Download presentation
Presentation is loading. Please wait.

1
Fetal Alcohol Syndrome Manish Saran MD Department of Psychiatry Louisiana State University Health Sciences Center Shreveport February 8, 2006

2
Historical view of alcohol as a teratogen Foolish, drunken, or harebrain women most often bring forth children like unto themselves Aristotle in Problemata Behold, thou shalt conceive and bear a son: And now, drink no wine or strong drink. Judges 13:7 Judges 13:7

3
Some Facts 60% of adult women drink 4% abuse or are dependent 20% of pregnant women drink 3% heavy drinkers 3% heavy drinkers 5.5% illegal drugs, 0.9%cocaine

4
Fetal alcohol syndrome FAS is a developmental disability caused by prenatal exposure to high levels of ETOH Most common preventable cause of adverse CNS development The reported prevalence of the disorder varies widely, estimates approach 1% of live births 4,000-12,000 infants per year in US The disorder is identified by the presence of growth impairment, central nervous system dysfunction, and a characteristic pattern of craniofacial features

5
Facies in Fetal Alcohol Syndrome

6
Adult Facies

7
Fetal Alcohol Effects Only a minority (10-40%) of the children of chronic alcoholic women are diagnosed with FAS Fetal Alcohol Effects (FAE): individuals lack the outward physical appearance of alcohol damage, and generally have higher IQ's 7,000-36,000 infants per year in US The internal damage to the brain and other organs can be just as serious
 of the children of chronic alcoholic women are diagnosed with FAS Fetal Alcohol Effects (FAE): individuals lack the outward physical appearance of alcohol damage, and generally have higher IQ s 7,000-36,000 infants per year in US The internal damage to the brain and other organs can be just as serious")
8
Fetal Alcohol Spectrum Disorders category 1 FAS with confirmed maternal ETOH exposure category 2 FAS without confirmed maternal ETOH exposure category 3 partial FAS with confirmed maternal ETOH exposure category 4 ARBD (alcohol -related birth defects), (physical only) category 5 ARND (alcohol -related neurodevelopmental disorder)
, (physical only) category 5 ARND (alcohol -related neurodevelopmental disorder)")
9
Co morbid Conditions attention deficit hyperactivity disorder (40%) mental retardation (15–20%) learning disorders (25%) speech and language disorders (30%), sensory impairment (30%) cerebral palsy (4%) epilepsy (8–10%).
 mental retardation (15–20%) learning disorders (25%) speech and language disorders (30%), sensory impairment (30%) cerebral palsy (4%) epilepsy (8–10%).")
10
Brain damage The brain on the right suffers from microencephaly and migration anomalies (neural and glia cells did not migrate to their proper location in the brain, but instead many of them simply migrated to the top of the cortex). Although it cannot be seen here, there is also agenesis of the corpus callosum and the ventricles are dilated.

11
General Intellectual Performance FSIQVIQPIQ 40 55 70 85 100 115 Standard score IQ scale * * * ** * * Prenatal Exposure to Alcohol Fetal Alcohol Syndrome Normal control

12
Neuropsychological Performance

13
2 1 3 1 2 3 Group 0 2 4 6 Rule Violations NC PEA FAS P<0.001 Move only one piece at a time using one hand and never place a big piece on top of a little piece Starting position Ending position Mattson, et al., 1999 Executive functioning deficits

14
Secondary Disabilities

15
Risk Factors Dose of alcohol the higher the dose of alcohol, the greater the likelihood that the child will exhibit fetal alcohol effects the higher the dose of alcohol, the greater the likelihood that the child will exhibit fetal alcohol effects Pattern of exposure - binge vs chronic Both human and animal studies have found that binge drinking (drinking a large amount of alcohol in a short period of time), which produces high blood alcohol levels, is more damaging to the fetus than chronic alcohol exposure that produces lower blood alcohol levels. Both human and animal studies have found that binge drinking (drinking a large amount of alcohol in a short period of time), which produces high blood alcohol levels, is more damaging to the fetus than chronic alcohol exposure that produces lower blood alcohol levels.
, which produces high blood alcohol levels, is more damaging to the fetus than chronic alcohol exposure that produces lower blood alcohol levels..")
16
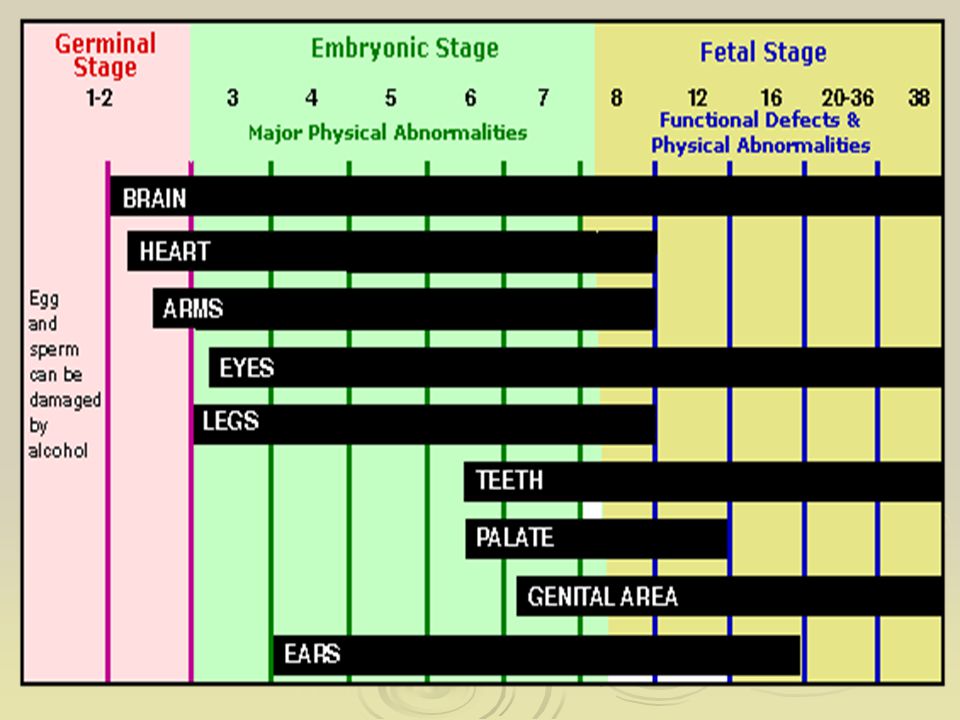
Risk Factors Developmental timing of exposure the facial features associated with prenatal alcohol treatment appear to be related to alcohol exposure during the first trimester the facial features associated with prenatal alcohol treatment appear to be related to alcohol exposure during the first trimester The brain undergoes a very prolonged developmental course and therefore, may be susceptible to fetal alcohol effects throughout gestation The brain undergoes a very prolonged developmental course and therefore, may be susceptible to fetal alcohol effects throughout gestation Genetic variation Maternal characteristics Synergistic reactions with other drugs Nutrition

17
Treatment and Prevention Very little research done on these topics Many children with FAS treated for their individual symptoms (e.g. stimulants for ADHD) Animal data indicates that early intervention with environmental variables might have a beneficial effect such as motor training Public education may not be reaching the women most likely to have a child with FAS Intensive, case-management approaches appear to work very well.
 Animal data indicates that early intervention with environmental variables might have a beneficial effect such as motor training Public education may not be reaching the women most likely to have a child with FAS Intensive, case-management approaches appear to work very well..")
18
Prevention – The Birth to 3 Program Parent-child assistance program Intensive home visitation model for the highest risk mothers Paraprofessional Advocates Paired with client for 3 years following the birth of the target Baby Link clients with community services Extensively trained and closely supervised Maximum caseload of 15 Outcomes Fewer alcohol/drug affected children Reduced foster care placement Reduced dependence on welfare

19
Ethnic Considerations Rate of FAS (per 1000; 1980-1986) Native Americans 2.97 Native Americans 2.97 African Americans 0.6 African Americans 0.6 Caucasians 0.09 Caucasians 0.09 Hispanics 0.08 Hispanics 0.08 Asians 0.03 Asians 0.03
 Native Americans 2.97 Native Americans 2.97 African Americans 0.6 African Americans 0.6 Caucasians 0.09 Caucasians 0.09 Hispanics 0.08 Hispanics 0.08 Asians 0.03 Asians 0.03")
20
Summary Fetal Alcohol Syndrome is a devastating developmental disorder that affects children born to women who abuse alcohol during pregnancy. Although FAS is entirely preventable, and in spite of our increasing knowledge about the effects of prenatal alcohol exposure, children continue to be born exposed to high amounts of alcohol. Its consequences affect the individual, the family, and society. Its costs are tremendous, both personally and financially. Effective treatment and prevention strategies must be developed and made available.

21
Discussion/ Questions

Similar presentations

 EUROPEAN PARLIAMENT STRASBOURGH, TUESDAY SEPTEMBER 4 TH 2007 Dr. Kieran D. O’ Malley MB,BAO,BCH, DABPN Consultant.>")






>")

 TLSE 240 Presentation For:>")

 Reducing alcohol-related harm through a nonjudgmental approach Dr. Samuel Harper.>")



>")



