Download presentation
Presentation is loading. Please wait.

1
CONCUSSION RECOGNITION AND MANAGEMENT Toggenburg Ski Patrol R Eugene Bailey, MD January 22, 2012

2
OBJECTIVES Head Injury – review of treatment What is a concussion? Extent of the problem Recognition and triage Define concussion management team Education / Promotion Our Return to play protocol at ESM Discuss protocol for Toggenburg

3
Feb 2, 2011 – Lindsey Vonn – concussion during practice.

4
15-4 Head Injuries

5
Suspect a Head or Spinal Injury With any unresponsive trauma patient When wounds or other injuries suggest large forces involved Observe patient carefully during the initial assessment

6
Injuries to the Head May be open or closed Bleeding may be profuse Closed injuries may involve swelling/ depression at site of skull fracture Bleeding inside skull may occur with any head injury

7
General Signs and Symptoms Lump or deformity in head, neck, or back Changing levels of responsiveness Drowsiness Confusion Dizziness Unequal pupils

8
General Signs and Symptoms continued Headache Clear fluid from nose or ears Stiff neck Inability to move any body part Tingling, numbness, or lack of feeling in feet or hands

9
Assessing an Unresponsive Patient If no life-threatening condition perform limited physical examination for other injuries Do not move patient unless necessary Check for serious injuries Stabilize head and neck

10
Assessing an Unresponsive Patient Ask those at scene: What happened Patient’s mental status before becoming unresponsive

11
Assessing a Responsive Patient If nature of injuries suggests potential spinal injury, carefully assess for spinal injury during physical examination Ask patient not to move more than you ask during the examination

12
Assessing a Responsive Patient Ask: Does your neck or back hurt? What happened? Where does it hurt?

13
Physical Examination Perform standard examination When checking torso, look for impaired breathing or loss of bladder/bowel control Compare strength from one side of body to other Assess both feet and both hands at same time

14
Physical Examination Perform standard examination Don’t assume patient without symptoms has no spinal injury. Consider forces involved When in doubt, keep head immobile while waiting for additional EMS

15
15-15 Skill: Head and Spinal Injury Assessment

16
Check the victim’s head.

17
Check neck for deformity, swelling, and pain.

18
Check sensation in feet.

19
Ask victim to point toes.

20
Ask victim to push against your hands with feet.

21
Check sensation in hands.

22
Ask victim to make a fist and curl it in.

23
Ask victim to squeeze your hands.

24
15-24 Brain Injuries

25
Occur with blow to head with/without open wound Brain injury likely with skull fracture Brain swelling/bleeding

26
Signs and Symptoms of a Brain Injury Severe or persistent headache Altered mental status (confusion, unresponsiveness) Lack of coordination, movement problems
 Lack of coordination, movement problems")
27
Signs and Symptoms of a Brain Injury Continued Weakness, numbness, loss of sensation, paralysis Nausea and vomiting Seizures Unequal pupils Problems with vision or speech Breathing problems or irregularities

28
Concussion Brain injury involving temporary impairment Usually no head wound or signs and symptoms of more serious head injury Victim may have been “knocked out” but regained consciousness quickly

29
Signs and Symptoms of Concussion Temporary confusion Memory loss about event Brief loss of responsiveness Mild or moderate altered mental status Unusual behavior Headache

30
Medical Evaluation Concussion patient may recover quickly Difficult to determine injury severity More serious signs and symptoms may occur over time Patients with suspected brain injuries require medical evaluation

31
Emergency Care for Head Injuries Perform standard patient care Use the jaw-thrust to open airway Follow local protocol re: oxygen Manually stabilize the head and neck Don’t let patient move

32
Emergency Care for Head Injuries continued Closely monitor mental status Control bleeding. No direct pressure on skull fracture Monitor vital signs Expect vomiting Provide additional care for skull fracture

33
Skull Fracture Check for possible skull fracture before applying direct pressure to scalp bleeding Direct pressure could push bone fragments into brain Skull fracture is life threatening

34
Signs of a Skull Fracture Deformed area Depressed or spongy area Blood or fluid from ears or nose Eyelids swollen shut or becoming discolored (bruising)
")
35
Bruising under eyes (raccoon eyes) Bruising behind ears (Battle’s sign) Unequal pupils An object impaled in skull Signs of a Skull Fracture
 Bruising behind ears (Battle’s sign) Unequal pupils An object impaled in skull Signs of a Skull Fracture")
36
Emergency Care for Skull Fractures Care as for any head/spinal injury Don’t clean wound, press on it, or remove impaled object Cover wound with sterile dressing

37
Emergency Care for Skull Fractures If bleeding, apply pressure only around edges of wound. Use a ring dressing Do not move victim unnecessarily

38
CONCUSSION MANAGEMENT

39
What is a Concussion? A concussion is a mild traumatic brain injury (MTBI) that interferes with normal function of the brain Evolving knowledge “dings” and “bell ringers” are serious brain injuries Do not have to have loss of conciousness Young athletes are at increased risk for serious problems
 that interferes with normal function of the brain Evolving knowledge dings and bell ringers are serious brain injuries Do not have to have loss of conciousness Young athletes are at increased risk for serious problems.")
40
The Problems in the Medical Field There is much variation in the knowledge of health care providers managing concussed athletes Physicians (MD/DO) Physician assistants Nurse practitioners Chiropractors Athletic trainers School nurses New and emerging research and technologies will lead to a continuing evolution of care
 Physician assistants Nurse practitioners Chiropractors Athletic trainers School nurses New and emerging research and technologies will lead to a continuing evolution of care")
41
Problems for Athletes- Post-Concussion Syndrome 85-90% of concussed young athletes will recover within 1 to 2 weeks The remainder may have symptoms lasting from weeks to months interfering with school and daily life Subtle deficits may persist a lifetime

42
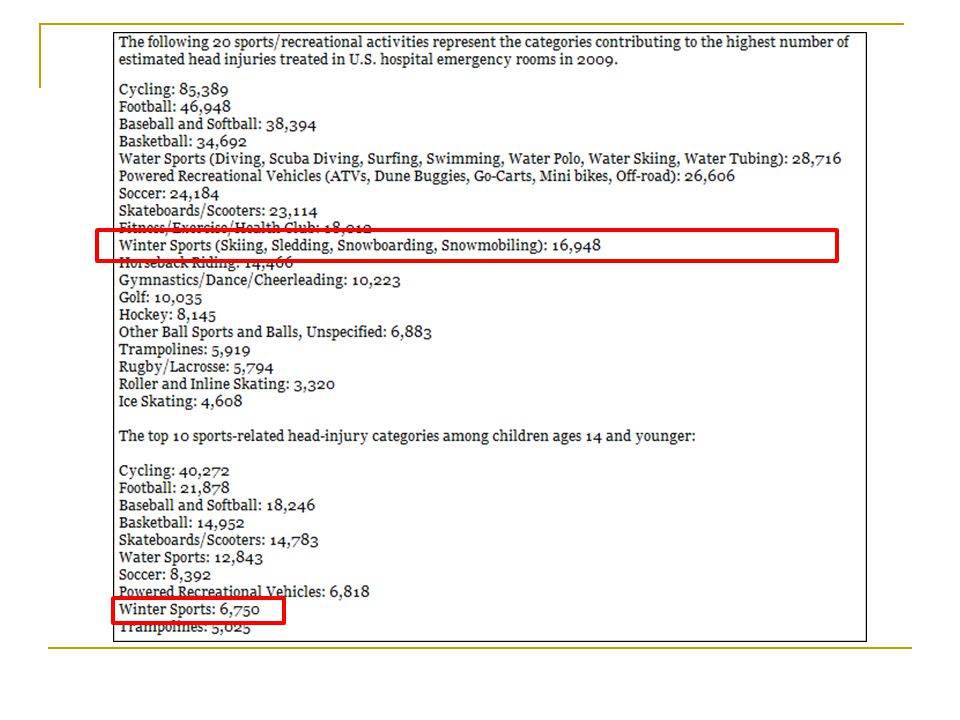
Extent of the Problem Professional athletes get a great deal of attention 1600 NFL players Much more common in high school than any other level- due to large number of participants HS Sports Participants Football- 1.14 million Boys Soccer- 384,000 Girls Soccer- 345,000 Boys Hoops- 545,000 Girls Hoops- 444,000 NFHS 2008-09

43
Extent of the Problem 19.3% of all FB injuries in 2009!!! Likely at least 100,000 concussions in HS athletes yearly based on CDC estimates

44
Not Just a Football Problem Injury rate per 100,000 player games in high school athletes Football47 Girls soccer36 Boys soccer22 Girls basketball21 Wrestling18 Boys basketball7 Softball7 Data from HS RIO JAT, 2007

46
What has happened to make this such a big deal? Increasing awareness and incidence Number of high profile athletes over the past 20 years Steve Young, Troy Aikman, Eric Lindros, etc Bigger and faster kids, increased opportunities

47
What has happened to make this such a big deal? High profile cases Second Impact Syndrome Death or devastating brain damage when having a second injury when not healed from the first Long-term effects Possible long-term effects- dementia, depression

48
NFL and long-term complications

49
Prevention “Concussion prevention” has become the “holy grail” for sports equipment marketers Soccer head gear Girl’s Lacrosse head gear/helmets Pole vaulting helmet New football helmets, soccer head pads, mouth guards- NO PROVEN PROTECTION FROM CONCUSSION!! Multiple flaws in a study looking at “Riddell Revolution” helmet Neurosurgery, 2006

50
Prevention

52
Concussion Diagnosis & Management 3 rd statement following the 1 st (Vienna - 2001) and 2 nd (Prague -2004) International Symposia
 and 2 nd (Prague -2004) International Symposia")
53
2010 – 2011 NFHS Rule Book Changes on Concussion Any athlete who exhibits signs, symptoms, or behaviors consistent with a concussion (such as loss of consciousness, headache, dizziness, confusion, or balance problems) shall be immediately removed from the contest and shall not return to play until cleared by an appropriate health care professional. (Please see NFHS Suggested Guidelines for Management of Concussion). Approved by NFHS Sports Medicine Advisory Committee – October 2009 Approved by the NFHS Board of Directors – October 2009
. Approved by NFHS Sports Medicine Advisory Committee – October 2009 Approved by the NFHS Board of Directors – October")
54
Staying Ahead of the Issue Need to take initiative Several meetings to review our policy and procedure Major campaign for awareness Revised recognition and management RTP protocol Establishment of the concussion management team

55
CONCUSSION MANAGEMENT TEAM 1. IDENTIFY THE PROBLEM 2. DEFINE OUR CONCUSSION MANAGEMENT TEAM 3. DEVELOP PROTOCOLS 4. INVOLVE COMMUNITY 5. EDUCATE ATHLETES, COACHES Ski Patrollers, PARENTS,PHYSICIANS

56
Family: Parents/guardians, siblings, grandparents Medical: Primary care doctor, neurologist, concussion specialist. School Physical: School Physician, Athletic Trainers, School Nurse, Coaches. School Academic: Teacher, Counselors, Administrator Toggenburg: Ski Patrol / Admin

57
Community based Multi disciplinary Concussion Management Team Family Team Medical Team Toggenburg Ski Patrol

58
Concussion Management- The Basics Coach Education Awareness and Recognition When in doubt, sit ‘em out!! Policies No return to activity on the same day of a concussion No return to activity if having symptoms of a concussion

59
What are we doing at ESM? Educating athletes, coaches and parents Field-side concussion evaluation form Follow up ESM Concussion Evaluation form for Physicians Return to play protocol

62
HEAD INJURY ASSESSMENT HEADACHE NAUSEA VOMITING BALANCE/ STABILITY ISSUES DIZZINESS FATIGUE TROUBLE FALLING ASLEEP SLEEPING MORE THAN USUAL SLEEPING LESS THAN USUAL DROWSINESS SENSITIVITY TO LIGHT SENSITIVITY TO NOISE IRRITABILITY SADNESS EMOTIONAL SENSITIVITY NUMBNESS/ TINGLING SENSATION IN EXTREMITIES FEELING “SLOW” FEELING “FOGGY” DIFFICULTY WITH CONCENTRATION DIFFICULTY WITH MEMORY BLURRED VISION DOUBLE VISION

63
Who? Parents Coaches Students Administrators Nurses Teachers Guidance Councilors Ski Patrollers

64
How will this information be promoted? Parent Meetings Posters Handouts Training classes for coaches In service presentations Access to online power point, and references What can Toggenburg do?

65
STEP BY STEP SCENARIO Athlete sustains head injury Evaluated on-field by AT, coach, or opposing team’s AT(if available) 1. Remove from play 2. Use Head Injury evaluation instrument 3. Minimum 20 minutes out of action, check athlete every 5 minutes 4. Athlete MAY NOT RETURN TO PLAY while ANY symptoms are present Decision- is a concussion suspected? Physician Referral, Parents contacted Athlete or parents given concussion information, including ESM concussion evaluation form Athlete seen by physician, in ER or by family physician Once athlete is symptom free and cleared by physician, Return To Play protocol begins under the supervision of an Athletic Trainer

66
STEP BY STEP SCENARIO Athlete sustains head injury Evaluated on-field by AT, coach, or opposing team’s AT(if available) 1. Remove from play 2. Use Head Injury evaluation instrument 3. Minimum 20 minutes out of action, check athlete every 5 minutes 4. Athlete MAY NOT RETURN TO PLAY while ANY symptoms are present Decision- is a concussion suspected? Physician Referral, Parents contacted Athlete or parents given concussion information, including ESM concussion evaluation form Athlete seen by physician, in ER or by family physician Once athlete is symptom free and cleared by physician, Return To Play protocol begins under the supervision of an Athletic Trainer

68
Step 1: Rest / No Physical Activity Step 2: Light aerobic activity (Walking, swimming, stationary bike 10-15 min) Step 3: Sport specific exercise (running drills, 20-30 min, no weight lifting) Step 4: Non-contact training drills (More progressive training drills, may start progressive resistance training) Step 5: Full contact practice (Participate in normal practice/training activities) Step 6: Return to play
 Step 3: Sport specific exercise (running drills, min, no weight lifting) Step 4: Non-contact training drills (More progressive training drills, may start progressive resistance training) Step 5: Full contact practice (Participate in normal practice/training activities) Step 6: Return to play")
69
If a step is failed, the athlete will drop back to the previous step and try again after 24hrs of rest. If the athlete continues to have symptoms after failing any 2 steps the athlete should be referred back to his/her physician.

70
Conclusions Educate Everyone dealing with young athletes must be aware of the signs, symptoms, and ramifications of concussions Mandate or Legislate? Concussion management policies must be in place at every level If you don’t do it, someone will do it for you

71
What can Toggenburg do? Discussion

72
Heat Index Procedures Use the following link from NYSPHSAA for heat index procedures: http://www.nysphsaa.org/safety/pdf/HeatI ndexProcedure.pdf Go to accuweather.com put in the area code for the location of your game If the Real Feel (heat index) temperature is above 96 the contest will be suspended.
 temperature is above 96 the contest will be suspended.")
73
Lightning Policy Hear it, see it, flee it. Find shelter for your team (school, bus, etc.) 30 minute wait period after the last sound or sight of lightning. The clock resets if seen or heard. Use the following link from NYSPHSAA for Thunder/Lightning procedures: http://www.nysphsaa.org/safety/pdf/ThunderLight ningPolicy.pdf http://www.nysphsaa.org/safety/pdf/ThunderLight ningPolicy.pdf
 30 minute wait period after the last sound or sight of lightning. The clock resets if seen or heard. Use the following link from NYSPHSAA for Thunder/Lightning procedures: ningPolicy.pdf ningPolicy.pdf.")
74
References http://www.nysphaa.org http://www.nfhs.org http://accuweather.com http://cdc.gov/concussion/ http://extras.mnginteractive.com/live/media/site36/2010/1102/2010110 2_071347_RMHC%20REAP%20Final%207-10.pdf (Rocky Mountain Youth Sports Medicine Institute) P.McCrory, W.Meewise, K. Johnston, J. Dvorak, M. Aubry, M. Molloy, &R. Cantu. (2009). Consensus statement on concussion in sport – The 3 rd International Conference on concussion in sport, held in Zurich, November 2008. Journal of Clinical Neuroscience. 16. 755-763.
. Consensus statement on concussion in sport – The 3 rd International Conference on concussion in sport, held in Zurich, November Journal of Clinical Neuroscience")
75
THANK YOUs!!!!!! Dr. Desiato and our Board of Education Bill McEachron – Athletic Director Dan Rancier, MD – ESM School Physician Eugene Bailey, MD- ESM School Physician Mark Powell, MS, ATC, CSCS Paul Houck, MS, ATC Paul Manfredo, BS, ATC And all parents in attendance tonight!

76
Feel free to contact us or go to the ESM Athletics website with any questions

Similar presentations










 with an ambulance crew responding at the.>")











