Download presentation
1
2010 Food Safety Epidemiology Capacity Assessment CSTE Annual Conference June 13, 2011 Lauren Rosenberg, MPA Council of State and Territorial Epidemiologists

2
Purpose To enumerate and characterize the foodborne epidemiology workforce To characterize the use of electronic tools used in outbreak detection and investigation To identify barriers to conducting effective outbreak investigations

3
Key Areas of Assessment Capacity to detect, investigate, and respond Enumeration of foodborne disease epidemiology capacity Legal authority in states CIFOR (Council to Improve Foodborne Outbreak Response) Guidelines for Foodborne Disease Outbreak Response
 Guidelines for Foodborne Disease Outbreak Response")
4
Methods Assessment in the field during April 2010 – Distributed electronically 100% overall response rate from states Scale of capacity: – None – None of the activity, knowledge, or resources described within the question are met. – Minimal – 1-24% are met. – Partial – 25-49% are met. – Substantial – 50-74% are met. – Almost full – 75-99% are met. – Full – 100% are met.

5
Capacity to detect, investigate, and respond

6
Capacity to Use Electronic Lab Reporting

7
States’ Use of Electronic Database to Maintain Records for Enteric Disease Cases (N=49)
")
8
Information recorded by electronic database for enteric disease cases (N=50)
")
9
Proportion of Foodborne Disease Outbreaks for which Specimens were Collected Stool specimen collection is more common than food sample collection – 38 of 50 states collect stool specimens for 50% or more of outbreaks – 13 of 50 states collect food samples for 50% or more of outbreaks

10
States that Investigate 75-100% of Foodborne Outbreaks by Pathogen Type

11
Moderate-to-substantial reported barriers to investigation of enteric outbreaks Delayed notification (82%) Lack of adequate number of staff (58%) Low priority (54%) Lack of ability to pay overtime (40%)
 Lack of adequate number of staff (58%) Low priority (54%) Lack of ability to pay overtime (40%)")
12
Factors not perceived as barriers to investigation of enteric outbreaks Lack of epidemiology expertise (24%) Lack of statistical support (16%) Travel policy constraints (16%) Lack of lab capacity (14%)
 Lack of statistical support (16%) Travel policy constraints (16%) Lack of lab capacity (14%)")
13
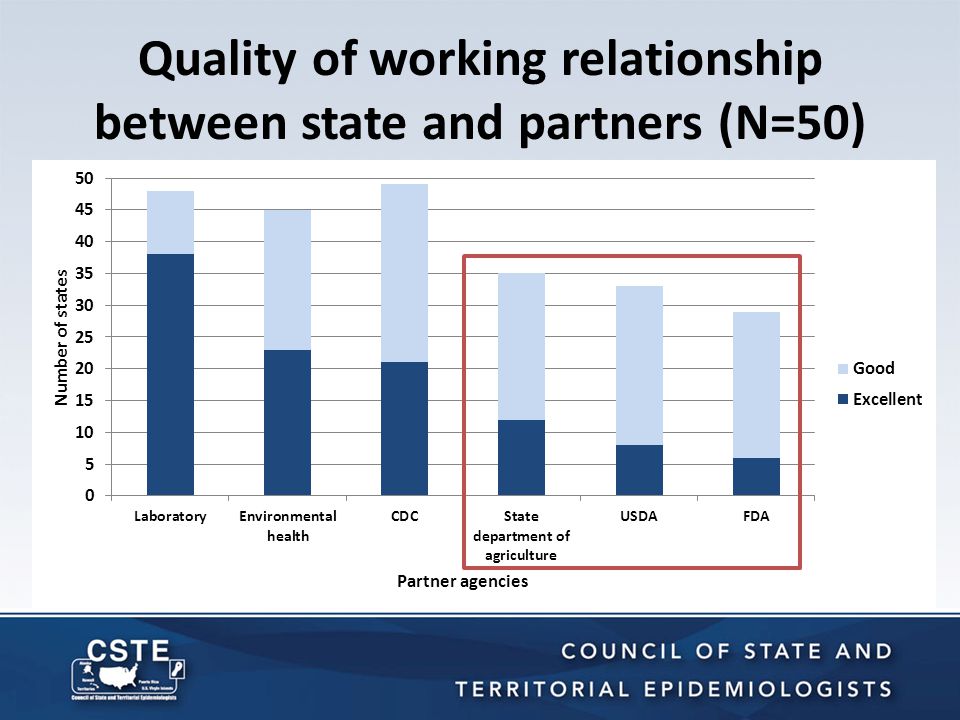
Quality of working relationship between state and partners (N=50)
")
15
Enumerating foodborne epidemiology capacity

16
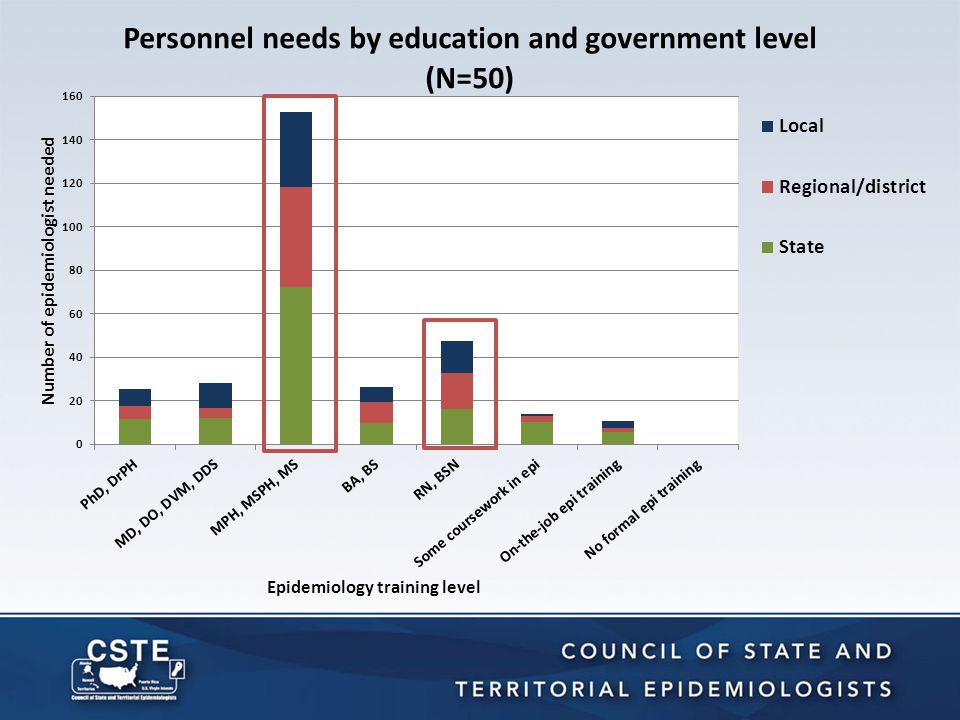
Training of foodborne disease epidemiologists in state health departments Level of epidemiology trainingNo.% Doctoral degree in epidemiology 145.7 Professional background (e.g., MD, DO, DVM, DDS) with dual degree in epidemiology 25.510.4 Masters degree in epidemiology 93.538.6 Bachelors degree in epidemiology 15.56.3 Nursing designation or degree 2912.2 Completed some coursework in epidemiology 2510.6 Received on-the-job training in epidemiology 23.510.0 No formal training in epidemiology 146.1 Total240100 54.7%
 with dual degree in epidemiology Masters degree in epidemiology Bachelors degree in epidemiology Nursing designation or degree Completed some coursework in epidemiology Received on-the-job training in epidemiology No formal training in epidemiology Total %")
19
Legal authority

20
Sources of Legal Authority to Conduct Foodborne Investigations (N=49) Answer Options# States% States State statutes that grant general authority for public health activities 4285.7% State agency regulations that grant general authority for public health activities 3163.3% State agency regulations that expressly authorize foodborne investigations 2551.0% State statutes that expressly authorize foodborne investigations 2142.9% Local government ordinances/regulations 1836.7% Other (please specify) 24.1%
 Answer Options# States% States State statutes that grant general authority for public health activities % State agency regulations that grant general authority for public health activities % State agency regulations that expressly authorize foodborne investigations % State statutes that expressly authorize foodborne investigations % Local government ordinances/regulations % Other (please specify) 24.1%")
21
Legal barriers to outbreak response A minority of states reported any substantial barriers Barriers reported include: – Constraints to conduct a coordinated response (36%) – Constraints on accessing information (31%) – Constraints on sharing information (28%)
 – Constraints on accessing information (31%) – Constraints on sharing information (28%)")
22
Release of information about enteric disease Individuals – Information released only for a legitimate purpose (84% of states) – Information is confidential; not open to public release (100% of states) Business entities – Information released for a legitimate purpose (40% of states) – More open to public release upon request (29% of states)
 – Information is confidential; not open to public release (100% of states) Business entities – Information released for a legitimate purpose (40% of states) – More open to public release upon request (29% of states)")
23
Conclusions There is significant variation among states with regard to reporting and surveillance. Most states report a lack of capacity, impacting their ability to investigate and intervene in the control of foodborne illness. – ⅔ of states investigate all E. coli O157 outbreaks. – ½ collected stool specimens – ¼ collected implicated food specimens

24
Conclusions Delayed notification and lack of adequate number of staff are the most common barriers to completion of foodborne illness investigations. There are differences in states’ working relationships with other disciplines, including federal partners.

25
Conclusions States consistently reported full legal authority to detect, investigate, and respond to foodborne diseases.

26
Recommendations Increase staff working in foodborne disease epidemiology and surveillance in state and local health departments Enhance epidemiology training opportunities for staff to promote a well-qualified workforce

27
Recommendations Increase investment in IT to realize greater improvements in capacity for the detection, reporting, investigation, and surveillance of outbreaks Develop strategies for further enhancing the relationship between state/local health departments and federal regulatory agencies

28
Recommendations Develop marketing strategies to increase awareness and use of the CIFOR Guidelines Toolkit

29
Acknowledgements Matthew Boulton, CSTE Consultant CSTE Workgroup: Roberta Hammond (FDA) Tim Jones (Tennessee) C.P. Kanwat (South Carolina) Bill Keene (Oregon) Bela Matyas (California) Julie Schlegel (South Carolina) Don Sharp (CDC)
 Bill Keene (Oregon) Bela Matyas (California) Julie Schlegel (South Carolina) Don Sharp (CDC).")
30
Thank you!
















 Ottawa, Canada, 20-21 September 2006 Overview: United.>")
 Sustainability for Early Childhood Systems Building.>")




