Download presentation
Presentation is loading. Please wait.

1
Managing patients with chronic viral hepatitis who need renal replacement therapy. Thursday 5 th February Dr Allister Grant Leicester Liver Unit

2
Hepatitis and Dialysis Hepatitis epidemiology Vaccination Natural history Suitability for transplantation Antiviral treatment Hepatitis-positive donors

3
Outbreak Date Patient cases Contacts cases Staff casesTotal cases Patient death Staff death Total death Manchester 1965/66 5 - 11 16 - 3 3 Liverpool 1966/71 15 7 3355 - - - Charing Cross I 1966/67 15 - - - - - Charing Cross II 1968/71 64 - 1 65 - - - Birmingham 1967/71 21 4 12 37 - - - Newcastle 1969/71 4 1 - 5 1 - 1 Royal Free 1969/70 3 - 8 11 - - - Hammersmith I 1969/70 6 - 1 7 3 - 3 Hammersmith II 1971 6 - 2 8 - - - Edinburgh 1969/71 18 2 8 28 8 3 11 Guys 1969/71 33 14 42 89 - - - Cardiff 1969/71 16 1 4 21 - - - TOTAL: 206 29 122 357 12 6 18 The horror of HBV in dialysis units! From the website of the Renal Unit of the Royal Infirmary of Edinburgh “In April 1969, a CRF patient was transfused with one unit of blood that was incubating hepatitis.”

4
Rosenheim Report 1972 Guidelines for prevention and control of HBV in renal dialysis and transplantation units.

5
Basic barrier precautions against exposure to blood Segregation of infected patients (from susceptible patients) dedicated machines dedicated area or room dedicated staff for any shift exclusion of HBsAg-positive staff Regular screening of patients and staff for infection monthly testing of susceptible patients
 dedicated machines dedicated area or room dedicated staff for any shift exclusion of HBsAg-positive staff Regular screening of patients and staff for infection monthly testing of susceptible patients")
6
1972 universal precautions, screening and segregation % HBsAg-positivity in patients and staff ‘76 7.8.5 ‘82‘80 3.8 5.2 2.6.5 screening of blood for HBsAg 1972

7
Rosenheim Report 1972 Guidelines for prevention and control of HBV in renal dialysis and transplantation units. Basic barrier precautions against exposure to blood Segregation of infected patients (from susceptible patients) dedicated machines dedicated area or room dedicated staff for any shift exclusion of HBsAg-positive staff Regular screening of patients and staff for infection monthly testing of susceptible patients Then (since ’82) introduction of vaccination for staff and patients (and carers)
 dedicated machines dedicated area or room dedicated staff for any shift exclusion of HBsAg-positive staff Regular screening of patients and staff for infection monthly testing of susceptible patients Then (since ’82) introduction of vaccination for staff and patients (and carers).")
8
1972 universal precautions, screening and segregation HBV vaccination of patients & staff 1982 % HBsAg-positivity in patients and staff ‘76 7.8.5 ‘82‘80 3.8 ‘99 <1% EPO CAPD & home dialysis 5.2 2.6.5 0 1986 screening of blood for HBsAg 1972

9
universal precautions, screening and segregation HBV vaccination of patients & staff 1982 EPO CAPD & home dialysis 1986 screening of blood for HBsAg 1972 Reducing the Risk for HCV Transmission

10
1972 universal precautions, screening and segregation HBV vaccination of patients & staff 1982 EPO CAPD & home dialysis 1986 screening of blood for HBsAg 1972 screening of blood for HCV 1991 Reducing the Risk for HCV Transmission

11
Prevalence of BBV infections in UK renal patients (postal survey 1996) HBsAg-positiveHCV-positive Maintenance HD (hospital) 0.53%2.2% Maintenance PD0.54%1.1% Functioning renal transplant 0.20%0.74% Chronic renal disease 0.13%0.04% Maintenance HD (home) 0.09%0.47%
 HBsAg-positiveHCV-positive Maintenance HD (hospital) 0.53%2.2% Maintenance PD0.54%1.1% Functioning renal transplant 0.20%0.74% Chronic renal disease 0.13%0.04% Maintenance HD (home) 0.09%0.47%")
12
HCV Infection in HD Patients Jadoul et al Nephrol Dial Transplant 2004;19:904-9.

13
Hepatitis and Dialysis Hepatitis epidemiology for HBV and HCV locally & globally relevance to dialysis

14
The Stages of Chronic HBV Infection immune tolerance immune clearance inactive carrier reactivation HBeAg Anti-HBe HBV-DNA ALT

15
HBeAg positive HBeAg negative Giusti et al, Giusti et al, 1991 1975-85: 539 patients Prevalence of HBeAg Negative Chronic HBV in Italy 58% 42% Gaeta et al, 2003 2001: 837 patients 10% 90%

18
Where do carriers come from? Acute infection Chronic infection “carrier” <5% risk

19
Where do carriers come from? Acute infection Chronic infection “carrier” <5% risk “carrier” from abroad

20
New chronic infections in England & Wales (per annum) Arising in E & W n = 216 (3%) Coming from abroad n = 6,571 (97%) Transmission of HBV in England & Wales Hahné et al J Clin Virol 2004;29:211-220.
 Arising in E & W n = 216 (3%) Coming from abroad n = 6,571 (97%) Transmission of HBV in England & Wales Hahné et al J Clin Virol 2004;29:")
21
HBV Notifications in England & Wales

22
QE Hepatitis Database 2005/6 Hepatitis B

23
QE Hepatitis Database 2005/6 Ethnicity of HBV Patients

24
QE Renal Database Ethnicity of HBV patients (17/850 = 2%)
")
25
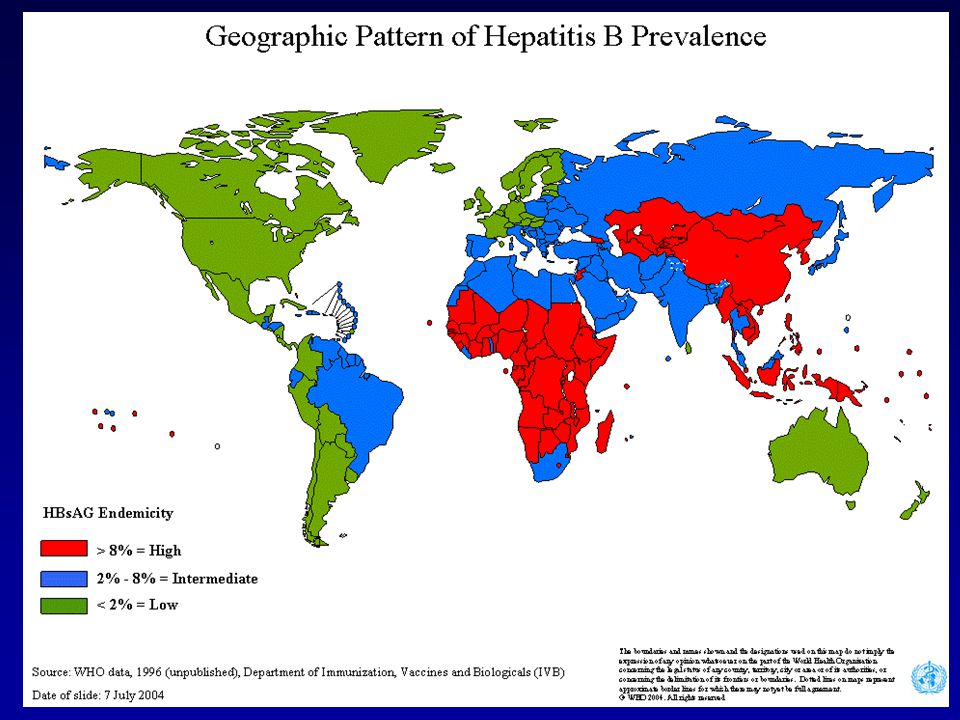
Prevalence of Hepatitis C virus 2001 WHO

26
UK HCV Prevalence <1% IV Drug Use Migration Blood Donation 200,000 Screening 1991

27
HCV- Natural History 100 Infected 20% at 20yrs 50% at 30yrs Age Gender Alcohol 20 Clear the HCV 80 Develop Chronic Hepatitis 20 No Harmful Effects 60 Signs/symptoms CIRRHOSIS Transplantation Liver Failure Liver Cancer 3.9% pa 1.4% pa

28
QE Hepatitis Database 2005/6 Hepatitis C

30
QE Renal Database Ethnicity of HCV patients (23/850 = 2%)
")
31
HBV Vaccination for Renal Patients Complex immunological defect asymptomatic acute infection high risk for chronic infection after exposure low serum transaminases Poor response to HBV vaccination poor seroconversion rate (60%) despite augmented protocols correlates with creatinine clearance low titre antibodies in responders rapid decline in antibody titre need for regular measurement & boosters (anti-s < 10 IU/l)
 despite augmented protocols correlates with creatinine clearance low titre antibodies in responders rapid decline in antibody titre need for regular measurement & boosters (anti-s < 10 IU/l)")
32
Vaccination in End-stage Renal Disease Bel’eed et al Postgrad Med J 2002;78:538-40.

33
QE Birmingham Renal Unit Audit 2003 (862 patients with ESRF)
")
34
Vaccination in End-stage Renal Disease Bel’eed et al Postgrad Med J 2002;78:538-40.

35
Hepatitis and Dialysis Hepatitis epidemiology Vaccination Natural history

36
Hepatitis & Renal Failure Natural History all causes mortality is high long natural history of chronic hepatitis ? hepatitis-associated mortality independent of liver disease (for HCV) modified by antiviral treatment for HBV publications outdated all causes hepatitis liver disease DIALYSIS
 modified by antiviral treatment for HBV publications outdated all causes hepatitis liver disease DIALYSIS.")
37
Impact of HCV on Survival of HD Patients Espinosa et al Nephrol Dial Transplant 2001;16:1669-74. 175 patients 57 anti HCV-positive Independent predictors of survival baseline age (RR 1.04) diabetic aetiology (3.6) transplantation during f-up (0.66) HCV-positivity (1.62) Kaplan-Meier survival 52% at 8 years for HCV-negative 32% at 8years for HCV-positive Causes of death similar except 4 HCV-pos died of liver disease (vs 0 HCV-negs)
 diabetic aetiology (3.6) transplantation during f-up (0.66) HCV-positivity (1.62) Kaplan-Meier survival 52% at 8 years for HCV-negative 32% at 8years for HCV-positive Causes of death similar except 4 HCV-pos died of liver disease (vs 0 HCV-negs).")
38
Impact of HCV on Survival of HD Patients Espinosa et al Nephrol Dial Transplant 2001;16:1669-74. 175 patients 57 anti HCV-positive Independent predictors of survival baseline age (RR 1.04) diabetic aetiology (3.6) transplantation during f-up (0.66) HCV-positivity (1.62) Kaplan-Meier survival 52% at 8 years for HCV-negative 32% at 8years for HCV-positive Causes of death similar except 4 HCV-pos died of liver disease (vs 0 HCV-negs) Confirmed in meta-analysis. Fabrizi et al Aliment Pharmacol Ther 2004;20:1271-7.
 diabetic aetiology (3.6) transplantation during f-up (0.66) HCV-positivity (1.62) Kaplan-Meier survival 52% at 8 years for HCV-negative 32% at 8years for HCV-positive Causes of death similar except 4 HCV-pos died of liver disease (vs 0 HCV-negs) Confirmed in meta-analysis. Fabrizi et al Aliment Pharmacol Ther 2004;20:")
39
HBV & HCV and Post-Renal Transplant Outcome Mathurin et al Hepatology 1999;29:257-63.

41
Liver Biopsy Scoring System Ishak et al. J Hepatology 1995;22:696. GradingScore Periportal hepatitis0-4 Confluent necrosis0-6 Spotty necrosis0-4 Portal inflammation0-4 0-18 Staging (fibrosis)0-6
0-6.")
42
liver fibrosis score (degree of scarring) 0 6 3 years 10 2030 60 cirrhosis
 years cirrhosis")
43
liver fibrosis score (degree of scarring) 0 6 3 years 10 2030 60 cirrhosis HCV-pos (median time 38 years)
 years cirrhosis HCV-pos (median time 38 years)")
44
liver fibrosis score (degree of scarring) 0 6 3 years 10 2030 60 cirrhosis ? end-stage renal disease

45
liver fibrosis score (degree of scarring) 0 6 3 years 10 2030 60 cirrhosis end-stage renal disease ? immune suppression

46
Hepatitis and Dialysis Hepatitis epidemiology Vaccination Natural history Suitability for transplantation?

47
Suitability for Kidney Transplantation Accurate assessment of stage is there advanced fibrosis or cirrhosis? What is the prognosis of the liver disease with versus without immunosuppression? Can prognosis be influenced by antivirals? before and/or after transplantation Is or will combined liver and kidney transplantation be feasible or appropriate? liver units are fussy!

48
Suitability for Kidney Transplantation Accurate assessment of stage is there advanced fibrosis or cirrhosis? What is the prognosis of the liver disease with versus without immunosuppression? Can prognosis be influenced by antivirals? before and/or after transplantation Is or will combined liver and kidney transplantation be feasible or appropriate? liver units are fussy!

49
Antiviral Therapy HBV Aim is suppression of replication rarely elimination HIV treatment paradigm suppression prevents disease Indefinite treatment ? lifelong Treatment well tolerated

50
Antiviral Therapy HBV Aim is suppression of replication rarely elimination HIV treatment paradigm suppression prevents disease Indefinite treatment ? lifelong Treatment well tolerated HCV Aim is viral eradication Treatment of finite duration Treatment is poorly tolerated particularly in renal patients

51
Antiviral Therapy For HBV is Evolving Approved Drugs –Conventional Interferons (IFNs) –Lamivudine (LMV) –Adefovir (ADV) –Pegylated Interferon a-2a (PEG-IFN) –Entecavir (ETV) –Tenofovir (TDF) Future Options –Telbivudine (LdT) X –Clevudine –Pradefovir –Emtricitabine ? –Valtorcitabine –etc………….. Monotherapy Sequential therapy Combination therapy

52
HBV (DNA) HEPATOCYTE NUCLEUS DNA reverse transcription transcription DNA RNA
 HEPATOCYTE NUCLEUS DNA reverse transcription transcription DNA RNA")
53
HBV (DNA) HEPATOCYTE NUCLEUS DNA reverse transcription transcription DNA RNA inhibited by nucleoside/tide analogues
 HEPATOCYTE NUCLEUS DNA reverse transcription transcription DNA RNA inhibited by nucleoside/tide analogues")
54
HBV Viral Replication and Mutational Frequency High virion production: 10 12-13 virions per day Wild-type HBV Pol lacks proof-reading function 10 10-11 point mutations produced per day All possible single base changes can be produced per day Single / double mutations pre-exist in HBV from patients prior to therapy: WHY MOST MONOTHERAPIES FAIL Triple / quadruple mutations require replication in the presence of selection pressure and rarely pre-exist: WHY COMBINATION TREATMENT WORKS (Colgrone & Japour. 1999. AVR. 41:45)
.")
55
Treatment of lamivudine-resistant HBV adefovir lamivudine

56
Lamivudine Entecavir Clevudine Emtricitabine Adefovir

57
Extended LAM therapy in HBeAg(-) CHB: The Italian experience (616 patients) Major clinical events under therapy (Hepatitic flares, decompensation,HCC, transplantation, death) Non-cirrhotics: 6.5% Cirrhosis Child. A:31% Cirrhosis Child B-C: 86% Di Marco V for AISF Lamivudine Study Group, Hepatology. 2004; 40: 883-91

58
HBV Treatment in Renal Failure Creat clearance Lamivudine (mg per day) > 50100 30-5050 15-3025 5-1515 <510 Creat clearance Adefovir > 5010 mg daily 20-50 10 mg every other day 10-20 10 mg every 3 rd day HD 10mg wkly post-HD Creat clearance Tenofovir > 50245 mg daily 30-50 245 mg every other day 10-20 245 mg every 3 rd day HD 245mg wkly post-HD
 > <510 Creat clearance Adefovir > 5010 mg daily mg every other day mg every 3 rd day HD 10mg wkly post-HD Creat clearance Tenofovir > mg daily mg every other day mg every 3 rd day HD 245mg wkly post-HD")
59
HCV Antiviral Treatment IFN Pegylated IFN IFN & ribavirin Peg-IFN & ribavirin efficacy tolerability

60
HCV Genotypes 6 main genotypes Nucleotide diversity > 20% Little effect on natural history Geographical variation Most important determinant of response to treatment

61
Peg-IFN & Ribavirin (normal renal function)
")
62
Pegylated IFN & Ribavirin for HD Patients Bruchfeld et al Journal of Viral Hepatitis 2006;13:316-21. HCV genotype type/dose of peg-IFN ribavirin dose (g/week) HCV negative (week) Treatment duration outcome 112b 50µg1.81248cured 212b 50µg1.21248failed 342b 50µg1.4510died 412b 50µg1.424 failed 512a 135µg1.41236cured 622a 135µg2.01224cured
 HCV negative (week) Treatment duration outcome 112b 50µg cured 212b 50µg failed 342b 50µg1.4510died 412b 50µg1.424 failed 512a 135µg cured 622a 135µg cured.")
63
Caucasian QE Hepatitis Database 2005/6 Hepatitis C genotype

64
Asian QE Hepatitis Database 2005/6 Hepatitis C genotype

65
Suitability for Kidney Transplantation Accurate assessment of stage is there advanced fibrosis or cirrhosis? What is the prognosis of the liver disease with versus without immunosuppression? Can prognosis be influenced by antivirals? before and/or after transplantation Is or will combined liver and kidney transplantation be feasible or appropriate? liver units are fussy!

66
Hepatitis and Dialysis Hepatitis epidemiology Vaccination Natural history Suitability for transplantation Antiviral treatment Hepatitis-positive donors

67
UK Transplant Data 2002 - 2004 Liver donor HBsAg, core antibody or HCV positivity 200220032004 Number of donors646560616 HBsAg-pos000 Core antibody-pos (HBsAg-neg) 11(1.5%)7(1.1%)18(2.4%) HCV-pos7(1%)2(0.3%)4(0.5%)
 11(1.5%)7(1.1%)18(2.4%) HCV-pos7(1%)2(0.3%)4(0.5%)")
68
HBV core antibody positive organ donation organ donors who have past HBV infection now immune (HBsAg-negative/core antibody positive) ? risk of HBV transmission risk is very high for liver recipients modified by recipient HBV immunity lamivudine prophylaxis justified

69
Core antibody positive kidney donation Fabrizi et al J Nephrology 2002;15:605-13. Number of recipients of core-positive kidney HBsAg seroconversion Wachs421 Krieger191 Satterthwaite380 Fong7632 Kadian190 Madayag450 9264 (0.4%)
.")
70
HBV core antibody positive organ donation organ donors who have past HBV infection now immune (HBsAg-negative/core antibody positive) ? risk of HBV transmission risk is very high for liver recipients modified by recipient HBV immunity lamivudine prophylaxis justified risk is very low for kidney recipients HBV immune recipient any recipient lamivudine prophylaxis probably not justified

71
Hepatitis and Dialysis Hepatitis epidemiology global village Natural history greater impact in transplantation than in dialysis hepatitis B data may become outdated Suitability for transplantation beware of the cirrhotic (particularly HCV) Antiviral treatment well tolerated and effective for HBV poorly tolerated for HCV (but promise!) Hepatitis-positive donors HBV core antibody positivity is ok (for anyone) HCV-positive donors for HCV-positive recipients
 Antiviral treatment well tolerated and effective for HBV poorly tolerated for HCV (but promise!) Hepatitis-positive donors HBV core antibody positivity is ok (for anyone) HCV-positive donors for HCV-positive recipients")
Similar presentations









 Infection Hepatitis C Virus (HCV) Infection.>")


, ABIM Gastoenterologist King Abdulaziz University Hospital.>")









