Download presentation
Presentation is loading. Please wait.

1
Final Med. Orthopaedics
Mr. James Harty

2
A fracture is a break or interruption in the continuity of a bone

3
Anatomical Bone involved Part of bone involved Radius, femur
Diaphysis, metaphysis neck/shaft/head

4
Direction of Fracture Line
Transverse Oblique Spiral

5
All fractures are either UNDISPLACED or DISPLACED the deformity of the fracture

6
All fractures are either CLOSED or OPEN
A communication between the fracture site and the skin surface (Compound)
")
9
All fractures are either SIMPLE or COMMINUTED
More than two fragments (>1 fracture line)
")
12
A fracture occurring in a bone weakened by disease
Often refers to a fracture occuring in a bony secondary

13
A fracture occurring in immature bone
Cortex bends rather than breaks

14
Classified by Salter-Harris Types I-V
Type II is commonest

15
Type II fracture distal radius

16
“Look, Feel, Move” Pain, tenderness Swelling… bruising Loss of function Crepitus Signs of blood loss Injury to other structures

17
History Examination X-ray Isotope Bone Scan Specialised Imaging C.T.
M.R.I.

18
Two planes Two joints Two occasions Two limbs Two opinions

19
Two planes Two joints Two occasions Two limbs Two opinions
AP and Lateral +/- special views e.g. scaphoid Two planes Two joints Two occasions Two limbs Two opinions

20
Two planes Two joints Two occasions Two limbs Two opinions
Joint above and below for shaft fractures Two planes Two joints Two occasions Two limbs Two opinions

21
Two planes Two joints Two occasions Two limbs Two opinions
Repeat X-rays after an interval may show a fracture e.g. scaphoid, hip

22
Two planes Two joints Two occasions Two limbs Two opinions
Comparative views of opposite limb e.g. elbow injuries in children

23
Two planes Two joints Two occasions Two limbs Two opinions
Ask a radiologist or senior colleague!

24
haematoma inflammatory exudate new blood vessels (2-3 days) bone forming cells bridge of callus (cartilage, bone, fibrous tissue) framework for bridging the gap replaced by woven bone remodelling along lines of stress

25
callus is the response to movement at fracture site
callus does not develop if the fracture is rigidly fixed with no movement: primary bone healing

26
Depends on many factors
age bone type of fracture infection nutrition stimulation

27
Full assessment Reduction Immobilisation Maintenance of reduction Rehabilitation

28
restoring “normal” anatomy not always necessary open/closed
anaesthesia local/regional/general

29
general rule: joint above and joint below splints, plaster, braces
for shaft fractures splints, plaster, braces internal fixation plates, screws, wires, intramedullary rods external fixation traction

30
maintain until united check x-rays clinical and radiological evidence of union

31
starts A.S.A.P. keep non-immobilised joints mobile avoid muscle wasting physiotherapy

32
Open Fractures problem: infection
prophylactic antibiotics appropriate to the injury anti-tetanus cover irrigation “the solution to pollution is dilution” debridement: remove all dead tissue skin cover

33
non-union/delayed union
multiple fractures pathological fractures fractures likely to slip intra-articular fractures nursing difficulties

34
Initial Treatment Initial treatment – splinting and analgesia. Compound injuries – Antibiotic cover (usually cephalosporin +/- aminoglycoside if contaminated). -Tetanus cover.
. -Tetanus cover.")
35
Further Treatment Compound injuries must be debrided ASAP, should be within 6 hours. Bone should be covered with tissue to prevent dessication. Delayed primary closure of the wound, or “second look” procedure.

36
Treatment Aims – obtain union, maintain relative positions of knee and ankle joints. Treatment options include: Conservative. Open Reduction and Internal Fixation. Intra medullary nailing. External fixation.

37
Conservative Treatment
Casting may be considered if: Isolated tibial fracture (fibula not involved). >50% cortical overlap at # site. Closed reduction of displaced #’s and casting leads to significant incidence of non-union. Less than 2cm initial shortening.
. >50% cortical overlap at # site. Closed reduction of displaced #’s and casting leads to significant incidence of non-union. Less than 2cm initial shortening.")
38
ORIF Usually used for intra–articular #’s involving knee or ankle rather than shaft #’s. Periosteal stripping required. Fracture site must be opened. May be useful in Rx of non-union +/- bone grafting.

40
Nailing Probably preferred Rx of closed displaced tibial shaft fractures. Union rates of near 100% for closed injuries. Fracture site not opened during the procedure, reduced chance of infection. More difficult in proximal shaft fractures.

42
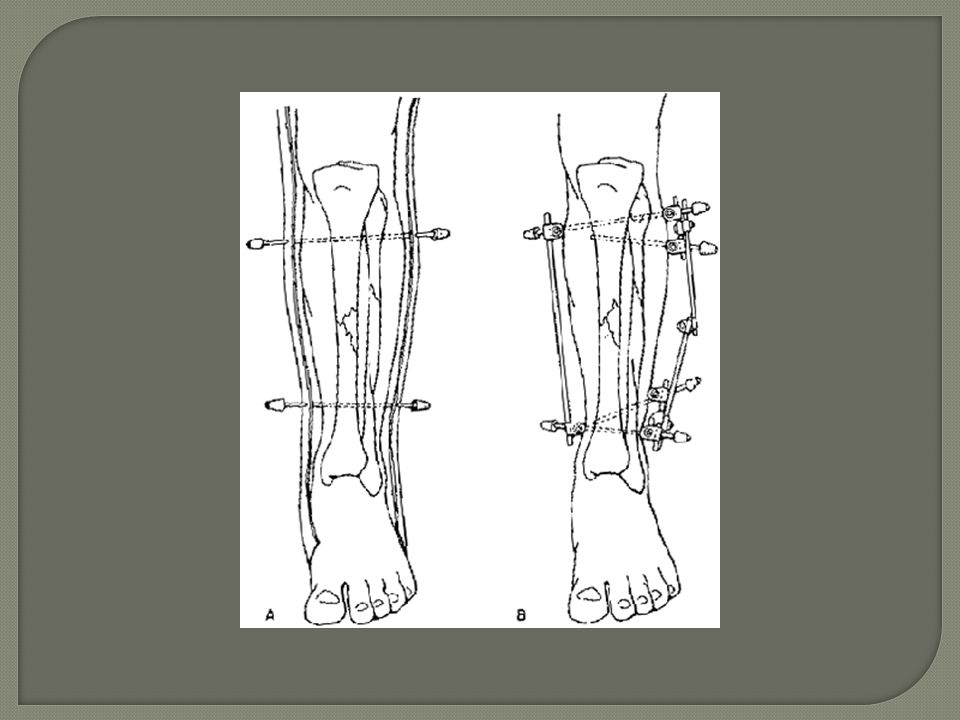
External Fixation Minimal soft tissue trauma.
Little foreign material in body, may be preferred in compound fractures. Comminuted injuries. Uniplanar, circular or combination of both (hybrid) fixators.
 fixators.")
45
Complications Compartment syndrome.
Pressure in muscular compartments rises above capillary pressure, ischaemia of tissues in affected compartment. Patients complain of pain unrelieved by splinting and analgesia.

46
Compartment Syndrome Pain on passive stretching is classic physical sign. Normal distal pulses and neurology DO NOT exclude compartment syndrome. Incidence NOT reduced in compound fractures (up to 9%). ? May complicate nailing of fracture.
. May complicate nailing of fracture.")
47
Union delayed union non-union atrophic hypertrophic infected mal-union

48
skin compound wounds fracture blisters plaster sores pressure sores

49
muscle/tendon disuse, wasting avulsion
late rupture (e.g. EPL, Colles’ fracture)
")
50
haemorrhage thrombosis/embolism pelvis 6-8 units (hidden)
femur 3-4 units hip 1-2 units thrombosis/embolism esp. pelvic and hip fractures

51
infection growth disturbance stiffness local (compound or operated)
respiratory urinary tract growth disturbance epiphyseal fractures stiffness keep non-injured joints mobile

52
neighbouring structures
nerves vessels internal organs

53
Fractured Neck of Femur
Subcapital Femoral Fracture. Over 100,000/year in the UK

54
Key Points Common in osteoporotic bone.
Majority of blood supply to head comes from the neck. Elderly. Almost 90% occur in >65 years. Almost 75% occur in females.

55
Hip Joint - Anatomy The fibres are reflected back along the neck of the femur to the articular margin of the femoral head. The reflected part constitutes the retinacular fibres, which bind down the nutrient arteries from the trochanteric anastomosis, along the neck to supply the head.

56
About the blood supply The head and intracapsular part of the neck receive blood from the trochanteric anastomosis. Formed by descending superior gluteal artery with ascending branches of the medial and lateral circumflex femoral arteries. Branches pass along the femoral neck with the retinacular fibres of the capsule.

57
Anatomy – Blood Supply

58
Fractures Traumatic fracture Pathological fracture

59
Clinical Features Severe hip pain associated with a fall.
Unable to weight-bear. Shortened and externally rotated leg AP/Lateral hip required. Older – co-morbidity.

60
Garden 1 fractured neck femur
RS Garden, Preston Royal Infirmary, JBJS 1961

61
Garden 2

62
Garden 3

63
Garden 4

64
Complications Avascular necrosis of femoral head
Blood supply lost through thrombosis or interrossoeus hypertension. Marrow of head is replaced by fat, bone dies. Zone of revascularisation, incomplete if large avascular area. Zone of reossification – joint may collapse. May -> secondary arthritis.

65
Complications Avascular necrosis of femoral head
X-rays – may appear normal. Radioisotope – dead area of femoral head surrounded by hyperaemic area of revascularisation. MRI – one or more avascular areas.

66
Initial Management ATLS principals of resuscitation Co-morbidity
Work-up for theatre Relevant Radiology - Diagnosis Decide surgical/anaesthetic management Informed Consent Prophylactic Antibiotics Anticoagulation Early Mobilization Discharge arrangements

67
Surgical Treatment Age and displacement Co-Morbidity
Undisplaced (Garden 1 & 2): 1. Cannulated Hip Screws. 2. DHS. 3. Hemi-Arthroplasty Displaced (Garden 3 & 4): 1. Hemi-Arthroplasty. 2. Total Hip Replacement occasionally if pre-existing OA.
: 1. Cannulated Hip Screws. 2. DHS. 3. Hemi-Arthroplasty. Displaced (Garden 3 & 4): 1. Hemi-Arthroplasty. 2. Total Hip Replacement occasionally if pre-existing OA.")
68
Garden 1 - Treatment AO Screws to hold femoral head in position
Indications for Closed Reduction and Fixation: Physiologically young patient: age < 65, working patient, good bone stock; Demented elderly patient that requires total care; Adequate closed reduction with no comminution or femoral neck defects; Patient should be aware that with an inadequate closed reduction, then an open reduction or hemiarthroplasty will be required

69
Garden 2-3 Older patients – Hemiarthroplasty
Especially in Life Expectancy<5 years One definitive operation. Fractures may progressively displace.

70
DHS - Richards Undisplaced Garden 1+2 – no vascular disruption
Lateral Approach X-ray control First part is a heavy plate fixed to lateral cortex of femur with cortical screws. Second part is a rod which passes into the femoral head. The threaded end crosses the fracture line to engage and hold the fracture line. As the patient weight bears on the healing fracture the broken ends of the bone collapse into each other and compress the fracture. The sliding-rod mechanism allows this to happen without the hip falling into varus.

71
Complications Avascular Necrosis Non-Union General DVT/PE Infection
Ulcers Anaemia

72
Garden 4 Femoral Head survival unlikely.
Under fifty – reduce and pin immediately. Older: <65 THR >65 Hemiarthroplasty

73
Treatment – Hemiarthroplasty
Austin Talley Moore, MD South Carolina In September 1940, Austin Tally Moore and Harold Ray Bohlman, replaced the proximal 12 inches of a femur destroyed by a recurrent giant cell tumor with a custom-made prosthesis, Dr. Moore was encouraged to develop a new femoral head with a short stem for intramedullary fixation, and, the now legendary Austin Moore Hip was introduced in 1950. Cemented Frederick Roeck Thompson, MD Texas Son of the renowned reconstructive surgeon Dr. James E. Thompson of the University of Texas Medical Branch, Frederick R. Thompson, MD, designed - one of the first metal hips for use in hip fractures and salvage arthroplasties. The first F.R. Thompson Hip was implanted in January 1951, and is still in worldwide use today. Uncemented

74
Indications – AMP/Thompson
Poor general health that would prevent a second operation; pathologic hip fractures Parkinson's disease, hemiplegia, or other neurological disease; Physiologic age > 70 yrs; Severe osteoporosis without loss of primary trabeclae in femoral head Inadequate closed reduction; Displaced fracture which is several days old; Pre-existing hip disease (DJD, RA, AVN); Contraindications: Pre-existing sepsis Young patient Failure of internal fixation devices; Pre-existing disease of the acetabulum; Even without normal preoperative cartilagenous space, many patients will become symptomatic at 5 years due to metal induced degradation;
; Contraindications: Pre-existing sepsis. Young patient. Failure of internal fixation devices; Pre-existing disease of the acetabulum; Even without normal preoperative cartilagenous space, many patients will become symptomatic at 5 years due to metal induced degradation;")
75
Before and After

76
Complications Mortality - mortality after hemiarthroplasty is 10 to 40% Fracture of the Femur: 4.5% almost all fractures occur when surgeon attempts to reduce prosthesis; most are non displaced and involve either greater trochanter or neck; with femoral shaft fracture consider methy methacrylate combined with a long stem prosthesis; Post-op: sepsis: 2% to 20% more common w/ posterior surgical approach; infections may be superficial or deep Loosening and migration presence of a radiolucent zone around the prosthesis; if clinical signs and symptoms are present and loosening or migration is present, then consider revision to THR;erosion tends to occur in active pts with cemented Thompson hemiarthroplasty;

77
Complications Dislocation less than 10%.
more common with too much anteversion or retroversion, posterior capuslectomy, & excessive postoperative flexion or rotation with hip adducted

78
Outcome Mobility: 41% of elderly walk as well as pre-injury (Koval, Clin Orthop 1995). Mortality: 3% to 27% in first 3 months. 15-30% die within 1 year of fracture.

79
Treatment of extra-capsular hip fractures.
The goal of operative treatment is Strong ,stable fixation of the fracture fragments.

80
Treatment of extra-capsular hip fractures.
Dynamic Hip Screw: Shorter plate (e.g 2-hole) can be used for some undisplaced intra- capsular #s. Varying angles to suit angle at femoral neck. Sliding compression screw device allows collapse into position of stability.
 can be used for some undisplaced intra- capsular #s. Varying angles to suit angle at femoral neck. Sliding compression screw device allows collapse into position of stability.")
81
Treatment of extra-capsular hip fractures.
Dynamic Condylar Screw (95 °): Used in (paticularly) sub-troch #s. In certain inter-trochanteric #s.
: Used in (paticularly) sub-troch #s. In certain inter-trochanteric #s.")
82
Complications Early. Late.
1. Femoral Shaft Fracture (intra-operative). 2. Respiratory, urinary tract infections. 3. Wound haematoma/infection. 3. DVT/Pulmonary embolus. Late. 1. Avascular necrosis. 2. Delayed/Non-Union. 3. Fixation Failure. 4. Post-traumatic arthritis. 5. Deep Infection
. 2. Respiratory, urinary tract infections. 3. Wound haematoma/infection. 3. DVT/Pulmonary embolus. Late. 1. Avascular necrosis. 2. Delayed/Non-Union. 3. Fixation Failure. 4. Post-traumatic arthritis. 5. Deep Infection.")
83
Complications Other Complications: Pressure sores. Nerve palsies.
Prosthesis Dislocation. Failure to mobilise & death.

84
Outcome Mobility: 41% of elderly walk as well as pre-injury
(Koval, Clin Orthop 1995). Mortality: 3% to 27% in first 3 months. 15-20% die within 1 year of fracture. Mortality risk over age-matched controls for up to 1 year post injury. Inter-trochanteric #s associated with greater morbidity & mortality.
. Mortality: 3% to 27% in first 3 months % die within 1 year of fracture. Mortality risk over age-matched controls for up to 1 year post injury. Inter-trochanteric #s associated with greater morbidity & mortality.")
86
Important Exam Topics - Clinical Examination
Hip :Thomas test for fixed flexion deformity

87
Important Exam Topics - Clinical Examination
Hip :Trendelenburg test

88
Osteoarthritis May be Primary due to intrnsic defect (mechanical,immune, vascular, cartilage) Secondary - trauma, infection, congenital disorders. Get loss of the bearing surface, followed by development of osteophytes and breakdown of the osteochondral junction

89
Radiographic Features
Subchondral cysts ( from microfractures) Osteophyte formation Joint space narrowing Sclerotic bone formation
 Osteophyte formation. Joint space narrowing. Sclerotic bone formation.")
90
Degenerative Changes in the Hip
Subchondral cysts Joint space narrowing Sclerosis

91
Indications for Surgery- Joint Replacement
Pain is the main + best indication Degenerative joint disease – OA 1o or 2o Rheumatoid Arthritis Intractable pain Stiffness Deteriorating function

Similar presentations























>")


 guidelines with attention.>")
