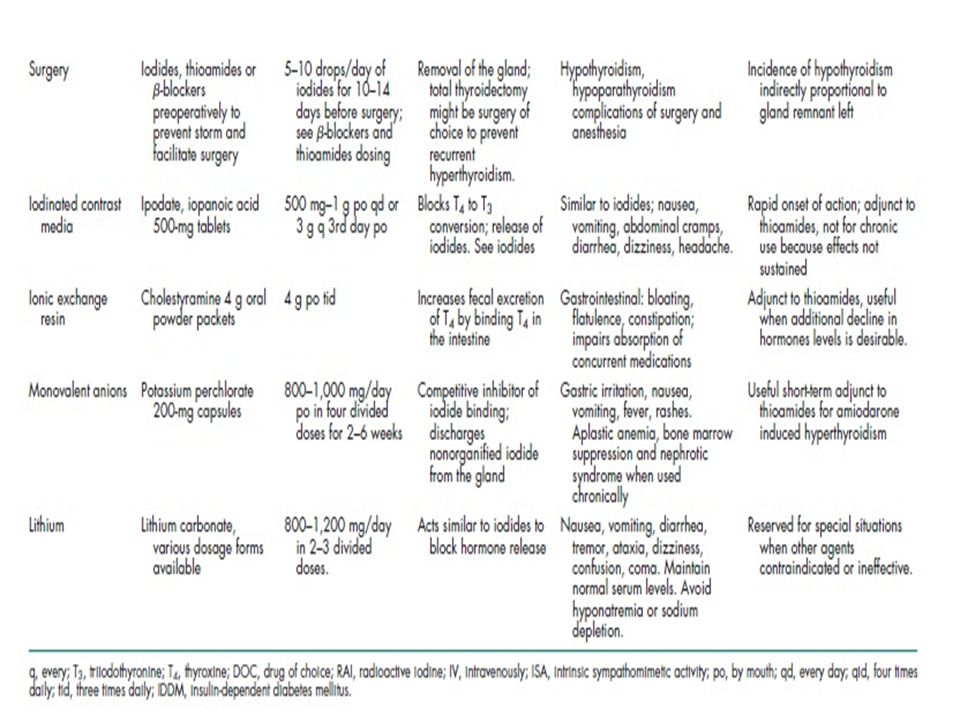
Therapeutic Plan: (table 38.7, p.998-999)
Major Modalities for Management of Hyperthyroidism, include: 1) Thioamides 2) RAI 3) Surgery ** Treatment must be individualized, each has advantages & limitations **Effective Treatment Selection p.1000, Fig.38.3
 Thioamides. 2) RAI. 3) Surgery. ** Treatment must be individualized, each has. advantages & limitations. **Effective Treatment Selection p.1000, Fig")
26
Treatment Adjuncts: Iodides Iodinated Contrast Media K Perchlorate Adrenergic Antagonists Corticosteroids Cholestyramine Rarely Li

27
In U. S. , RAI is most commonly used except in younger pts
In U.S., RAI is most commonly used except in younger pts. for whom Thioamides are used. In Europe & Japan, Thioamides are the TOC. Surgery is the last choice unless there is: *Obstructive symptoms or* Malignancy

28
Treatment is individualized a/c to:
1. Etiology 2. Pt. age 3. Goiter size 4. Thyroid & Medical complications 5. Social & Economic issues

29
Graves: All 3 methods are effective but pt. or Dr. may. prefer meds
Graves: All 3 methods are effective but pt. or Dr. may prefer meds. over RAI or surgery. TMG: RAI or surgery > effective than meds., but factors as medical condition or pt or Dr. may prefer RAI use over surgery. 3.Transient Treatment : may be used when the disease is self-limited, i.e.: * Subacute Thyroiditis (PPT,…) *Neonatal Graves *Drug-Induced Hyperthroidism
 *Neonatal Graves. *Drug-Induced Hyperthroidism.")
30
In Uncomplicated Graves esp
In Uncomplicated Graves esp. in children, Thioamides are preferred until remission. Thioamides: - Do NOT destroy the gland - Control the disease - Chronic thyroid replacement may not be necessary (not like w/ RAI or Surg.), however, hypothyroid. may still develop eventually.
, however, hypothyroid. may still develop. eventually.")
31
If RAI or Surgery is selected, most older pts
If RAI or Surgery is selected, most older pts. & all severely ill thyrotoxic pts. should be pretreated w/ Thioamides. Pretreatment: Depletes gland of stored hormones. Hypermetabolic rate. Prevents leakage of hormone from gland after RAI or during surgery preventing thyroid storm.

32
Optimal Tx of hyperthyroidism in Graves opthalmopathy is unresolved.
Some prefer RAI or surgery (<desirable) to remove the antigen source (gland) & > effective than thioamides to prevent progressive opthalmopathy. Prophylactic systemic corticosteroid (e.g., Prednisone 30-40mg daily starting within a few days of RAI & cont. for ~2-3 wks. to prevent further progression of opthalmopathy in pts. w/ re-existing cases. Hypothyroidism can aggravate preexisting eye complaints. Hyperthyroidism control & hypothyroidism prevention are essential to prevent progression of opthalmopathy.
 to remove the antigen source (gland) & > effective than thioamides to prevent progressive opthalmopathy. Prophylactic systemic corticosteroid (e.g., Prednisone 30-40mg daily starting within a few days of RAI & cont. for. ~2-3 wks. to prevent further progression of opthalmopathy in pts. w/ re-existing cases. Hypothyroidism can aggravate preexisting eye complaints. Hyperthyroidism control & hypothyroidism prevention are essential to prevent progression of opthalmopathy.")
33
Single or Toxic multinodular Dz.:
Best managed with definitive Tx, i.e. RAI or surgery, because spontaneous remission is unlikely. Hyperthyroid Children: The usual Tx choices are Thioamides & subtotal thyroidectomy, although all 3 methods have been used.

34
In Pregnancy: Hyperthyroidism is difficult to manage. Spontaneous remission may occur because of the decrease in TRab. Antithyroid meds. are often NOT necessary. If untreated, complications may occur. RAI & Iodides are Contraindicated in pregnancy. Surgery in 2nd trimester is an option.

35
Neonatal Graves: Infants extremely ill w/in delivery hrs. Supportive measures, i.e. *sedation *O₂ *Fluids/Electrolytes Short-term (temporary) thioamides, iodides, or beta blockers since it is self-limiting. Symptoms disappear in 1-2 months, therefore, withdraw antithyroids at this time.
 thioamides, iodides, or beta blockers since it is self-limiting. Symptoms disappear in 1-2 months, therefore, withdraw antithyroids at this time.")
36
Subacute Thyroiditis:
Self-limiting (common spontaneous recovery). Symptomatic treatment: *Heat *Rest *NSAIDs *Beta-blockers * Thioamides are NOT effective since it is due to thyroid hormone leakage & NOT increase in TH synthesis.
. Symptomatic treatment: *Heat. *Rest. *NSAIDs. *Beta-blockers. * Thioamides are NOT effective since it is due to thyroid hormone leakage & NOT increase in TH synthesis.")
37
Cont. Subacute Thyroiditis:
Corticosteroids are indicated for severe inflammation if NSAIDs are ineffective. In Hypothyroid phase: Transient thyroid replacement is used to suppress further TSH stimulation to damaged gland & treat hypothyroid symptoms.

42
Treatment: Fig.38.3 p.1000 Pharmacotherapy: Thioamides: *Long-term 1⁰ therapy for Graves esp. in children & adolescents. *Transiently used to reduce TH levels before definitive therapy w/ RAI or surgery. *TOC for small goiters & mild dz. For whom a high remission rate is likely.

43
Advantages: Potential for remission without gland damage. Limitations: 1.Non-adherence 2.Strict parental & physician supervision in kids. 3.Low success rates. 4. Risk of ADRs.

44
Thioamides: Methimazole 2. Propylthiouracil (PTU) They prevent TH synthesis. PTU (Not Methimazole) inhibits peripheral deiodination of T₄ to T₃. They suppress TSH receptor Ab level by unknown immunosuppressive MOA.

45
Thioamides Selection:
Pharmacologic Differences: ** Methimazole is preferred over PTU, because: 1. Single daily dose ( PTU Q6-8H) 2. More potent than PTU 3. Less toxic than low doses. 4. Less costly. ** Both are equally equipotent doses.
 2. More potent than PTU. 3. Less toxic than low doses. 4. Less costly. ** Both are equally equipotent doses.")
46
PTU is preferred over methimazole in pts. w/
**Thyroid Storm Or **Severe Hyperthyroidism Because: PTU blocks the conversion of T₄ to T₃ peripherally. PTU may have faster OA. *PTU is preferred in pregnancy because methimazole may be associated w/ congenital skin defect ( NOT sufficiently supported & has been used in pregnancy without deleterious effects). *Both can be used safely in pregnancy *PTU is preferred in lactation because insignificant amounts are secreted in the breast milk. *Generally, Methimazole is the thioamide of choice EXCEPT in the situations mentioned above where PTU is preferred , or if the patient cannot tolerate methimazole.
. *Both can be used safely in pregnancy. *PTU is preferred in lactation because insignificant amounts are secreted in. the breast milk. *Generally, Methimazole is the thioamide of choice EXCEPT in the. situations mentioned above where PTU is preferred , or if the patient. cannot tolerate methimazole.")
47
No IV preparations of thioamides.
It usually takes 6-8wks before SxS subside & TH normalize. Initial dose: Methimazole mg/d orally or PTU mg/d in 3-4 divided doses. **Tapering down dose only after SxS subside: **Initial dose is reduced gradually by 1/3 each month until daily M.D. of 5-15mg methimazole or mg PTU is reached.

48
Baseline FT₄ & WBC count w/ differ
Baseline FT₄ & WBC count w/ differ. should be done before thioamides are started because agranulocytosis can be induced by thioamides & also hyperthyroidism is associated w/ relative reduction of neutrophils. FT₄ or FT₄I & TSH should be monitored 4-8 wks after starting Tx & after any dose change. Once stable thioamide M.D. is reached, TFTs should be monitored Q 2-4 or Q3-6 months.

49
Recommended duration of Tx for Graves is emperic: Generally 12-18 months.
12 months is the minimum Tx duration recommended to maximize remission potential. Longer durations can be used if NO ADRs. Some pts. remain in remission & others relapse ????

50
Toxic Reactions: Pruritic Maculopapular Skin Rash: Most common & treated w/ antihistamines. Hepatatis: *If LFTs normalize w/in 3 months of dose reduction, NO need to discontinue PTU. *If there is clinical evidence of hepatitis, D/C PTU immediately. * Routine monitoring of LFTs is required for: 1. Pts. w/ liver dz. history. 2. Hepatitis risk factors, i.e. alcoholism

51
3) Hypoprothrobinemia (w/ PTU):. Rare
3) Hypoprothrobinemia (w/ PTU): * Rare * Recovery may occur after D/C of PTU, if not start steroids. 4) Agranulocytosis (PMNs<500): *Most serious but rare. * Likely to occur during the 1st 6 wks of Tx. * Complete recovery is seen a few days to 3 wks after D/C of thioamide. * Granulocyte colony-stimulating factor & corticosteroids may shorten the recovery period.
 Hypoprothrobinemia (w/ PTU): * Rare * Recovery may occur after D/C of PTU, if not start steroids. 4) Agranulocytosis (PMNs<500): *Most serious but rare. * Likely to occur during the 1st 6 wks of Tx. * Complete recovery is seen a few days to 3 wks after D/C of thioamide. * Granulocyte colony-stimulating factor & corticosteroids may shorten the recovery period.")
52
2) K Perchlorate: MOA: Interferes w/ Iodine binding causing discharge of non-organified iodide from the gland. *Especially useful for the short-term management of drug-induced hyperthyroidism because it is competitive inhibitor of iodide, but its antithyroid effect can be overcome by iodine administration. *Short-term adm. (2-6wks) is well tolerated. *Limited use of chronic Tx is due to: 1) Irreversible aplastic anemia 2) Nephrotic syndrome
 is well tolerated. *Limited use of chronic Tx is due to: 1) Irreversible aplastic anemia 2) Nephrotic syndrome .")
53
3) Iodides:. Clinical use superseded by thioamides & beta blockers
3) Iodides: *Clinical use superseded by thioamides & beta blockers. *MOA: 1)Inhibit iodide organification (Wolf-Chaikoff). ** 2)Inhibit TH release (Rapid Sx relief in 2-7d) 3)Decrease gland vascularity. *Rapid effect is beneficial for: 1. Thyroid storm 2. Pts. awaiting thioamide onset
 Iodides: *Clinical use superseded by thioamides & beta blockers. *MOA: 1)Inhibit iodide organification (Wolf-Chaikoff). ** 2)Inhibit TH release (Rapid Sx relief in 2-7d) 3)Decrease gland vascularity. *Rapid effect is beneficial for: 1. Thyroid storm 2. Pts. awaiting thioamide onset")
54
Iodides are NOT to be given before RAI because iodides block effective RAI retention by the gland for several wks. after use. Iodides are given 10-14days before surgery to: 1. Reduce vascularity 2. Increase firmness of hyperplastic gland to facilitate surgical removal. Preoperatively: Iodides+ Thioamides Comb. ( Preferred ) Iodides + Beta Blockers Comb. All 3 of them could be used.
 Iodides + Beta Blockers Comb. All 3 of them could be used.")
55
Major S/Es of Iodides: Hypersensitivity reactions Hyperthyroidism ( from failure of Wolff-Chaikoff block) Hypothyroidism ( unable to escape from Wolf-Chaikoff) Chronic adm. in pregnancy fetal goiter & asphyxation
 Chronic adm. in pregnancy fetal goiter & asphyxation.")
56
Advantages of Iodides:
Simplicity Low cost Low toxicity No gland destruction Limitations: Escape Tx relapse Allergy Interference w/ subsequent RAI therapy

57
4) Adrenergic Blockers:
4) Adrenergic Blockers: **Depletes or blocks the effects of TH on tissue catecholamines Rapid symptomatic relief before thioamides, RAI, or surgery. *Do NOT affect underlying dz. *Are NOT used as primary therapy *Propranolol Standard & most widely used (20-40mg TID or QID)
 Adrenergic Blockers: **Depletes or blocks the effects of TH on tissue catecholamines Rapid symptomatic relief before thioamides, RAI, or surgery. *Do NOT affect underlying dz. *Are NOT used as primary therapy *Propranolol Standard & most widely used (20-40mg TID or QID)")
58
Severe toxemia may need up to 480mg/day
Symptoms relieved by beta-blockers include: *palpitations *tachcardia *anxiety *sweating *tremor *diarrhea *Neuromuscular manifestations Symptoms NOT affected by beta-blockers include: *circulating TH *Wt. loss *goiter *O₂ consumption *exophthalmos

59
Beta-blockers are used as adjunct Tx w/ thioamides or RAI for:
*Neonatal thyrotoxicosis *Hyperthyroidism in pregnancy *Thyroid storm *Pre-operatively Only used for short term in pregnancy because chronic use in pregnancy esp. 3rd trimester & lactation should be avoided due to fetal complications.

60
Calcium Channel Blockers
esp. Diltiazem p.o. 120mg TID or 60mg QID may be used as alternative to beta blockers when contraindicated, i.e. asthma or DM1

61
5) RAI: Radioactive Iodine)
*Indicated for: Post-adolescent hyperthyroid patients Graves opthalmopathy Hx of thyroid surgery Poor surgical candidates Who fail or experience thioamide toxicity TOC for older patients w/ cardiac dz or those w/ TMGs (Toxic Multinodular Goiter) **I₁₃₁ isotope is the most commonly used **Absolute contraindication in pregnancy: destroys the fetal gland .
 **I₁₃₁ isotope is the most commonly used. **Absolute contraindication in pregnancy: destroys the fetal. gland .")
62
RAI dosage is calculated using a certain formula.
RAI pts. should be pretreated w/: *thioamides to deplete the gland of the stored TH Or*beta blockers or Ca channel blockers before & after RAI to prevent exacerbations of thyrotoxicosis w/in 10-14days after RAI due to leakage of TH after RAI. *Methimazole: *preferred as pretreatment over PTU *showed > success as preTx. *because PTU is associated w/poorer RAI retention & higher RAI failure rates

63
Resolution of hyperthyroidism is slow:
Sx improvement :by 3-6wks after RAI Max. effect : 3-4 months after an ablative dose Other therapies may be needed after RAI due to delayed onset for symptomatic control. Major concerns: *Carcinogenesis * Leukemia * Genetic damage which are unfounded.

64
Advantages of RAI: 1) Effective 2) Quick 3) Painless 4) Nontoxic Major Complications: Hypothyroidism : Most common in the 1st year & increases w/ time.

65
Iodinated Contrast Media:(e.g. Ipodate)
Inhibits peripheral deiodination of T₄ to T₃. Inhibits TH secretion. Relatively non-toxic. Useful adjuncts to thioamides in the management of: Severe thyrotoxicosis Thyroid storm Amiodarone-induced thyrotoxicosis Alternative for those allergic to thioamides in the preoperative preparation ** Chronic use is not indicated because its effectiveness in reducing TH is not sustained for more than 1 month in most cases.

66
Non-pharmacological Therapy:
Surgery (Thyroidectomy): Treatment of Choice for: 1. Contraindications of RAI or Thioamides. 2. Large goiters causing:*cosmetic disfigurement * resp. distress * swallowing difficulties 3. Suspected Malignancies. 4. Selected children & pregnants.
: Treatment of Choice for: 1. Contraindications of RAI or Thioamides. 2. Large goiters causing:*cosmetic disfigurement. * resp. distress. * swallowing difficulties. 3. Suspected Malignancies. 4. Selected children & pregnants.")
67
Euthyroidism produced by surgery is faster & is assoc
Euthyroidism produced by surgery is faster & is assoc. w/ lower relapse rates than w/ RAI or thioamides. Poor Surgical Candidates: Severe cardiac, resp., or debilitating dz. 3rd trimester pregnant (spontaneous labor) **Risk of recurrent thyrotoxicosis is directly proportional to amount of remnant left of the gland. **Subtotal Thyroidectomy is preferred
 **Risk of recurrent thyrotoxicosis is directly. proportional to amount of remnant left of the gland. **Subtotal Thyroidectomy is preferred.")
68
Total thyroidectomy: 1. Increases the risk of hypothyroidism 2. Prevents recurrence of hyperthroidism Surgery pts. should be adequately prepared w/standard combination of: 1. Thioamide 2. Iodides or 3. Beta-blockers

69
Major Surg. Complication:
*Hypothyroidism in the 1st 6mos-3yrsafter surg. or as late as 10yrs. after surgery. Advantages of Surgery: Rapid recovery Definitive surgical intervention 3. Lack of need for the rigid dosing schedule of the thioamides Disadvantages of Surgery: 1. Expense 2. Need of hospitalization 3. Risk of anesthesia 4. Postoperative complications 5.Fear of surgery

70
Special Treatment Issues:
1.Subclinical Hyperthyroidism: Tx is controversial Tx is considered for high risk pts.: *>60y.o. *Cardiac dz. *Atrial Fibrillation *Osteoporosis * Without risk factors: Observe & Do routine TSH monitoring

71
2. Exophthalmous & Ophthalmologic Complications:
*Ocular Tx: symptomatic till euthyroidism occurs *Elevation of bed head for diuresis. *Protective glasses + Methylcellulose (lubricant) Hydrocortisone drops *Avoid smoke & dust *Tape eyes during sleep to prevent corneal scarring & drying. *Systemic corticosteroids for progressive inflammatory exophthalmous & reduced visual acuity: Prednisone mg/d in divided doses X 1-3 wks then taper when sxs resolve over 2 wks then Discontinue. External orbital radiation therapy for contraindications to corticosteroids. After euthyroidism & stable eye Sx Lid or orbital surgery for cosmetic or visual correction
 Hydrocortisone drops. *Avoid smoke & dust. *Tape eyes during sleep to prevent corneal scarring & drying. *Systemic corticosteroids for progressive inflammatory exophthalmous & reduced. visual acuity: Prednisone mg/d in divided doses X 1-3 wks. then taper when sxs resolve over 2 wks. then Discontinue. External orbital radiation therapy for contraindications to corticosteroids. After euthyroidism & stable eye Sx Lid or orbital surgery for cosmetic or visual correction.")
72
3. Atrial Fibrillation & CHF:
3. Atrial Fibrillation & CHF: *Hyperthyroidism or subclinical hyperthyroidism can cause or worsen A. Fibrillation & CHF which are difficult to control until euthyroid. *Hyperthyroid pts. Resistant to Digoxin *Hypothyroid pts. Very sensitive to Digoxin * Warfarin is recommended in pts. w/ hyperthyroidism-related A.Fib, valvular dz.,& CHF due to high risk of systemic emboli

73
4. Thyroid Storm: *Treatment: Support vital signs w/: *Sedation *O₂ *Fluids/Electrolytes *Antipyretics *Treat infection *Corticosteroids (Hydrocortisone mg I.V. Q6H) 2. Thioamides & Iodides in large doses: *PTU mg Q6H or *Methimazole 30-40mg Q6H *Iodides added 1hr after thioamides Lithium used if iodides are contraindicated Cholestyramines may also be recommended
 2. Thioamides & Iodides in large doses: *PTU mg Q6H. or. *Methimazole 30-40mg Q6H. *Iodides added 1hr after thioamides. Lithium used if iodides are contraindicated. Cholestyramines may also be recommended.")
74
Thyroid Storm cont.: Propranolol 20-80mg p.o. Q6H or 0.5-2mg IV or comparable beta-blocker or Diltiazem mg p.o. TID or QID to control HR. Eliminating & correcting precipitating factors. 6. Removing circulating hormones by: a. Plasmapheresis b. Exchange transfusion c. Dialysis when routine measures fail. TSH is the most sensitive for diagnosis.

75
Hypothyroidism

76
Hypothyroidism: Caused by TH deficiency. Characterized by slowing down of all body systems. Myxedema: Exaggeration of SxS of severe prolonged hypothyroidism preceding coma Myxedema Coma: End-stage of long-standing uncorrected hypothyroidism. Cretinism or Congenital Hypothyroidism; Hypothyroidism developing in the utero or in neonates & can lead to mental & growth impairment.

77
Subclinical Hypothyroidism:
Increased TSH & Normal TH usually without symptoms of hypothyroidism. * Primary Hypothyroidism: *Failure of thyroid gland to secrete sufficient TH *Most common type Secondary Hypothyroidism: Rare Due to pituitary or hypothalamic injury.

78
Treatment Goals: p.1007 More common in females Risk Factors: 1.Family hx of thyroid or autoimmune disorder 2.Older age, esp. women 3.Medically treated thyroid dz. Types of Hypothyroidism by cause: Goitrous Nongoitrous

79
Goitrous forms include:
*Hashimotos thyroiditis: *Most common in U.S. *Autoimmune *Drug-induced thyroiditis: *Iodides *Lithium *Cytokines *Thiocyanate *Dyshormogenesis: *Familial thyroid disorders from abnormalities in synthesis, delivery, or peripheral action of TH. *Endemic thyroiditis: *Caused by Iodine deficiency during growth years. *Subacute Thyroiditis *Multinodular Goiters (MNG)
")
80
2. Nongoitrous forms include: *Cretinism *Idiopathic atrophy (uncommon) *Iatrogenic causes: *2nd most common *by RAI or surgery *Pituitary causes (uncommon)
 *Iatrogenic causes: *2nd most common *by RAI or surgery *Pituitary causes (uncommon) .")
81
SxS: * Table 38.4 * Atypical in elderly SxS from naturally occurring hypothyroidism (Hashimoto): insidious & unnoticed x mos-yrs before terminal myxedema state. Iatrogenic Hypoth. (by RAI or Surgery):occur rapidly.
:occur rapidly.")
82
Hypothyroid. pts. : sensitive to meds. i.e.:
*Digoxin *Anesthetics *Narcotics *Sedatives-hypnotics Medical Tx of concurrent diseases (DM, Hyperlipidemia, Cardiac conditions): Maybe influenced
: Maybe influenced.")
83
Diagnosis: May go unnoticed
Recommended to measure TSH 35y.o. & every 5 yrs thereafter esp. in women. Adults: * Low FT₄I or FT₄ (T₃ may be normal) * Increased TSH Secondary Hypothyroid: *Low FT₄ *Low TSH *Other features of pituitary or hypothalamic dz. Hashimoto Thyroiditis: *Antibodies present
 * Increased TSH. Secondary Hypothyroid: *Low FT₄. *Low TSH. *Other features of pituitary or hypothalamic dz. Hashimoto Thyroiditis: *Antibodies present.")
84
Therapeutic Plan: Fig. 38.4 p.1011
TH administration provides adequate replacement therapy for Hypothyroidism & prevents progression to myxedema coma. Average Dose= mcg L-thyroxine QD (parallels normal TH production) * mcg QD in females * mcg QD in males Dosing requirements depend on: age, weight, severity, cause, cardiac dz., hormone absorption.
 * mcg QD in females. * mcg QD in males. Dosing requirements depend on: age, weight, severity, cause, cardiac dz., hormone absorption.")
85
Treatment: Pharmacotherapy: L-thyroxine: Preparation of choice. Other commercial preparations (table 38.9) Young-healthy pt. w/ short duration dz.: Administer L-thyroxine mcg QD ( mcg/kg/d) Dose can be adjusted using SxS & lab values @ steady-state (after 6-8 wks of Tx)
 Dose can be adjusted using SxS & lab steady-state (after 6-8 wks of Tx)")
86
Older pts.= mcg QD Old w. Cardiovascular Dz.= 25 mcg QD Lower doses are sufficient for hypothyroidism caused by RAI or surgery than with spontaneous hypothyroidism. Pregnancy: Increase the pre-pregnancy dose of L-thyroxine by 20-30% in 1st or nd trimester.

87
Malabsorption by SBS or coadministration w/ several meds. (tab. 38
*Malabsorption by SBS or coadministration w/ several meds.(tab.38.10)Reduces thyroxine absorption *Improvement in typical SxS should be seen after 3-4 wks of Tx. *Wt., skin, hair, voice changes: May NOT reverse for months despite normal TFTs. *TSH & FT₄ : Should be SS (after 2-3 mos. of daily dosing) *Changes in TSH lag behind changes in TH. Therefore, TSH & T₄ should be checked NOT earlier than 4 wks after starting Tx. *Once dose is established: Evaluate yearly intervals
Reduces thyroxine absorption *Improvement in typical SxS should be seen after 3-4 wks of Tx. *Wt., skin, hair, voice changes: May NOT reverse for months despite normal TFTs. *TSH & FT₄ : Should be SS (after 2-3 mos. of daily dosing) *Changes in TSH lag behind changes in TH. Therefore, TSH & T₄ should be checked NOT earlier than 4 wks after starting Tx. *Once dose is established: Evaluate yearly intervals")
88
Avoid over-replacement to avoid hyperthyroidism which can increase the risk of: * osteoporosis
* Bone loss * Cardiac arrhythmias 1. L-thyroxine (T₄) whose t⅟₂=7days: The most popular of the 8 commercial preparations because of: 1. Potency 2. Cost-effectiveness 3. Lack of foreign protein antigenicity 4. Ease of dosing
 whose t⅟₂=7days: The most popular of the 8 commercial preparations because of: 1. Potency. 2. Cost-effectiveness. 3. Lack of foreign protein antigenicity. 4. Ease of dosing.")
89
T₃ (t ⅟₂=1.5d): * May be used for short-term replacement. *NOT recommended for routine Tx due to its: 1. Cardiotoxic effect 2. Multiple daily dosing 3. Greater difficulty in monitoring therapeutic & toxic responses. 4. High cost

90
3) T₃+T₄ Combination: Needs to be further investigated 4) Dessicated Thyroid from Animals: Considered obsolete although inexpensive due to allergic reactions & abnormal TFTs.

91
Special Treatment Issues:
Congenital Hypothyroidism: *The earlier the Tx begins, the better the prognosis of mental & growth development. *DOC: L-thyroxine *Infants w/ long standing & severe myxedema: Extremely sensitive to minute doses of TH *Start w/ very small doses (tab.38.11) to prevent toxicity. * TSH should normalize after 3-4months of starting Tx.
 to prevent. toxicity. * TSH should normalize after 3-4months of starting Tx.")
92
2) Subclinical Hypothyroidism:
*Treatment: Debatable *Not all cases progress to hypothyroidism: Higher TSH elevation , greater risk *Risk is greatest w/ TSH > 10mIU/L *Decision to treat is based on: Risk vs. benefit of Tx Likelihood of overt hypothyroid (hx RAI or surgery) Degree of TSH elevation Hx of thyroid dz.
 Degree of TSH elevation. Hx of thyroid dz.")
93
3) Myxedema Coma: Hormone replacement + Supportive measures
c. Eliminate or correct precipitating factors

94
a. Hormone Replacement:
L-thyroxine: Large IV dose ( mcg) then M.D mcg IV QD until p.o. is possible. Hydrcortisone: mg IV Q6H: To prevent adrenal crisis in case of undetected hypopituitarism exists.
 then M.D mcg IV QD. until p.o. is possible. Hydrcortisone: mg IV Q6H: To prevent adrenal crisis in case of undetected. hypopituitarism exists.")
95
b. Supportive Measures: 1. Assisted ventilation 2
b. Supportive Measures: 1. Assisted ventilation 2. Glucose infusion for hypoglycemia 3. Fluid restriction due to hyponatremia 4. Plasma expanders for shock & circulatory collapse **Heating blankets: NOT recommended because it can aggrevate shock by vasodilation. c. Eliminate or Correct Precipitating Factors ** If properly treated, Recovery can occur w/in 24 hrs.

Similar presentations
















,Triiodothyronine T3 (9%) and rT3 (1%). Reverse T3 (rT3) is biologically inactive.>")









 55 F Graves’ disease diagnosed at 彰基 one year ago Initial presentation: sweating, good appetite, easy nervousness Physical.>")


 is an acute state of hyperthyroidism where all of the signs and symptoms are exaggerated.>")

BB>")


 2. Siti Hadijah (14700108) 3. I Putu Adi Styawan (14700120) 4. Jaka Primadhana. R (14700132)>")