Download presentation
Presentation is loading. Please wait.

1
Sedation in the ICU from A to E
The ABCDE Bundle

2
Salvatore Vitale M.D. Director Cardio-vascular Anesthesia Westchester Medical Center Assistant Professor Dept. of Anesthesiology New York Medical College Immediate Past President New York State Society of Anesthesiologists

3
Westchester Medical Center
TAVR Team

4
Learning Objectives Describe current guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit Use validated scales to measure sedation, pain, agitation, and delirium in critically ill patients Compare the benefits and limitations of available sedatives and analgesics in the acute care, procedural, and surgical settings

5
Goals for Sedation and Analgesia
Prevent pain and anxiety Decrease oxygen consumption Decrease the stress response Patient-ventilator synchrony Avoid adverse neurocognitive sequelae Depression PTSD Dementia Anxiety Rotondi AJ, et al. Crit Care Med. 2002;30: Weinert C. Curr Opin in Crit Care. 2005;11: Kress JP, et al. Am J Respir Crit Care Med. 1996;153:

6
Jacobi J, et al. Crit Care Med. 2002;30:119-141
American College of Critical Care Medicine (ACCM) Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult Guideline focus Prolonged sedation and analgesia Patients older than 12 years Patients during mechanical ventilation Assessment and treatment recommendations Analgesia Sedation Delirium Sleep Jacobi J, et al. Crit Care Med. 2002;30:
 Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Guideline focus. Prolonged sedation and analgesia. Patients older than 12 years. Patients during mechanical ventilation. Assessment and treatment recommendations. Analgesia. Sedation. Delirium. Sleep. Jacobi J, et al. Crit Care Med. 2002;30:")
7
What Is the ABCDE Bundle?
ABCDE bundle is designed to: Standardize care processes Break the cycle of oversedation and prolonged ventilation Pull and add pratik’s here. Vasilevskis EE, et al. Chest. 2010;138(5):
:")
8
What Is in the ABCDE Bundle?
Awakening and Breathing Trial coordination Coordination/Choice of Sedation Delirium Monitoring and Management Early Mobility Vasilevskis EE, et al. Chest. 2010;138(5):
:")
9
ABCDE Awakening Breathing Coordination/Choice of Sedation Delirium Monitoring and Management Early Mobilization

10
Daily Sedation Interruption (DSI) Decreases Duration of Mechanical Ventilation
Hold sedation infusion until patient awake and then restart at 50% of the prior dose “Awake” defined as any 3 of the following: Open eyes in response to voice Use eyes to follow investigator on request Squeeze hand on request Stick out tongue on request Fewer diagnostic tests to assess changes in mental status No increase in rate of agitated-related complications or episodes of patient-initiated device removal No increase in PTSD or cardiac ischemia Kress JP, et al. N Engl J Med. 2000;342:

11
The ABC Trial: Objectives
To determine the efficacy and safety of a protocol linking: spontaneous awakening trials (SATs) & spontaneous breathing trials (SBTs) Ventilator-free days Duration of mechanical ventilation ICU and hospital length of stay Duration of coma and delirium Long-term neuropsychological outcomes Girard TD, et al. Lancet. 2008;371:
 & spontaneous breathing trials (SBTs) Ventilator-free days. Duration of mechanical ventilation. ICU and hospital length of stay. Duration of coma and delirium. Long-term neuropsychological outcomes. Girard TD, et al. Lancet. 2008;371:")
12
ABC Trial: Main Outcomes
SBT SAT+SBT P-value Ventilator-free days 12 15 0.02 Time-to-Event, days Successful extubation, days 7.0 5 0.05 ICU discharge, days 13 9 0.02 Hospital discharge, days 19 15 0.04 Death at 1 year, n (%) 97 (58%) 74 (44%) 0.01 Days of brain dysfunction Coma 3.0 2.0 0.002 Delirium 2.0 2.0 0.50 *Median, except as noted Girard TD, et al. Lancet. 2008;371:
 97 (58%) 74 (44%) Days of brain dysfunction. Coma Delirium *Median, except as noted. Girard TD, et al. Lancet. 2008;371:")
13
ABC Trial: 1 Year Mortality
Girard TD, et al. Lancet. 2008;371:

14
Canada – 40% get SATs (273 physicians in 2005)1
Daily Sedation Interruption (DSI) Not Standard of Practice at Most Institutions Canada – 40% get SATs (273 physicians in 2005)1 US – 40% get SATs ( )2 Germany – 34% get SATs (214 ICUs in 2006)3 France – 40–50% deeply sedated with 90% on continuous infusion of sedative/opiate4 1. Mehta S, et al. Crit Care Med. 2006;34: 2. Devlin J. Crit Care Med. 2006;34: 3. Martin J, et al. Crit Care. 2007;11:R124. 4. Payen JF, et al. Anesthesiology. 2007;106:
 Not Standard of Practice at Most Institutions. Canada – 40% get SATs (273 physicians in 2005)1. US – 40% get SATs ( )2. Germany – 34% get SATs (214 ICUs in 2006)3. France – 40–50% deeply sedated with 90% on continuous infusion of sedative/opiate4. 1. Mehta S, et al. Crit Care Med. 2006;34: Devlin J. Crit Care Med. 2006;34: Martin J, et al. Crit Care. 2007;11:R Payen JF, et al. Anesthesiology. 2007;106:")
15
Barriers to Daily Sedation Interruption (Survey of 904 SCCM members)
Increased device removal Poor nursing acceptance Compromises patient comfort Leads to respiratory compromise Difficult to coordinate with nurse No benefit Leads to cardiac ischemia Leads to PTSD #1 Barrier #2 Barrier #3 Barrier 10 20 30 40 50 60 70 Number of respondents (%) Clinicians preferring propofol were more likely use daily interruption than those preferring benzodiazepines (55% vs 40%, P < ) Tanios MA, et al. J Crit Care. 2009;24:66-73. 15
 Clinicians preferring propofol were more likely use daily interruption. than those preferring benzodiazepines (55% vs 40%, P < ) Tanios MA, et al. J Crit Care. 2009;24:")
16
Awakening and Breathing (AB) Safety Screens
Breathing Trial Awakening Trial No active agitation Oxygen saturation ≥ 88% FiO2 ≤ 50% PEEP ≤ 8 cm H2O No myocardial ischemia (24h) Normal intracranial pressure No significant vasopressor or inotrope use No active seizures No active alcohol withdrawal No active agitation No active paralytic use No myocardial ischemia (24h) Normal intracranial pressure Girard TD, et al. Lancet. 2008;371(9607):
 Normal intracranial pressure. No significant vasopressor or inotrope use. No active seizures. No active alcohol withdrawal. No active agitation. No active paralytic use. No myocardial ischemia (24h) Normal intracranial pressure. Girard TD, et al. Lancet. 2008;371(9607):")
17
ABCDE Awakening Breathing Coordination/Choice of Sedation Delirium Monitoring and Management Early Mobilization

18
ICU Sedation: The Balancing Act
Patient Comfort and Ventilatory Optimization Oversedation Prolonged mechanical ventilation Increased length of stay Increased risk of complications - Ventilator-associated pneumonia Increased diagnostic testing Inability to evaluate for delirium G O A L Undersedation Patient recall Device removal Ineffectual mechanical ventilation Initiation of neuromuscular blockade Myocardial or cerebral ischemia Decreased family satisfaction w/care Jacobi J, et al. Crit Care Med. 2002;30: 18 18

19
Targeted Sedation 30.6% 15.4% 54.0% Undersedated3 Oversedated
Continuous sedation carries the risks associated with oversedation and may increase the duration of mechanical ventilation (MV)1 MV patients accrue significantly more cost during their ICU stay than non-MV patients2 $31,574 versus $12,931, P < 0.001 Sedation should be titrated to achieve a cooperative patient and daily wake-up, a JC requirement1,2 30.6% 15.4% 54.0% Undersedated3 Oversedated On Target 1. Kress JP, et al. N Engl J Med. 2000;342: 2. Dasta JF, et al. Crit Care Med. 2005;33: 3. Kaplan LJ, Bailey H. Crit Care. 2000;4(suppl 1):P190.
1. MV patients accrue significantly more cost during their ICU stay than non-MV patients2. $31,574 versus $12,931, P < Sedation should be titrated to achieve a cooperative patient and daily wake-up, a JC requirement1, % 15.4% 54.0% Undersedated3. Oversedated. On Target. 1. Kress JP, et al. N Engl J Med. 2000;342: Dasta JF, et al. Crit Care Med. 2005;33: Kaplan LJ, Bailey H. Crit Care. 2000;4(suppl 1):P190.")
20
Assessing Agitation and Sedation
Richmond Agitation-Sedation Scale (RASS) Sessler CN, et al. Am J Respir Crit Care Med ;166(10): Ely EW, et al. JAMA. 2003;289: Sedation-Agitation Scale (SAS) Riker RR, et al. Crit Care Med. 1999;27: Brandl K, et al. Pharmacotherapy. 2001;21: 20
 Sessler CN, et al. Am J Respir Crit Care Med. 2002;166(10): Ely EW, et al. JAMA. 2003;289: Sedation-Agitation Scale (SAS) Riker RR, et al. Crit Care Med. 1999;27: Brandl K, et al. Pharmacotherapy. 2001;21:")
21
Richmond Agitation Sedation Scale (RASS) *
Score Term Description +4 Combative Overtly combative, violent, immediate danger to staff +3 Very agitated Pulls or removes tube(s) or catheter(s); aggressive +2 Agitated Frequent non-purposeful movement, fights ventilator +1 Restless Anxious but movements not aggressive vigorous Alert and calm -1 Drowsy Not fully alert, but has sustained awakening (eye-opening/eye contact) to voice (>10 seconds) -2 Light sedation Briefly awakens with eye contact to voice (<10 seconds) -3 Moderate sedation Movement or eye opening to voice (but no eye contact) -4 Deep sedation No response to voice, but movement or eye opening to physical stimulation -5 Unarousable No response to voice or physical stimulation
 or catheter(s); aggressive. +2. Agitated. Frequent non-purposeful movement, fights ventilator. +1. Restless. Anxious but movements not aggressive vigorous. Alert and calm. -1. Drowsy. Not fully alert, but has sustained awakening (eye-opening/eye contact) to voice (>10 seconds) -2. Light sedation. Briefly awakens with eye contact to voice (<10 seconds) -3. Moderate sedation. Movement or eye opening to voice (but no eye contact) -4. Deep sedation. No response to voice, but movement or eye opening to physical stimulation. -5. Unarousable. No response to voice or physical stimulation.")
22
Procedure for RASS Assessment
1. Observe patient Patient is alert, restless, or agitated. (score 0 to +4) 2. If not alert, state patient’s name and say to open eyes and look at speaker. Patient awakens with sustained eye opening and eye contact. (score –1) Patient awakens with eye opening and eye contact, but not sustained. (score –2) Patient has any movement in response to voice but no eye contact. (score –3) 3. When no response to verbal stimulation, physically stimulate patient by shaking shoulder and/or rubbing sternum. Patient has any movement to physical stimulation. (score –4) Patient has no response to any stimulation. (score –5)
 2. If not alert, state patient’s name and say to open eyes and look at speaker. Patient awakens with sustained eye opening and eye contact. (score –1) Patient awakens with eye opening and eye contact, but not sustained. (score –2) Patient has any movement in response to voice but no eye contact. (score –3) 3. When no response to verbal stimulation, physically stimulate patient by shaking shoulder and/or rubbing sternum. Patient has any movement to physical stimulation. (score –4) Patient has no response to any stimulation. (score –5)")
23
Characteristics of an Ideal Sedative
Rapid onset of action allows rapid recovery after discontinuation Effective at providing adequate sedation with predictable dose response Easy to administer Lack of drug accumulation Few adverse effects Minimal adverse interactions with other drugs Cost-effective Promotes natural sleep Ostermann ME, et al. JAMA. 2000;283: Jacobi J, et al. Crit Care Med. 2002;30: Dasta JF, et al. Pharmacother. 2006;26: Nelson LE, et al. Anesthesiol. 2003;98:

24
Patient Comorbidities to Consider
Chronic pain Organ dysfunction CV instability Substance withdrawal Respiratory insufficiency Obesity Obstructive sleep apnea

25
Overview of Presently available Intravenous Agents

26
The Good a2 Agonist Propofol Acetaminophen NSAIDs Haldol

27
The Bad Opiates Benzodiazepines

28
The Ugly Flumazenil Naloxone

29
The Good

30
Dexmedetomidine a2 Agonist
Clinical Effects Adverse Effects Antihypertensive Sedation Analgesia Decreased shivering Anxiolysis Patient arousability Potentiate effects of opioids, sedatives, and anesthetics Decrease sympathetic activity Hypotension Hypertension Nausea Bradycardia Dry mouth Peripheral vasoconstriction at high doses Kamibayashi T, et al. Anesthesiol. 2000;93: Bhana N, et al. Drugs. 2000;59(2):
:")
31
Clinical Effects Adverse Effects
Propofol Clinical Effects Adverse Effects Sedation Hypnosis Anxiolysis Muscle relaxation Mild bronchodilation Decreased ICP Decreased cerebral metabolic rate Antiemetic Pain on injection Respiratory depression Hypotension Decreased myocardial contractility Increased serum triglycerides Tolerance Propofol infusion syndrome Prolonged effect with high adiposity Seizures (rare) Ellett ML. Gastroenterol Nurs. 2010;33(4): Lundström S, et al. J Pain Symptom Manage. 2010;40(3):
 Ellett ML. Gastroenterol Nurs. 2010;33(4): Lundström S, et al. J Pain Symptom Manage. 2010;40(3):")
32
Clinical Effects Adverse Effects
Acetaminophen Clinical Effects Adverse Effects Available in po and IV forms Demonstrated effective relief of pain, either alone (mild to moderate pain) or as part of a multimodal regimen (moderate to severe pain) No delerium Peak effect: within an hour of administration Duration of effect: 4 to 6 hours No significant effect on platelet aggregation5 Potential Hepatotoxicity Antipyretic effects may mask fever in patients treated for post-surgical pain
 or as part of a multimodal regimen (moderate to severe pain) No delerium. Peak effect: within an hour of administration. Duration of effect: 4 to 6 hours. No significant effect on platelet aggregation5. Potential Hepatotoxicity. Antipyretic effects may mask fever in patients treated for post-surgical pain.")
33
NSAIDS Ketorolac and Ibuprofen
Lacks respiratory depression Good pain control Anti platelet activity Black box warning for cardiac patients

34
Haloperidol Dopamine Antagonist
Clinical Effects Adverse Effects Dysphoria2 Adverse CV effects include QT interval prolongation Extrapyramidal symptoms, neuroleptic malignant syndrome (rare)1 Metabolism altered by drug-drug interactions2 Hypnotic agent with antipsychotic properties1 For treatment of delirium in critically ill adults1 Does not cause respiratory depression1 1. Harvey MA. Am J Crit Care. 1996;5:7-16. 2. Crippen DW. Crit Care Clin. 1990;6:
1. Metabolism altered by drug-drug interactions2. Hypnotic agent with antipsychotic properties1. For treatment of delirium in critically ill adults1. Does not cause respiratory depression1. 1. Harvey MA. Am J Crit Care. 1996;5: Crippen DW. Crit Care Clin. 1990;6:")
35
The Bad

36
Opioids Clinical Effects Adverse Effects Analgesia Hypotension
Bradycardia Respiratory depression Tolerance Constipation Withdrawal symptoms Hormonal changes Sedation Fentanyl Morphine Remifentanyl Benyamin R, et al. Pain Physician. 2008;11(2 Suppl):S
:S")
37
Benzodiazepines Clinical Effects Adverse Effects
Sedation, anxiolysis, and amnesia Commonly used for long-term sedation Adverse Effects Metabolic acidosis (propylene glycol vehicle toxicity) Retrograde and anterograde amnesia Delirium Midazolam Lorazapam Olkkola KT, Ahonen J. Handb Exp Pharmacol. 2008;(182): Wilson KC, et al. Chest. 2005;128(3):
 Retrograde and anterograde amnesia. Delirium. Midazolam. Lorazapam. Olkkola KT, Ahonen J. Handb Exp Pharmacol. 2008;(182): Wilson KC, et al. Chest. 2005;128(3):")
38
Comparison of Clinical Effects
Benzodiazepines Propofol Opioids a2 Agonists Haloperidol Sedation X X X X X Alleviate anxiety1,2 X X Analgesic properties1-4 X X Promote arousability during sedation2-4 X Facilitate ventilation during weaning2-4 X X Control delirium1-4 X X 1. Blanchard AR. Postgrad Med. 2002;111:59-74. 2. Kamibayashi T, et al. Anesthesiol. 2000;95: 3. Maze M, et al. Anesthetic Pharmacology: Physiologic Principles and Clinical Practice. Churchill Livingstone; 2004. 4. Maze M, et al. Crit Care Clin. 2001;17:

39
Comparison of Adverse Effects
Benzodiazepines Propofol Opioids a2 Agonists Haloperidol Prolonged weaning 1 X X X * Respiratory depression 1 X X X Hypotension 1-3 X X X X X Constipation 1 X Deliriogenic X X X Tachycardia 1 Bradycardia 1 X X X X *Excluding remifentanil 1. Harvey MA. Am J Crit Care. 1996;5:7-18. 2. Aantaa R, et al. Drugs of the Future. 1993;18:49-56. 3. Maze M, et al. Crit Care Clin. 2001;17:

40
The Ugly

41
Flumazenil Flumazenil reverses the effects of sedatives from the benzodiazepine group of drugs.

42
Naloxone An opioid antagonist drug developed in the 1960s.
Naloxone is a drug used to counter the effects of opiate overdose, for example heroin or morphine overdose. Use with caution in the opioid addicted patient It is not to be confused with naltrexone, an opioid receptor antagonist with qualitatively different effects, used for dependence treatment rather than emergency overdose treatment.

43
ABCDE Awakening Breathing Coordination/Choice of Sedation Delirium Monitoring and Management Early Mobilization

44
Cardinal Symptoms of Delirium and Coma
Morandi A, et al. Intensive Care Med. 2008;34:

45
ICU Delirium Develops in ~2/3 of critically ill patients
Hypoactive or mixed forms most common Increased risk Benzodiazepines Extended ventilation Immobility Associated with weakness Undiagnosed in up to 72% of cases Vasilevskis EE, et al. Chest. 2010;138(5):
:")
46
DELIRIUM Less Modifiable More Modifiable Patient Factors
Increased age Alcohol use Male gender Living alone Smoking Renal disease Predisposing Disease Cardiac disease Cognitive impairment (eg, dementia) Pulmonary disease Less Modifiable Acute Illness Length of stay Fever Medicine service Lack of nutrition Hypotension Sepsis Metabolic disorders Tubes/catheters Medications: Anticholinergics Corticosteroids - Benzodiazepines DELIRIUM Environment Admission via ED or through transfer Isolation No clock No daylight No visitors Noise Physical restraints More Modifiable Van Rompaey B, et al. Crit Care. 2009;13:R77. Inouye SK, et al. JAMA.1996;275: Skrobik Y. Crit Care Clin. 2009;25:
 Pulmonary disease. Less Modifiable. Acute Illness. Length of stay. Fever. Medicine service. Lack of nutrition. Hypotension. Sepsis. Metabolic disorders. Tubes/catheters. Medications: Anticholinergics. Corticosteroids. - Benzodiazepines. DELIRIUM. Environment. Admission via ED or through transfer. Isolation. No clock. No daylight. No visitors. Noise. Physical restraints. More. Modifiable. Van Rompaey B, et al. Crit Care. 2009;13:R77. Inouye SK, et al. JAMA.1996;275: Skrobik Y. Crit Care Clin. 2009;25:")
47
Mechanisms for Delirium in the Critically Ill: Numerous and
Not Clearly Understood Neurotransmitter imbalance Neuroinflammation Blood brain barrier permeability Impaired oxidative metabolism Microglial activation Abnormal levels of large neutral amino acids (eg, tryptophan) and their metabolism (eg, kynurenine pathway) It’s a bit complicated Maldonado JR. Crit Care Clin. 2008;24(4): Pandharipande PP. Intensive Care Med. 2009;35(11): Adams-Wilson JR, et al. Crit Care Med (in press)
 and their metabolism (eg, kynurenine pathway) It’s a bit complicated. Maldonado JR. Crit Care Clin. 2008;24(4): Pandharipande PP. Intensive Care Med. 2009;35(11): Adams-Wilson JR, et al. Crit Care Med (in press)")
48
During the ICU/Hospital Stay After Hospital Discharge
Sequelae of Delirium Increased mortality Longer intubation time Average 10 additional days in hospital Higher costs of care During the ICU/Hospital Stay Increased mortality Development of dementia Long-term cognitive impairment Requirement for care in chronic care facility Decreased functional status at 6 months After Hospital Discharge Bruno JJ, Warren ML. Crit Care Nurs Clin North Am. 2010;22(2): Shehabi Y, et al. Crit Care Med. 2010;38(12): Rockwood K, et al. Age Ageing. 1999;28(6): Jackson JC, et al. Neuropsychol Rev. 2004;14:87-98. Nelson JE, et al. Arch Intern Med. 2006;166: 48
: Shehabi Y, et al. Crit Care Med. 2010;38(12): Rockwood K, et al. Age Ageing. 1999;28(6): Jackson JC, et al. Neuropsychol Rev. 2004;14: Nelson JE, et al. Arch Intern Med. 2006;166:")
49
Delirium Duration and Mortality
Kaplan-Meier Survival Curve P < 0.001 Each day of delirium in the ICU increases the hazard of mortality by 10% Pisani MA. Am J Respir Crit Care Med. 2009;180:

50
Worse Long-term Cognitive Performance
Duration of delirium was an independent predictor of cognitive impairment An increase from 1 day of delirium to 5 days was associated with nearly a 5-point decline in cognitive battery scores Girard TD, et al. Crit Care Med. 2010;38: Misak CJ. Am J Respir Crit Care Med. 2004;170(4):
:")
51
Risk Factors Specific for ICU Delirium
Benzodiazepine use4,10 Coma (medical vs. pharmacologic)4,9 Morphine use (?data unclear) Dementia1,2,3 Hypertension history4,5 Alcoholism3,4 Severity of illness1,4,6,7,8 Age (?pos6,8 /neg2,3,4,9) Pisani MA, et al. Crit Care Med. 2009;37: Pisani MA, et al. Arch Intern Med. 2007;167: Van Rompaey B, et al. Crit Care. 2009;13:R77. Ouimet S, et al. Intensive Care Med. 2007;33:66-73. Dubois MJ, et al. Intensive Care Med. 2001;27: Pandharipande PP, et al. Anesthesiology. 2006;104:21-26. Pisani MA, et al. Crit Care Med. 2009;37: Pandharipande PP, et al. Intensive Care Med. 2009;35: Ely EW, et al. Crit Care Med. 2007;35: Pandharipande PP, et al. J Trauma. 2008;65: Coma is an independent risk factor for ICU patients to develop delirium, based upon moderate quality of evidence (B). However, establishing a definitive relationship between various subtypes of coma (i.e. medication-related, structural, neurological, medical) and delirium in ICU patients will require further study.
4,9. Morphine use ( data unclear) Dementia1,2,3. Hypertension history4,5. Alcoholism3,4. Severity of illness1,4,6,7,8. Age ( pos6,8 /neg2,3,4,9) Pisani MA, et al. Crit Care Med. 2009;37: Pisani MA, et al. Arch Intern Med. 2007;167: Van Rompaey B, et al. Crit Care. 2009;13:R77. Ouimet S, et al. Intensive Care Med. 2007;33: Dubois MJ, et al. Intensive Care Med. 2001;27: Pandharipande PP, et al. Anesthesiology. 2006;104: Pisani MA, et al. Crit Care Med. 2009;37: Pandharipande PP, et al. Intensive Care Med. 2009;35: Ely EW, et al. Crit Care Med. 2007;35: Pandharipande PP, et al. J Trauma. 2008;65: Coma is an independent risk factor for ICU patients to develop delirium, based upon moderate quality of evidence (B). However, establishing a definitive relationship between various subtypes of coma (i.e. medication-related, structural, neurological, medical) and delirium in ICU patients will require further study.")
52
Delirium Assessment Tools
Confusion Assessment Method for the ICU (CAM-ICU) Ely EW, et al. Crit Care Med. 2001;29: Ely EW, et al. JAMA. 2001;286: Intensive Care Delirium Screening Checklist (ICDSC) Bergeron N, et al. Intensive Care Med ;27: Ouimet S, et al. Intensive Care Med ;33:
 Ely EW, et al. Crit Care Med. 2001;29: Ely EW, et al. JAMA. 2001;286: Intensive Care Delirium Screening Checklist (ICDSC) Bergeron N, et al. Intensive Care Med. 2001;27: Ouimet S, et al. Intensive Care Med. 2007;33:")
54
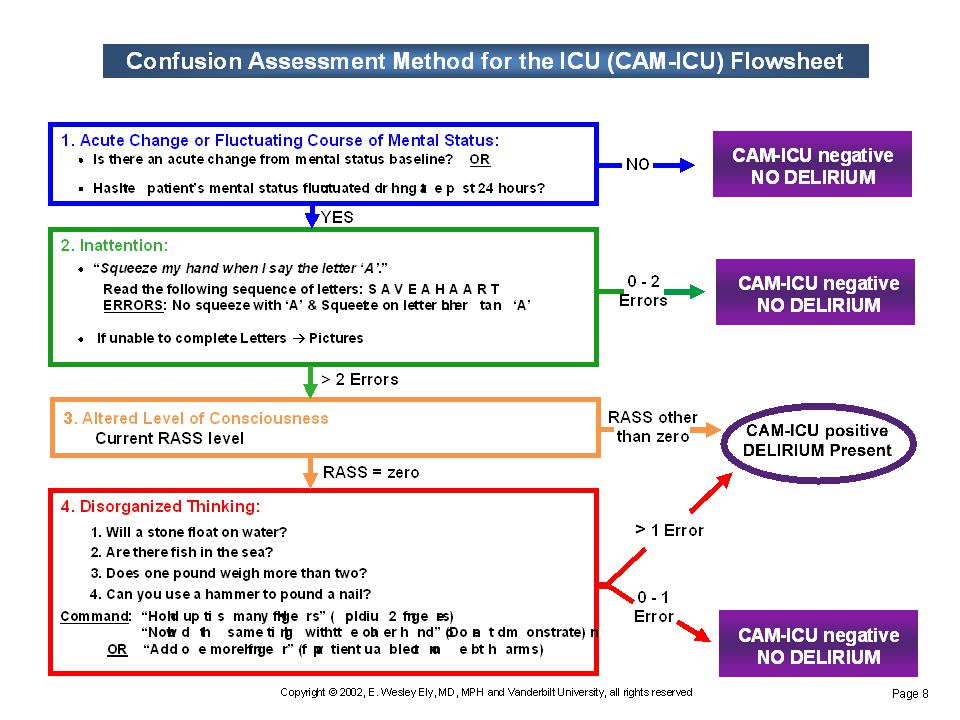
Confusion Assessment Method (CAM-ICU)
1. Acute onset of mental status changes or a fluctuating course and 2. Inattention and 3. Altered level of consciousness 4. Disorganized thinking or = Delirium Ely EW, et al. Crit Care Med. 2001;29: Ely EW, et al. JAMA. 2001;286:

56
Delirium Assessment Tools
Confusion Assessment Method for the ICU (CAM-ICU) Ely EW, et al. Crit Care Med. 2001;29: Ely EW, et al. JAMA. 2001;286: Intensive Care Delirium Screening Checklist (ICDSC) Bergeron N, et al. Intensive Care Med ;27: Ouimet S, et al. Intensive Care Med ;33:
 Ely EW, et al. Crit Care Med. 2001;29: Ely EW, et al. JAMA. 2001;286: Intensive Care Delirium Screening Checklist (ICDSC) Bergeron N, et al. Intensive Care Med. 2001;27: Ouimet S, et al. Intensive Care Med. 2007;33:")
57
Intensive Care Delirium Screening Checklist
1. Altered level of consciousness 2. Inattention 3. Disorientation 4. Hallucinations 5. Psychomotor agitation or retardation 6. Inappropriate speech 7. Sleep/wake cycle disturbances 8. Symptom fluctuation Score 1 point for each component present during shift Score of 1-3 = Subsyndromal Delirium Score of ≥ 4 = Delirium Bergeron N, et al. Intensive Care Med. 2001;27: Ouimet S, et al. Intensive Care Med. 2007;33:

58
Helpful Approach to Delirium Management
Stop THINK Lastly, medicate

59
Stop and THINK Do any meds need to be stopped or lowered?
Especially consider sedatives Is patient on minimal amount necessary? Daily sedation cessation Targeted sedation plan Do sedatives need to be changed? Toxic Situations CHF, shock, dehydration Deliriogenic meds (tight titration) New organ failure (liver/kidney) Hypoxemia Infection/sepsis (nosocomial) Immobilization Nonpharm interventions Hearing aids, glasses, reorient, sleep protocols, music, noise control, ambulation K+ or electrolyte problems
 New organ failure (liver/kidney) Hypoxemia. Infection/sepsis (nosocomial) Immobilization. Nonpharm interventions. Hearing aids, glasses, reorient, sleep protocols, music, noise control, ambulation. K+ or electrolyte problems.")
60
Delirium Nonpharmacologic Interventions
Early mobility – the only nonpharmacologic intervention shown to reduce ICU delirium1 Other interventions: Environmental changes (eg, noise reduction) Sensory aids (eg, hearing aids, glasses) Reorientation and stimulation Sleep preservation and enhancement Schweickert WD, et al. Lancet. 2009;373:
 Sensory aids (eg, hearing aids, glasses) Reorientation and stimulation. Sleep preservation and enhancement. Schweickert WD, et al. Lancet. 2009;373:")
61
Sleep Abnormalities in the ICU
More time in light sleep Less time in deep sleep More sleep fragmentation There is little evidence that sedatives in the ICU restore normal sleep Friese R. Crit Care Med. 2008;36: Weinhouse GL, Watson PL. Crit Care Clin. 2009;25:

62
Boosting Sleep Quality in ICU
Optimize environmental strategies Day/night variation, reduce night interruptions, noise reduction Avoid benzodiazepines (↓ Slow wave sleep (SWS) & REM) Consider dexmedetomidine (↑ SWS) GABA receptor agonists (eg, zolpidem) Sedating antidepressants (eg, trazodone) or antipsychotics Melatonin Pilot: may improve sleep quality of ICU COPD patients GABA receptor agonists that don’t reduce slow wave sleep (like zolpidem) Weinhouse GL, Watson PL. Crit Care Clinics. 2009;25: Faulhaber J, et al. Psychopharmacology. 1997;130: Shilo L, et al. Chronobiol Int. 2000;17:71-76. 62
 & REM) Consider dexmedetomidine (↑ SWS) GABA receptor agonists (eg, zolpidem) Sedating antidepressants (eg, trazodone) or antipsychotics. Melatonin. Pilot: may improve sleep quality of ICU COPD patients. GABA receptor agonists that don’t reduce slow wave sleep (like zolpidem) Weinhouse GL, Watson PL. Crit Care Clinics. 2009;25: Faulhaber J, et al. Psychopharmacology. 1997;130: Shilo L, et al. Chronobiol Int. 2000;17:")
63
Effect of Common Sedatives and Analgesics on Sleep
There is little evidence that administration of sedatives in the ICU achieves the restorative function of normal sleep Benzodiazepines ↑ Stage 2 NREM ↓ Slow wave sleep (SWS) and REM Propofol ↑ Total sleep time without enhancing REM ↓ SWS Analgesics Abnormal sleep architecture Dexmedetomidine ↑ SWS Weinhouse GL, et al. Sleep. 2006;29: Nelson LE, et al. Anesthesiology. 2003;98:
 and REM. Propofol. ↑ Total sleep time without enhancing REM. ↓ SWS. Analgesics. Abnormal sleep architecture. Dexmedetomidine. ↑ SWS. Weinhouse GL, et al. Sleep. 2006;29: Nelson LE, et al. Anesthesiology. 2003;98:")
64
Standardized Intervention
Elder Life Program Targeted Risk Factor Standardized Intervention Cognitive impairment Orientation & therapeutic activity protocol (discuss current events, word games, reorient, etc) Sleep deprivation Sleep enhancement & nonpharm sleep protocol (noise reduction, back massages, schedule adjustment) Immobility Early mobilization protocol (active ROM, reduce restraint use, ambulation, remove catheters) Visual impairment Vision protocol (glasses, adaptive equipment, reinforce use) Hearing impairment Hearing protocol (amplification devices, hearing aids, earwax disimpaction) Dehydration Dehydration protocol (early recognition of dehydration & volume repletion) “Targeted risk factors were selected on the basis of evidence of their association with the risk of delirium and because they were amenable to intervention strategies considered feasible in the context of current hospital practice.” Intervention provided by a trained interdisciplinary team: geriatric nurse specialist, ELP specialists, recreational therapist, PT consultant, geriatrician, trained volunteers. Inouye SK, et al. N Engl J Med. 1999;340:
 Sleep deprivation. Sleep enhancement & nonpharm sleep protocol. (noise reduction, back massages, schedule adjustment) Immobility. Early mobilization protocol. (active ROM, reduce restraint use, ambulation, remove catheters) Visual impairment. Vision protocol. (glasses, adaptive equipment, reinforce use) Hearing impairment. Hearing protocol. (amplification devices, hearing aids, earwax disimpaction) Dehydration. Dehydration protocol. (early recognition of dehydration & volume repletion) Targeted risk factors were selected on the basis of evidence of their association with the risk of delirium and because they were amenable to intervention strategies considered feasible in the context of current hospital practice. Intervention provided by a trained interdisciplinary team: geriatric nurse specialist, ELP specialists, recreational therapist, PT consultant, geriatrician, trained volunteers. Inouye SK, et al. N Engl J Med. 1999;340:")
65
Results Outcome Intervention Control P-value
Incidence of delirium, N (%) 42 (9.9) 64 (15) 0.02 Total days of delirium 105 161 Episodes of delirium 62 90 0.03 ↓ delirium incidence in patients with intermediate baseline risk Improved orientation score with targeted intervention (P = 0.04) Reduced rate of sedative use for sleep (P = 0.001) 87% overall adherence to protocol High baseline risk also had reduced incidence, but not statistically significant Inouye SK, et al. N Engl J Med. 1999;340:
 42 (9.9) 64 (15) Total days of delirium Episodes of delirium ↓ delirium incidence in patients with intermediate baseline risk. Improved orientation score with targeted intervention (P = 0.04) Reduced rate of sedative use for sleep (P = 0.001) 87% overall adherence to protocol. High baseline risk also had reduced incidence, but not statistically significant. Inouye SK, et al. N Engl J Med. 1999;340:")
66
Haloperidol Dopamine Antagonist
Clinical Effects Adverse Effects Dysphoria2 Hypnotic agent with antipsychotic properties1 Adverse CV effects include QT interval prolongation For treatment of delirium in critically ill adults1 Extrapyramidal symptoms, Neuroleptic malignant syndrome (rare)1 Does not cause respiratory depression1 Metabolism altered by drug-drug interactions2 1. Harvey MA. Am J Crit Care. 1996;5:7-16. 2. Crippen DW. Crit Care Clin. 1990;6:
1. Does not cause respiratory depression1. Metabolism altered by drug-drug interactions2. 1. Harvey MA. Am J Crit Care. 1996;5: Crippen DW. Crit Care Clin. 1990;6:")
67
Association Between Intravenous Haloperidol & Prolonged QT Interval
However, ventricular tachyarrhythmia was not detected among 307 patients within a 1 year period, although the ECG was continuously monitored for at least 8 hours after intravenous HAL. The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous. However, in an emergency situation, clinicians cannot exclude patients predisposed to torsade de pointes, such as those with inherited ion channel disorders. Therefore, clinicians should be aware of the association between intravenous HAL and QT prolongation

68
Atypical Antipsychotics
Receptor adherence is variable between agents Use has increased substantially Possible safety benefits Decreased extrapyramidal effects Little effect on the QTc interval (except ziprasidone) Less hypotension/fewer orthostatic effects Less likely to cause neuroleptic malignant syndrome Possible limitations No IV formulations available Little published experience in ICU patients Troublesome reports of adverse events but most associated with prolonged use in non-delirium patients Devlin JW, et al. Harv Rev Psychiatry. 2011;19:59-67. 68
 Less hypotension/fewer orthostatic effects. Less likely to cause neuroleptic malignant syndrome. Possible limitations. No IV formulations available. Little published experience in ICU patients. Troublesome reports of adverse events but most associated with prolonged use in non-delirium patients. Devlin JW, et al. Harv Rev Psychiatry. 2011;19:")
69
List of Atypical Antipsychotics
Amisulpride (Solian) Paliperidone (Invega) Aripiprazole (Abilify) Perospirone (Lullan) Asenapine (Saphris) Quetiapine (Seroquel) Blonanserin (Lonasen) Remoxipride (Roxiam) Carpipramine (Prazinil) Risperidone (Risperdal) Clocapramine (Clofekton) Sertindole (Serdolect) Sulpiride (Sulpirid, Eglonyl) Clotiapine (Entumine) Clozapine (Clozaril) Ziprasidone (Geodon, Zeldox) Iloperidone (Fanapt) Lurasidone (Latuda) Zotepine (Nipolept) Mosapramine (Cremin) Olanzapine (Zyprexa)
 Paliperidone (Invega) Aripiprazole (Abilify) Perospirone (Lullan) Asenapine (Saphris) Quetiapine (Seroquel) Blonanserin (Lonasen) Remoxipride (Roxiam) Carpipramine (Prazinil) Risperidone (Risperdal) Clocapramine (Clofekton) Sertindole (Serdolect) Sulpiride (Sulpirid, Eglonyl) Clotiapine (Entumine) Clozapine (Clozaril) Ziprasidone (Geodon, Zeldox) Iloperidone (Fanapt) Lurasidone (Latuda) Zotepine (Nipolept) Mosapramine (Cremin) Olanzapine (Zyprexa)")
70
Use of Atypical Antipsychotic Therapy Is Increasing
90 80 70 60 2001 50 2007 Respondents, % 40 30 20 10 Propofol Haloperidol Atypical Antipsychotics Benzodiazepines Ely EW, et al. Crit Care Med. 2004;32: Patel RP, et al. Crit Care Med. 2009;37:

71
Prophylactic Haloperidol
RCT of short-term low-dose IV haloperidol Patients N = 457 Age > 65 years ICU after noncardiac surgery Intervention Haloperidol 0.5 mg IV bolus then Infusion 0.1 mg/h for 12 hrs Placebo Primary endpoint Incidence of delirium within the first 7 days after surgery Crit Care Med Mar;40(3):731-9. Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: A randomized controlled trial*. Wang W, Li HL, Wang DX, Zhu X, Li SL, Yao GQ, Chen KS, Gu XE, Zhu SN. Source From the Departments of Anesthesiology and Surgical Intensive Care (WW, DXW, SLL, KSC, XEG) and Biostatistics (SNZ), Peking University First Hospital, Beijing, China; Department of Critical Care Medicine (HLL, XZ, GQY), Peking University Third Hospital, Beijing, China. Abstract OBJECTIVES: : To evaluate the efficacy and safety of short-term low-dose intravenous haloperidol for delirium prevention in critically ill elderly patients after noncardiac surgery. DESIGN: : Prospective, randomized, double-blind, and placebo-controlled trial in two centers. SETTING: : Intensive care units of two large tertiary teaching hospitals. PATIENTS: : Four hundred fifty-seven patients 65 yrs or older who were admitted to the intensive care unit after noncardiac surgery. INTERVENTION: : Haloperidol (0.5 mg intravenous bolus injection followed by continuous infusion at a rate of 0.1 mg/h for 12 hrs; n = 229) or placebo (n = 228) was randomly administered from intensive care unit admission. MEASURES: : The primary end point was the incidence of delirium within the first 7 days after surgery. Secondary end points included time to onset of delirium, number of delirium-free days, length of intensive care unit stay, all-cause 28-day mortality, and adverse events. Delirium was assessed using the confusion assessment method for the intensive care unit. RESULTS: : The incidence of delirium during the first 7 days after surgery was 15.3% (35/229) in the haloperidol group and 23.2% (53/228) in the control group (p = .031). The mean time to onset of delirium and the mean number of delirium-free days were significantly longer (6.2 days [95% confidence interval ] vs. 5.7 days [95% confidence interval ]; p = .021; and 6.8 ± 0.5 days vs. 6.7 ± 0.8 days; p = .027, respectively), whereas the median length of intensive care unit stay was significantly shorter (21.3 hrs [95% confidence interval ] vs hrs [95% confidence interval ]; p = .024) in the haloperidol group than in the control group. There was no significant difference with regard to all-cause 28-day mortality between the two groups (0.9% [2/229] vs. 2.6% [6/228]; p = .175). No drug-related side effects were documented. CONCLUSIONS: : For elderly patients admitted to intensive care unit after noncardiac surgery, short-term prophylactic administration of low-dose intravenous haloperidol significantly decreased the incidence of postoperative delirium. The therapy was well-tolerated. Wang W, et al. Crit Care Med. 2012;40(3):
: Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: A randomized controlled trial*. Wang W, Li HL, Wang DX, Zhu X, Li SL, Yao GQ, Chen KS, Gu XE, Zhu SN. Source. From the Departments of Anesthesiology and Surgical Intensive Care (WW, DXW, SLL, KSC, XEG) and Biostatistics (SNZ), Peking University First Hospital, Beijing, China; Department of Critical Care Medicine (HLL, XZ, GQY), Peking University Third Hospital, Beijing, China. Abstract. OBJECTIVES: : To evaluate the efficacy and safety of short-term low-dose intravenous haloperidol for delirium prevention in critically ill elderly patients after noncardiac surgery. DESIGN: : Prospective, randomized, double-blind, and placebo-controlled trial in two centers. SETTING: : Intensive care units of two large tertiary teaching hospitals. PATIENTS: : Four hundred fifty-seven patients 65 yrs or older who were admitted to the intensive care unit after noncardiac surgery. INTERVENTION: : Haloperidol (0.5 mg intravenous bolus injection followed by continuous infusion at a rate of 0.1 mg/h for 12 hrs; n = 229) or placebo (n = 228) was randomly administered from intensive care unit admission. MEASURES: : The primary end point was the incidence of delirium within the first 7 days after surgery. Secondary end points included time to onset of delirium, number of delirium-free days, length of intensive care unit stay, all-cause 28-day mortality, and adverse events. Delirium was assessed using the confusion assessment method for the intensive care unit. RESULTS: : The incidence of delirium during the first 7 days after surgery was 15.3% (35/229) in the haloperidol group and 23.2% (53/228) in the control group (p = .031). The mean time to onset of delirium and the mean number of delirium-free days were significantly longer (6.2 days [95% confidence interval ] vs. 5.7 days [95% confidence interval ]; p = .021; and 6.8 ± 0.5 days vs. 6.7 ± 0.8 days; p = .027, respectively), whereas the median length of intensive care unit stay was significantly shorter (21.3 hrs [95% confidence interval ] vs hrs [95% confidence interval ]; p = .024) in the haloperidol group than in the control group. There was no significant difference with regard to all-cause 28-day mortality between the two groups (0.9% [2/229] vs. 2.6% [6/228]; p = .175). No drug-related side effects were documented. CONCLUSIONS: : For elderly patients admitted to intensive care unit after noncardiac surgery, short-term prophylactic administration of low-dose intravenous haloperidol significantly decreased the incidence of postoperative delirium. The therapy was well-tolerated. Wang W, et al. Crit Care Med. 2012;40(3):")
72
Prophylactic Haloperidol
Haloperidol (n = 229) Placebo (n = 229) P-value 7 day delirium incidence (%) 15.3 23.2 0.031 Mean time to delirium onset (days) 6.2 5.7 0.021 Mean time delirium-free (days) 6.8 6.7 0.027 Median ICU LOS (hours) 21.3 23.0 0.024 All-cause 28-day mortality (%) 0.9 2.6 0.175 Prophylactic Haloperidol Crit Care Med Mar;40(3):731-9. Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: A randomized controlled trial*. Wang W, Li HL, Wang DX, Zhu X, Li SL, Yao GQ, Chen KS, Gu XE, Zhu SN. Source From the Departments of Anesthesiology and Surgical Intensive Care (WW, DXW, SLL, KSC, XEG) and Biostatistics (SNZ), Peking University First Hospital, Beijing, China; Department of Critical Care Medicine (HLL, XZ, GQY), Peking University Third Hospital, Beijing, China. Abstract OBJECTIVES: : To evaluate the efficacy and safety of short-term low-dose intravenous haloperidol for delirium prevention in critically ill elderly patients after noncardiac surgery. DESIGN: : Prospective, randomized, double-blind, and placebo-controlled trial in two centers. SETTING: : Intensive care units of two large tertiary teaching hospitals. PATIENTS: : Four hundred fifty-seven patients 65 yrs or older who were admitted to the intensive care unit after noncardiac surgery. INTERVENTION: : Haloperidol (0.5 mg intravenous bolus injection followed by continuous infusion at a rate of 0.1 mg/h for 12 hrs; n = 229) or placebo (n = 228) was randomly administered from intensive care unit admission. MEASURES: : The primary end point was the incidence of delirium within the first 7 days after surgery. Secondary end points included time to onset of delirium, number of delirium-free days, length of intensive care unit stay, all-cause 28-day mortality, and adverse events. Delirium was assessed using the confusion assessment method for the intensive care unit. RESULTS: : The incidence of delirium during the first 7 days after surgery was 15.3% (35/229) in the haloperidol group and 23.2% (53/228) in the control group (p = .031). The mean time to onset of delirium and the mean number of delirium-free days were significantly longer (6.2 days [95% confidence interval ] vs. 5.7 days [95% confidence interval ]; p = .021; and 6.8 ± 0.5 days vs. 6.7 ± 0.8 days; p = .027, respectively), whereas the median length of intensive care unit stay was significantly shorter (21.3 hrs [95% confidence interval ] vs hrs [95% confidence interval ]; p = .024) in the haloperidol group than in the control group. There was no significant difference with regard to all-cause 28-day mortality between the two groups (0.9% [2/229] vs. 2.6% [6/228]; p = .175). No drug-related side effects were documented. CONCLUSIONS: : For elderly patients admitted to intensive care unit after noncardiac surgery, short-term prophylactic administration of low-dose intravenous haloperidol significantly decreased the incidence of postoperative delirium. The therapy was well-tolerated. Wang W, et al. Crit Care Med. 2012;40(3):
 Placebo. (n = 229) P-value. 7 day delirium incidence (%) Mean time to delirium onset (days) Mean time delirium-free (days) Median ICU LOS (hours) All-cause 28-day mortality (%) Prophylactic Haloperidol. Crit Care Med Mar;40(3): Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: A randomized controlled trial*. Wang W, Li HL, Wang DX, Zhu X, Li SL, Yao GQ, Chen KS, Gu XE, Zhu SN. Source. From the Departments of Anesthesiology and Surgical Intensive Care (WW, DXW, SLL, KSC, XEG) and Biostatistics (SNZ), Peking University First Hospital, Beijing, China; Department of Critical Care Medicine (HLL, XZ, GQY), Peking University Third Hospital, Beijing, China. Abstract. OBJECTIVES: : To evaluate the efficacy and safety of short-term low-dose intravenous haloperidol for delirium prevention in critically ill elderly patients after noncardiac surgery. DESIGN: : Prospective, randomized, double-blind, and placebo-controlled trial in two centers. SETTING: : Intensive care units of two large tertiary teaching hospitals. PATIENTS: : Four hundred fifty-seven patients 65 yrs or older who were admitted to the intensive care unit after noncardiac surgery. INTERVENTION: : Haloperidol (0.5 mg intravenous bolus injection followed by continuous infusion at a rate of 0.1 mg/h for 12 hrs; n = 229) or placebo (n = 228) was randomly administered from intensive care unit admission. MEASURES: : The primary end point was the incidence of delirium within the first 7 days after surgery. Secondary end points included time to onset of delirium, number of delirium-free days, length of intensive care unit stay, all-cause 28-day mortality, and adverse events. Delirium was assessed using the confusion assessment method for the intensive care unit. RESULTS: : The incidence of delirium during the first 7 days after surgery was 15.3% (35/229) in the haloperidol group and 23.2% (53/228) in the control group (p = .031). The mean time to onset of delirium and the mean number of delirium-free days were significantly longer (6.2 days [95% confidence interval ] vs. 5.7 days [95% confidence interval ]; p = .021; and 6.8 ± 0.5 days vs. 6.7 ± 0.8 days; p = .027, respectively), whereas the median length of intensive care unit stay was significantly shorter (21.3 hrs [95% confidence interval ] vs hrs [95% confidence interval ]; p = .024) in the haloperidol group than in the control group. There was no significant difference with regard to all-cause 28-day mortality between the two groups (0.9% [2/229] vs. 2.6% [6/228]; p = .175). No drug-related side effects were documented. CONCLUSIONS: : For elderly patients admitted to intensive care unit after noncardiac surgery, short-term prophylactic administration of low-dose intravenous haloperidol significantly decreased the incidence of postoperative delirium. The therapy was well-tolerated. Wang W, et al. Crit Care Med. 2012;40(3):")
73
Delirium + Haloperidol PRN
Quetiapine vs. Placebo Delirium + Haloperidol PRN Quetiapine (n = 18) Placebo (n = 18) Randomized, double-blind, placebo-controlled Multisite (3 centers) 36 ICU patients PO delivery of study drug Quetiapine dose: mg q12h Primary outcome: time to first resolution of delirium (ie, first 12-hour period when ICDSC ≤ 3) Titrated in response to Haldol dosing q50mg intervals every 12 hrs. IV prn Haldol 1-10,mg up to q2hrs no other antipsychotics or continuous infusions allowed. 10 day treatment Dosing info From article: The study drug was continued until one of the following occurred: (1) the subject was deemed by the attending intensivist, based on their clinical judgment, to no longer demonstrate signs of delirium and, therefore, to no longer require scheduled therapy with an antipsychotic agent; (2) 10 days of therapy had elapsed; (3) ICU discharge occurred; or (4) an adverse event potentially attributable to the study drug occurred that warranted discontinuation of the study drug. Allowing the attending intensivist to discontinue study drug once the subject no longer had signs of delirium was consistent with existing clinical practice in our institutions. In situations in which 10 days of therapy was reached or the subject was ready to transfer out of the ICU while still receiving study drug, the subject’s treatment assignment was revealed to the attending intensivist (but not the study team) to help determine the best course of therapy (which could include continued therapy with quetiapine). Limitations: patient safety (3, 41, 44, 48, 49). A number of potential limitations of our study must be considered when evaluating the results. Although adequate to demonstrate a difference in our primary outcome, our sample size was not large enough to reliably detect differences in any of the efficacy or safety outcomes. In addition, the multiple analyses that were completed may have contributed to an inflated type 1 error. Therefore, our investigation should be considered a pilot study. The rigorous study inclusion criteria that we chose lead to only 14% of To accommodate the varying duration of delirium seen in clinical practice, we did not require a minimum duration of study drug treatment, instead allowing the subject’s intensivist to discontinue study drug when delirium was thought to have resolved or the subject was ready to transfer from the ICU. Given its fluctuating nature, considering delirium resolved when first noted to be absent may be premature, but it is a reasonable and reproducible event. In addition, study drug may have been discontinued prematurely in subjects with hypoactive delirium, although the optimal way to treat these patients is not well-defined (3, 50–53). Whereas the same “as-needed” haloperidol dosing protocol was used for all study patients, the average dose of haloperidol that was administered was lower than the dose recommended in some guidelines and may reflect increasing safety concerns among clinicians regarding the use of high-dose haloperidol therapy (9, 54). The greater use of haloperidol in patients receiving placebo could have diminished the treatment effect of quetiapine that was observed. Devlin JW, et al. Crit Care Med. 2010;38(2):
 Placebo (n = 18) Randomized, double-blind, placebo-controlled. Multisite (3 centers) 36 ICU patients. PO delivery of study drug. Quetiapine dose: mg q12h. Primary outcome: time to first resolution of delirium (ie, first 12-hour period when ICDSC ≤ 3) Titrated in response to Haldol dosing q50mg intervals every 12 hrs. IV prn Haldol 1-10,mg up to q2hrs no other antipsychotics or continuous infusions allowed. 10 day treatment. Dosing info From article: The study drug was continued until one of. the following occurred: (1) the subject was. deemed by the attending intensivist, based on. their clinical judgment, to no longer demonstrate. signs of delirium and, therefore, to no. longer require scheduled therapy with an antipsychotic. agent; (2) 10 days of therapy had. elapsed; (3) ICU discharge occurred; or (4) an. adverse event potentially attributable to the. study drug occurred that warranted discontinuation. of the study drug. Allowing the attending. intensivist to discontinue study drug once. the subject no longer had signs of delirium. was consistent with existing clinical practice. in our institutions. In situations in which 10. days of therapy was reached or the subject was. ready to transfer out of the ICU while still. receiving study drug, the subject’s treatment. assignment was revealed to the attending intensivist. (but not the study team) to help determine. the best course of therapy (which could include. continued therapy with quetiapine). Limitations: patient safety (3, 41, 44, 48, 49). A number of potential limitations of. our study must be considered when evaluating. the results. Although adequate to. demonstrate a difference in our primary. outcome, our sample size was not large. enough to reliably detect differences in. any of the efficacy or safety outcomes. In. addition, the multiple analyses that were. completed may have contributed to an. inflated type 1 error. Therefore, our investigation. should be considered a pilot. study. The rigorous study inclusion criteria. that we chose lead to only 14% of. To accommodate the varying duration. of delirium seen in clinical practice, we. did not require a minimum duration of. study drug treatment, instead allowing. the subject’s intensivist to discontinue. study drug when delirium was thought to. have resolved or the subject was ready to. transfer from the ICU. Given its fluctuating. nature, considering delirium resolved. when first noted to be absent may be. premature, but it is a reasonable and reproducible. event. In addition, study drug. may have been discontinued prematurely. in subjects with hypoactive delirium, although. the optimal way to treat these. patients is not well-defined (3, 50–53). Whereas the same as-needed haloperidol. dosing protocol was used for all study. patients, the average dose of haloperidol. that was administered was lower than the. dose recommended in some guidelines. and may reflect increasing safety concerns. among clinicians regarding the use. of high-dose haloperidol therapy (9, 54). The greater use of haloperidol in patients. receiving placebo could have diminished. the treatment effect of quetiapine that. was observed. Devlin JW, et al. Crit Care Med. 2010;38(2):")
74
Patients with First Resolution of Delirium
Log-Rank P = 0.001 Placebo Proportion of Patients with Delirium Quetiapine Day During Study Drug Administration Quetiapine added to as-needed haloperidol results in faster delirium resolution, less agitation, and a greater rate of transfer to home or rehabilitation. Devlin JW, et al. Crit Care Med. 2010;38: 74

75
Impact of Quetiapine on the Resolution of Individual Delirium Symptoms
Median ICDSC and individual delirium symptoms similar at study baseline Quetiapine Placebo P value Median time to symptom resolution Log rank Inattention 3 hrs 8 hrs 0.10 Disorientation 2 hrs 10 hrs Symptom fluctuation 4 hrs 14 hrs 0.004 Agitation 5 hrs 1 hrs 0.04 Time with each symptom [median (IQR)] Comparison of Proportions 47 (0-67)% 78 (43-100)% 0.02 Hallucinations 0 (0-17)% 28 (0-43)% 47 (19-67)% 89 (33-100)% Devlin JW, et al. Crit Care. 2011;15(5):R215.
] Comparison of Proportions. 47 (0-67)% 78 (43-100)% Hallucinations. 0 (0-17)% 28 (0-43)% 47 (19-67)% 89 (33-100)% Devlin JW, et al. Crit Care. 2011;15(5):R215.")
76
Rivastigmine for Delirium?
FDA approved for dementia of Alzheimer’s or Parkinson’s Cholinesterase inhibitor Result Mortality (vs placebo): 22% vs 8%, P = 0.07 Delirium (vs placebo): 5 vs 3 days, P = 0.06 Conclusion: Need RCTs for delirium as endpoint Don’t use rivastigmine for ICU delirium Survival (%) Time (days after inclusion) Lancet Nov 27;376(9755): Epub 2010 Nov 4. Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. van Eijk MM, Roes KC, Honing ML, Kuiper MA, Karakus A, van der Jagt M, Spronk PE, van Gool WA, van der Mast RC, Kesecioglu J, Slooter AJ. Source Department of Intensive Care Medicine, University Medical Centre, Utrecht, Netherlands. Abstract BACKGROUND: Delirium is frequently diagnosed in critically ill patients and is associated with adverse outcome. Impaired cholinergic neurotransmission seems to have an important role in the development of delirium. We aimed to establish the effect of the cholinesterase inhibitor rivastigmine on the duration of delirium in critically ill patients. METHODS: Patients (aged ≥18 years) who were diagnosed with delirium were enrolled from six intensive care units in the Netherlands, and treated between November, 2008, and January, Patients were randomised (1:1 ratio) to receive an increasing dose of rivastigmine or placebo, starting at 0·75 mL (1·5 mg rivastigmine) twice daily and increasing in increments to 3 mL (6 mg rivastigmine) twice daily from day 10 onwards, as an adjunct to usual care based on haloperidol. The trial pharmacist generated the randomisation sequence by computer, and consecutively numbered bottles of the study drug according to this sequence to conceal allocation. The primary outcome was the duration of delirium during hospital admission. Analysis was by intention to treat. Duration of delirium was censored for patients who died or were discharged from hospital while delirious. Patients, medical staff, and investigators were masked to treatment allocation. Members of the data safety and monitoring board (DSMB) were unmasked and did interim analyses every 3 months. This trial is registered with ClinicalTrials.gov, number NCT FINDINGS: Although a sample size of 440 patients was planned, after inclusion of 104 patients with delirium who were eligible for the intention-to-treat analysis (n=54 on rivastigmine, n=50 on placebo), the DSMB recommended that the trial be halted because mortality in the rivastigmine group (n=12, 22%) was higher than in the placebo group (n=4, 8%; p=0·07). Median duration of delirium was longer in the rivastigmine group (5·0 days, IQR 2·7-14·2) than in the placebo group (3·0 days, IQR 1·0-9·3; p=0·06). INTERPRETATION: Rivastigmine did not decrease duration of delirium and might have increased mortality so we do not recommend use of rivastigmine to treat delirium in critically ill patients. Accessed March 2012. Van Eijk MM, et al. Lancet ;376(9755):
: 22% vs 8%, P = Delirium (vs placebo): 5 vs 3 days, P = Conclusion: Need RCTs for delirium as endpoint. Don’t use rivastigmine for ICU delirium. Survival (%) Time (days after inclusion) Lancet Nov 27;376(9755): Epub 2010 Nov 4. Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. van Eijk MM, Roes KC, Honing ML, Kuiper MA, Karakus A, van der Jagt M, Spronk PE, van Gool WA, van der Mast RC, Kesecioglu J, Slooter AJ. Source. Department of Intensive Care Medicine, University Medical Centre, Utrecht, Netherlands. Abstract. BACKGROUND: Delirium is frequently diagnosed in critically ill patients and is associated with adverse outcome. Impaired cholinergic neurotransmission seems to have an important role in the development of delirium. We aimed to establish the effect of the cholinesterase inhibitor rivastigmine on the duration of delirium in critically ill patients. METHODS: Patients (aged ≥18 years) who were diagnosed with delirium were enrolled from six intensive care units in the Netherlands, and treated between November, 2008, and January, Patients were randomised (1:1 ratio) to receive an increasing dose of rivastigmine or placebo, starting at 0·75 mL (1·5 mg rivastigmine) twice daily and increasing in increments to 3 mL (6 mg rivastigmine) twice daily from day 10 onwards, as an adjunct to usual care based on haloperidol. The trial pharmacist generated the randomisation sequence by computer, and consecutively numbered bottles of the study drug according to this sequence to conceal allocation. The primary outcome was the duration of delirium during hospital admission. Analysis was by intention to treat. Duration of delirium was censored for patients who died or were discharged from hospital while delirious. Patients, medical staff, and investigators were masked to treatment allocation. Members of the data safety and monitoring board (DSMB) were unmasked and did interim analyses every 3 months. This trial is registered with ClinicalTrials.gov, number NCT FINDINGS: Although a sample size of 440 patients was planned, after inclusion of 104 patients with delirium who were eligible for the intention-to-treat analysis (n=54 on rivastigmine, n=50 on placebo), the DSMB recommended that the trial be halted because mortality in the rivastigmine group (n=12, 22%) was higher than in the placebo group (n=4, 8%; p=0·07). Median duration of delirium was longer in the rivastigmine group (5·0 days, IQR 2·7-14·2) than in the placebo group (3·0 days, IQR 1·0-9·3; p=0·06). INTERPRETATION: Rivastigmine did not decrease duration of delirium and might have increased mortality so we do not recommend use of rivastigmine to treat delirium in critically ill patients. Accessed March Van Eijk MM, et al. Lancet ;376(9755):")
77
Before Considering a Pharmacologic Treatment for Delirium…
Does your patient have delirium? Assessed with scale? Which type of delirium? Hyperactive Hypoactive Mixed hyperactive-hypoactive Have the underlying causes of delirium been identified and reversed/treated? Have non-pharmacologic strategies been optimized? Inouye SK, et al. N Engl J Med. 1999;340:

78
Antipsychotic Therapy
Rule Out Dementia Antipsychotic drugs are not approved for the treatment of dementia-related psychosis No drug is approved for dementia-related psychosis Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death Physicians considering antipsychotics for elderly patients with dementia-related psychosis should discuss this increased risk of mortality with their patients, patients’ families, and caregivers Antipsychotics. Accessed March 2012.

79
ABCDE Awakening Breathing Coordination/ Choice of Sedation Delirium Monitoring and Management Early Mobilization

80
Early Mobilization Patient Selection
Inclusion criteria Medical ICU Adults (≥ 18 years of age) On MV < 72 h, expected to continue for at least 24 h Met criteria for baseline functional independence (Barthel Index score ≥ 70) Exclusion criteria Rapidly developing Neuromuscular disease Cardiopulmonary arrest Irreversible disorders with estimated 6-month mortality > 50% Raised intracranial pressure Absent limbs Enrollment in another trial Schweickert WD, et al. Lancet. 2009;373:
 On MV < 72 h, expected to continue for at least 24 h. Met criteria for baseline functional independence (Barthel Index score ≥ 70) Exclusion criteria. Rapidly developing. Neuromuscular disease. Cardiopulmonary arrest. Irreversible disorders with estimated 6-month mortality > 50% Raised intracranial pressure. Absent limbs. Enrollment in another trial. Schweickert WD, et al. Lancet. 2009;373:")
81
Early Mobilization Trial Design
104 sedated patients with daily interruption Early exercise and mobilization (PT & OT; intervention; n = 49) PT & OT as ordered by the primary care team (control; n = 55) Primary endpoint: number of patients returning to independent functional status at hospital discharge Ability to perform 6 activities of daily living Ability to walk independently Assessors blinded to treatment assignment Secondary endpoints Duration of delirium during first 28 days of hospital stay Ventilator-free days during first 28 days of hospital stay Schweickert WD, et al. Lancet. 2009;373:
 PT & OT as ordered by the primary care team (control; n = 55) Primary endpoint: number of patients returning to independent functional status at hospital discharge. Ability to perform 6 activities of daily living. Ability to walk independently. Assessors blinded to treatment assignment. Secondary endpoints. Duration of delirium during first 28 days of hospital stay. Ventilator-free days during first 28 days of hospital stay. Schweickert WD, et al. Lancet. 2009;373:")
82
Perform Safety Screen First
*Range of motion may be started in comatose patients, but not considered Early Exercise/Mobility Pass Fail Exercise/Mobility Therapy Too Ill for Exercise/Mobility Schweickert WD, et al. Lancet. 2009;373:

83
Early Mobilization Protocol: Result
Return to independent functional status at discharge 59% in intervention group 35% in control group (P = 0.02) Schweickert WD, et al. Lancet. 2009;373:
 Schweickert WD, et al. Lancet. 2009;373:")
84
Early PT and OT in Mechanically Ventilated ICU Patients
All Patients P = 0.93 P = 0.08 P = 0.02 P = 0.02 Two center trial of 104 adult patients on mechanical ventilation for less than 72 hrs, randomized to early exercise and mobilization (PT and OT) during periods of daily interruption of sedation or to daily interruption of sedation with therapy as ordered by the primary care team. Schweickert WD, et al. Lancet. 2009;373(9678):
 during periods of daily interruption of sedation or to daily interruption of sedation with therapy as ordered by the primary care team. Schweickert WD, et al. Lancet. 2009;373(9678):")
85
Protocol for Early Mobility Therapy Acute Respiratory Failure Patients
Morris PE, et al. Crit Care Med. 2008;36(8):
:")
86
Early Mobility Therapy Results
Primary Endpoint: more protocol patients received PT than did usual care (80% vs. 47%, P ≤ 0.001) Usual Care* (n = 135) Protocol* (n = 145) P-Value Days to first out of bed 11.3 5.0 0.001 Ventilator days 10.2 8.8 0.163 ICU LOS days 6.9 5.5 0.025 Hospital LOS days 14.5 11.2 0.006 * Values adjusted for BMI, Acute Physiology & Chronic Health Evaluation II, and vasopressor Morris PE, et al. Crit Care Med. 2008;36(8):
 Usual Care* (n = 135) Protocol* (n = 145) P-Value. Days to first out of bed Ventilator days ICU LOS days Hospital LOS days * Values adjusted for BMI, Acute Physiology & Chronic Health Evaluation II, and vasopressor. Morris PE, et al. Crit Care Med. 2008;36(8):")
87
Post-Intensive Care Syndrome (PICS)
SCCM Task Force on Long-Term Outcomes “Post-intensive care syndrome (PICS) was agreed upon as the recommended term to describe new or worsening problems in physical, cognitive, or mental health status arising after a critical illness and persisting beyond acute care hospitalization. The term could be applied to either a survivor or family member- PICS-F.” A task force was convened by the Society of Critical Care Medicine to address the long-term outcomes from critical illness. Key stakeholders were invited to participate from healthcare agencies, disciplines of palliative care, rehabilitative therapy, physiatrists, hospitalists and research funding agencies. The research was reviewed. Future directions were planned. It was clear that more attention needs to be made to assess, treat, and prevent the long-term consequences of critical illness. This means partnering with our colleagues outside of the ICU to provide smooth transitions across levels of acuity during handoffs. The major implications during the ICU stay are family inclusion in care and communication, appropriate sedation and early mobility while maintaining cognitive activities. Needham DM, et al. Crit Care Med. 2012;40(2):
 was agreed upon as the recommended term to describe new or worsening problems in physical, cognitive, or mental health status arising after a critical illness and persisting beyond acute care hospitalization. The term could be applied to either a survivor or family member- PICS-F. A task force was convened by the Society of Critical Care Medicine to address the long-term outcomes from critical illness. Key stakeholders were invited to participate from healthcare agencies, disciplines of palliative care, rehabilitative therapy, physiatrists, hospitalists and research funding agencies. The research was reviewed. Future directions were planned. It was clear that more attention needs to be made to assess, treat, and prevent the long-term consequences of critical illness. This means partnering with our colleagues outside of the ICU to provide smooth transitions across levels of acuity during handoffs. The major implications during the ICU stay are family inclusion in care and communication, appropriate sedation and early mobility while maintaining cognitive activities. Needham DM, et al. Crit Care Med. 2012;40(2):")
88
PICS Consequences Post Intensive Care Syndrome (PICS) Family (PICS-F)
Mental Health Anxiety/ASD PTSD Depression Complicated Grief Survivor (PICS) Cognitive Impairments Executive Function Memory Attention Physical Impairments Pulmonary Neuromuscular Physical Function Needham DM, et al. Crit Care Med. 2012;40(2): Desai SV, et al. Crit Care Med. 2011;39(2): Davidson JE, et al. Crit Care Med. 2012;40(2):
 Cognitive Impairments. Executive Function. Memory. Attention. Physical Impairments. Pulmonary. Neuromuscular. Physical Function. Needham DM, et al. Crit Care Med. 2012;40(2): Desai SV, et al. Crit Care Med. 2011;39(2): Davidson JE, et al. Crit Care Med. 2012;40(2):")
89
Benefits of ABCDE Protocol
Morandi A, et al. Curr Opin Crit Care. 2011;17:43-49.

90
Quality Improvement Project: Implementing ABCDE
Multidisciplinary team focused on reducing heavy sedation, using SAT-SBT protocol and increasing MICU staffing to include full-time physical and occupational therapists with new consultation guidelines Results: Delirium decreased Sedation use decreased Physical mobility improvement Decrease hospital length of stay Increased MICU admissions Needham DM, et al. Arch Phys Med Rehabil. 2010;91(4): Needham DM, et al. Top Stroke Rehabil. 2010;17(4):
: Needham DM, et al. Top Stroke Rehabil. 2010;17(4):")
91
Results of ICU Quality Initiative
Top Stroke Rehabil Jul-Aug;17(4): Rehabilitation quality improvement in an intensive care unit setting: implementation of a quality improvement model. Needham DM, Korupolu R. Source Division of Pulmonary & Critical Care Medicine, Johns Hopkins University, Baltimore, MD, USA. Abstract OBJECTIVE: There are barriers to providing early physical medicine and rehabilitation (PM&R) in the intensive care unit (ICU). We present a specific model for undertaking quality improvement (QI) projects and a case study focused on QI for early PM&R in the ICU. METHODS: The QI project was undertaken using a 4-step model: (1) summarizing the evidence, (2) identifying barriers, (3) establishing performance measures, and (4) ensuring patients receive the intervention. To evaluate the application and outcomes of this model, we present data collected during a 4-month QI period versus an immediately preceding 3-month control period. RESULTS: Deep sedation was a major barrier to early PM&R that was addressed in the QI project. Compared to the control period, there was a decrease in medical ICU (MICU) days with any benzodiazepine use (73% vs 96% of days, P = .03) and narcotic use (77% vs 96%, P = .05) and improved delirium status (MICU days without delirium, 53% vs 21%, P = .003). In addition, more QI patients had physical therapy consultations (93% vs 59%, P = .004) and greater number of rehabilitation treatments with higher functional mobility (treatments involving sitting or greater mobility, 78% vs 56%, P = .03). Hospital data for the QI period demonstrated a decrease in average length of stay in the MICU (4.9 vs 7.0 days, P = .02) and hospital (14.1 vs 17.2, P = .03) compared to the prior year. CONCLUSION: A structured QI model can be applied to implementation of early PM&R in the ICU resulting in markedly improved delirium status, delivery of PM&R, functional mobility, and length of stay. Needham DM, et al. Top Stroke Rehabil. 2010;17(4):
: Rehabilitation quality improvement in an intensive care unit setting: implementation of a quality improvement model. Needham DM, Korupolu R. Source. Division of Pulmonary & Critical Care Medicine, Johns Hopkins University, Baltimore, MD, USA. Abstract. OBJECTIVE: There are barriers to providing early physical medicine and rehabilitation (PM&R) in the intensive care unit (ICU). We present a specific model for undertaking quality improvement (QI) projects and a case study focused on QI for early PM&R in the ICU. METHODS: The QI project was undertaken using a 4-step model: (1) summarizing the evidence, (2) identifying barriers, (3) establishing performance measures, and (4) ensuring patients receive the intervention. To evaluate the application and outcomes of this model, we present data collected during a 4-month QI period versus an immediately preceding 3-month control period. RESULTS: Deep sedation was a major barrier to early PM&R that was addressed in the QI project. Compared to the control period, there was a decrease in medical ICU (MICU) days with any benzodiazepine use (73% vs 96% of days, P = .03) and narcotic use (77% vs 96%, P = .05) and improved delirium status (MICU days without delirium, 53% vs 21%, P = .003). In addition, more QI patients had physical therapy consultations (93% vs 59%, P = .004) and greater number of rehabilitation treatments with higher functional mobility (treatments involving sitting or greater mobility, 78% vs 56%, P = .03). Hospital data for the QI period demonstrated a decrease in average length of stay in the MICU (4.9 vs 7.0 days, P = .02) and hospital (14.1 vs 17.2, P = .03) compared to the prior year. CONCLUSION: A structured QI model can be applied to implementation of early PM&R in the ICU resulting in markedly improved delirium status, delivery of PM&R, functional mobility, and length of stay. Needham DM, et al. Top Stroke Rehabil. 2010;17(4):")
92
Results of ICU Quality Initiative (cont)
Top Stroke Rehabil Jul-Aug;17(4): Rehabilitation quality improvement in an intensive care unit setting: implementation of a quality improvement model. Needham DM, Korupolu R. Source Division of Pulmonary & Critical Care Medicine, Johns Hopkins University, Baltimore, MD, USA. Abstract OBJECTIVE: There are barriers to providing early physical medicine and rehabilitation (PM&R) in the intensive care unit (ICU). We present a specific model for undertaking quality improvement (QI) projects and a case study focused on QI for early PM&R in the ICU. METHODS: The QI project was undertaken using a 4-step model: (1) summarizing the evidence, (2) identifying barriers, (3) establishing performance measures, and (4) ensuring patients receive the intervention. To evaluate the application and outcomes of this model, we present data collected during a 4-month QI period versus an immediately preceding 3-month control period. RESULTS: Deep sedation was a major barrier to early PM&R that was addressed in the QI project. Compared to the control period, there was a decrease in medical ICU (MICU) days with any benzodiazepine use (73% vs 96% of days, P = .03) and narcotic use (77% vs 96%, P = .05) and improved delirium status (MICU days without delirium, 53% vs 21%, P = .003). In addition, more QI patients had physical therapy consultations (93% vs 59%, P = .004) and greater number of rehabilitation treatments with higher functional mobility (treatments involving sitting or greater mobility, 78% vs 56%, P = .03). Hospital data for the QI period demonstrated a decrease in average length of stay in the MICU (4.9 vs 7.0 days, P = .02) and hospital (14.1 vs 17.2, P = .03) compared to the prior year. CONCLUSION: A structured QI model can be applied to implementation of early PM&R in the ICU resulting in markedly improved delirium status, delivery of PM&R, functional mobility, and length of stay. Needham DM, et al. Top Stroke Rehabil. 2010;17(4):
: Rehabilitation quality improvement in an intensive care unit setting: implementation of a quality improvement model. Needham DM, Korupolu R. Source. Division of Pulmonary & Critical Care Medicine, Johns Hopkins University, Baltimore, MD, USA. Abstract. OBJECTIVE: There are barriers to providing early physical medicine and rehabilitation (PM&R) in the intensive care unit (ICU). We present a specific model for undertaking quality improvement (QI) projects and a case study focused on QI for early PM&R in the ICU. METHODS: The QI project was undertaken using a 4-step model: (1) summarizing the evidence, (2) identifying barriers, (3) establishing performance measures, and (4) ensuring patients receive the intervention. To evaluate the application and outcomes of this model, we present data collected during a 4-month QI period versus an immediately preceding 3-month control period. RESULTS: Deep sedation was a major barrier to early PM&R that was addressed in the QI project. Compared to the control period, there was a decrease in medical ICU (MICU) days with any benzodiazepine use (73% vs 96% of days, P = .03) and narcotic use (77% vs 96%, P = .05) and improved delirium status (MICU days without delirium, 53% vs 21%, P = .003). In addition, more QI patients had physical therapy consultations (93% vs 59%, P = .004) and greater number of rehabilitation treatments with higher functional mobility (treatments involving sitting or greater mobility, 78% vs 56%, P = .03). Hospital data for the QI period demonstrated a decrease in average length of stay in the MICU (4.9 vs 7.0 days, P = .02) and hospital (14.1 vs 17.2, P = .03) compared to the prior year. CONCLUSION: A structured QI model can be applied to implementation of early PM&R in the ICU resulting in markedly improved delirium status, delivery of PM&R, functional mobility, and length of stay. Needham DM, et al. Top Stroke Rehabil. 2010;17(4):")
93
Conclusions Untargeted sedation in the ICU is common, and it is associated with negative sequelae Be familiar with the ABCDE protocol Titrate all sedative medications using a validated assessment tool to keep patients comfortable and arousable if possible Use of benzodiazepines should be minimized 93

94
Conclusions Consider nonpharmacological management of delirium and reduce exposure to risk factors Typical and atypical antipsychotic medications may be used to treat delirium if nonpharmacological interventions are not adequate Early mobility in ICU patients decreases delirium and improves functional outcomes at discharge Recognize PICS exists for patients and families

95
Thanks

Similar presentations











>")
 monitoring State the key applications for BIS monitoring in the ICU Describe the impact.>")







. ii. The Behavioral.>")