Download presentation
Presentation is loading. Please wait.

1
Vomiting, Diarrhea & Constipation
Mark J. Koruda, MD Professor of Surgery

2
Assumptions Students understand the anatomy, embryology and physiology of the gastrointestinal tract.

3
Case 1 A 54-year-old woman presents with a two day history of crampy abdominal pain followed by episodes of bilious emesis. Important Items in the History? Previously hysterectomy for treatment of cervical cancer.

4
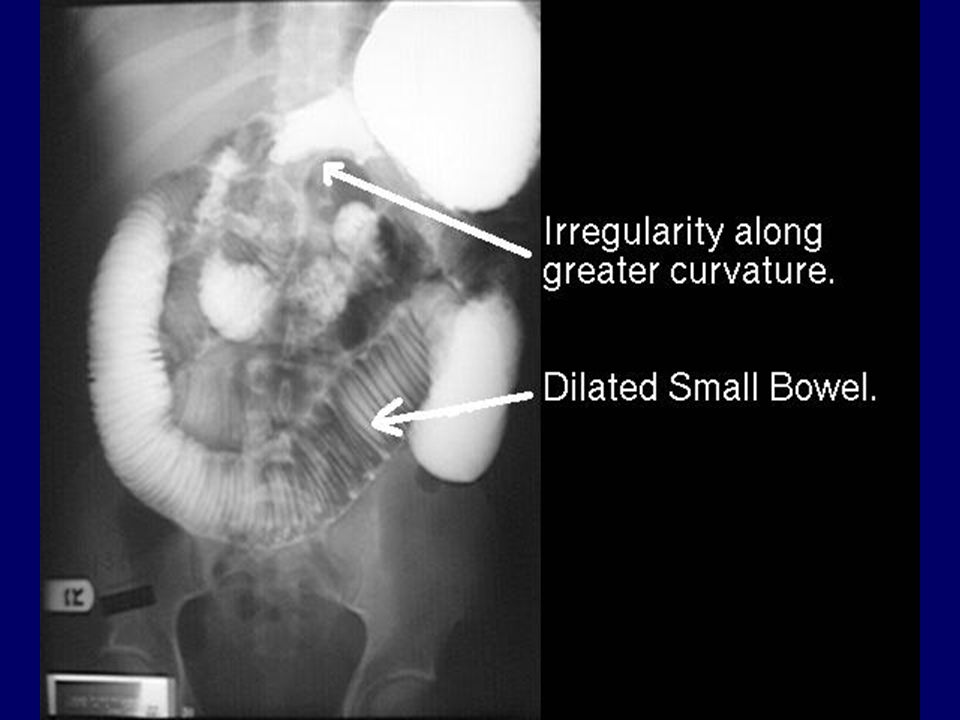
Small Bowel Obstruction

5
Small Bowel Obstruction Signs & Symptoms
Intermittent, Crampy Abdominal Pain Nausea / Emesis Distension Obstipation Peristaltic Rushes on Auscultation Focal Tenderness Diffuse Peritonitis

6
Case 1 What findings should be looked for on physical exam? Distended
No peritoneal signs

7
Case 1 What laboratory tests should be ordered?

8
Small Bowel Obstruction Laboratory Evaluation
May see hypochloremic, hypokalemic metabolic alkalosis if having frequent emesis (proximal obstruction). May see evidence of contraction alkalosis Increased H/H, BUN. WBC usually normal early.
. May see evidence of contraction alkalosis. Increased H/H, BUN. WBC usually normal early.")
9
Case 1 What laboratory tests should be ordered?
What diagnostic tests should be ordered?

10
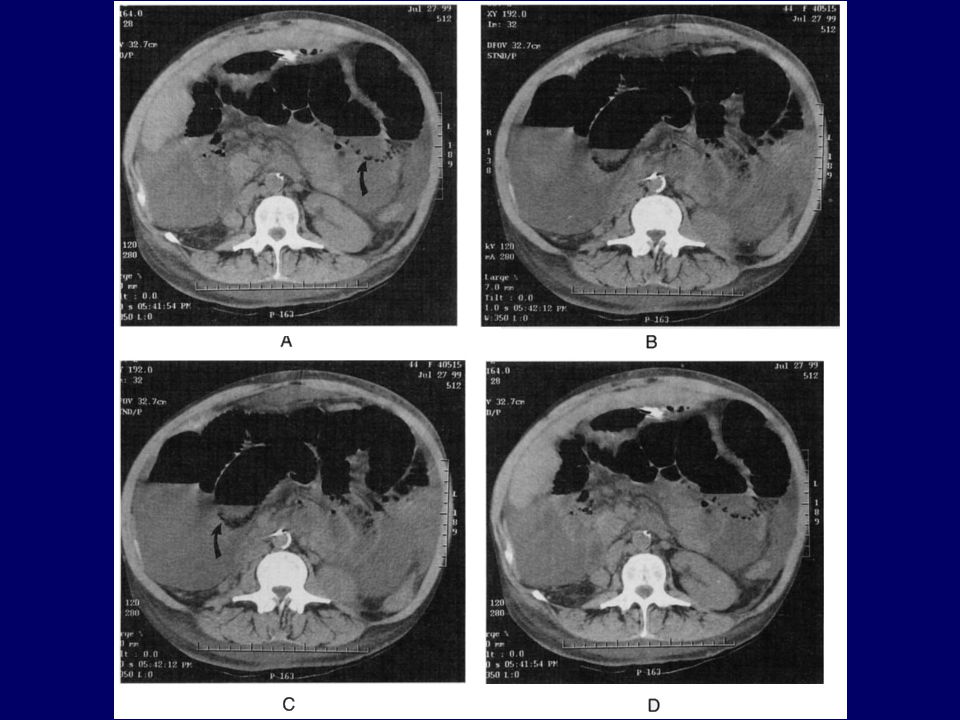
Small Bowel Obstruction Radiologic Evaluation
Xrays: ? AFLs, ? Free Air, ? Distal Gas UGI / SBFT: Identify mechanical obstruction Enteroclysis: Independent of gastric emptying CT Scan: ? Free Air, ? Pneumatosis, ? Tumor

15
Small Bowel Obstruction Etiologies
Adhesions Malignancy External or Internal Hernia Volvulus Crohn’s Disease Intra-abdominal Abscess

16
Small Bowel Obstruction Etiologies (Cont.)
Radiation Stricture Foreign Body Gallstone Ileus Meckel’s Diverticulum Intramural Hematoma Mesenteric Ischemia Intussusception

17
Intestinal Ileus Etiologies
Postoperative State Sepsis Electrolyte Imbalance Drugs Ureteral and Biliary Colic Retroperitoneal Hemorrhage Spinal Cord Injury Myocardial Infarction Pneumonia

18
Case 1 What is the initial management plan?

19
Small Bowel Obstruction Partial vs. Total
Why Not Just Wait?? Potential for Closed Loop Obstruction Risk of Ischemia / Perforation (4-6 hrs)
")
20
Small Bowel Obstruction Treatment
Correct intravascular volume deficit NGT vs. Miller-Abbott or Cantor Tubes Serial Exams Operation if no improvement or if signs of complete (closed loop) obstruction or incarceration. Evaluation of Bowel Viability
 obstruction or incarceration. Evaluation of Bowel Viability.")
22
Small Bowel Obstruction Special Cases
Early Postoperative SBO <1% risk in first month Must be considered after 7 days of “ileus” since adhesions become dense in 2-3 weeks. Recurrent SBO (5-15%) Malignant Obstruction Radiation Fibrosis
 Malignant Obstruction. Radiation Fibrosis.")
23
Case 2 A 72-year-old man presents with a two month history of gradually increasing constipation. Key Points in History?

24
Large Bowel Obstruction Diagnosis
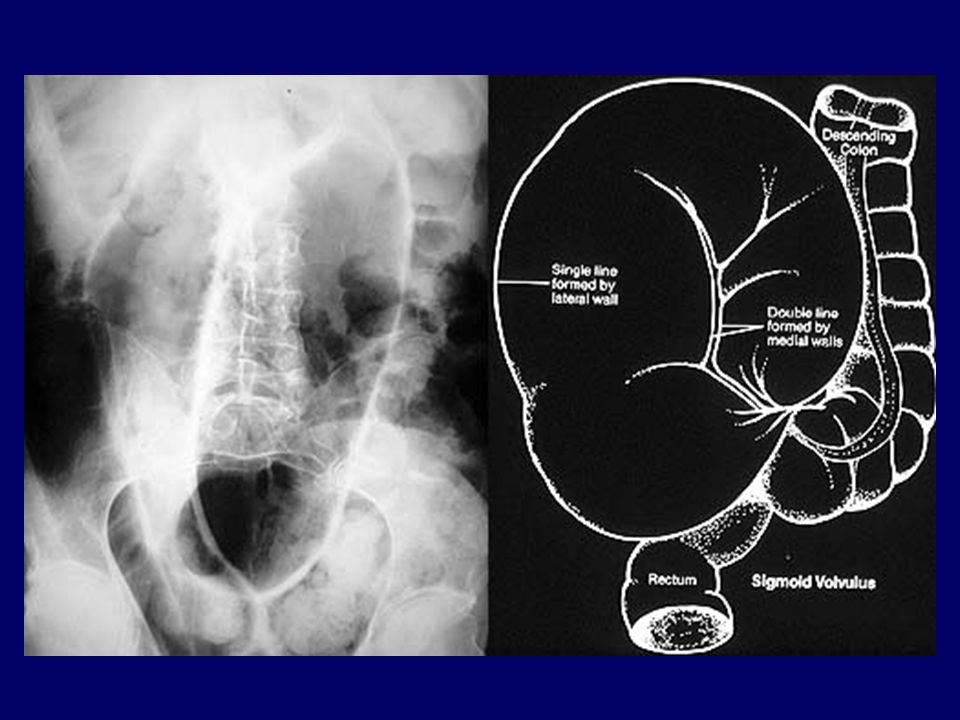
Crampy Pain Onset may be acute or insidious Distension (50-60% have competent ileo-cecal valve and develop severe distension) Xrays: cm cecum, perforation risk Contrast enema: Obstruction vs Oglive’s Consider rigid sigmoidoscopy to r/o and treat sigmoid volvulus
 Xrays: cm cecum, perforation risk. Contrast enema: Obstruction vs Oglive’s. Consider rigid sigmoidoscopy to r/o and treat sigmoid volvulus.")
25
Case 2 Physical Exam What further tests are indicated

26
Case 2 Differential Diagnosis Colonic Obstruction Colonic Dysfunction
Malignant Benign Colonic Dysfunction

27
Large Bowel Obstruction

28
Large Bowel Obstruction Etiologies
Colon Cancer Diverticulitis Extrinsic Cancer Fecal Impaction Intussusception Volvulus Incarcerated Hernias

29
Large Bowel Obstruction Colon Cancer
20% of colon cancers present with obstruction Left-sided lesions are more prone to obstruct (more narrow lumen, more solid fecal stream)
")
34
Large Bowel Obstruction Treatment
IVF NGT Operation Emergently if signs of peritonitis / perforation Prep bowel if possible Is an ostomy necessary? Right vs. Left-sided Lesions Traditional vs. Newer Attitudes right colon - can reanastamose transverse colon - extended right hemi left colon 3 stage (ostomy, resection, takedown) 2 stage (resect with protecting ostomy, takedown) 1 stage (resect, anastamose with or without colonic lavage) leak rate 5% 1 stage (resect whole colon and do an ileoproctostomy to avoid fecal loading)
 2 stage (resect with protecting ostomy, takedown) 1 stage (resect, anastamose with or without colonic lavage) leak rate 5% 1 stage (resect whole colon and do an ileoproctostomy to avoid fecal loading)")
35
Large Bowel Dysfunction
Inflammation Colonic Inertia Etc

37
Oglive’s Syndrome (Colonic Pseudo-Obstruction)
May mimic mechanical obstruction Associated Conditions Treatment: Rectal tube / enemas /exams (work in most) Colonoscopic decompression (80-90% eff.) Surgery (Cecostomy vs. Resection) - cecum >12 cm or peritoneal signs Associated Conditions: Amyloidosis Blunt trauma Cardiopulmonary Bypass C-section Chemotherapy Dermatofibrosis Diabetes Electrolyte abnormalities Hypothyroidism Medications (anticholinergics, ganglionic blockers, narcotics, phenothiazines, tricyclic antidepressants) Ortho or Neurologic Procedures Renal Failure RenalTransplantation Scleroderma Dementia / Stroke SLE
 Colonoscopic decompression (80-90% eff.) Surgery (Cecostomy vs. Resection) - cecum >12 cm or peritoneal signs. Associated Conditions: Amyloidosis. Blunt trauma. Cardiopulmonary Bypass. C-section. Chemotherapy. Dermatofibrosis. Diabetes. Electrolyte abnormalities. Hypothyroidism. Medications (anticholinergics, ganglionic blockers, narcotics, phenothiazines, tricyclic antidepressants) Ortho or Neurologic Procedures. Renal Failure. RenalTransplantation. Scleroderma. Dementia / Stroke. SLE.")
38
Case 3 A 54-yo Caucasian male with history of ileocolonic Crohn's disease, s/p ileocolectomy in 1979, who has not been on any Rx for CD. Presents to the UNC ER complaining of crampy abdominal pain that began at 8 hrs earlier located in the right lower and left lower quadrant. He also had nausea and vomiting as well as decreasing flatus associated. The patient stated his last BM was on the day of admission. He stated that the pain feels like his previous obstructions. Occurring every couple of months, recently increasing in frequency. No fevers. About 10 lb weight loss. Key Points in History

39
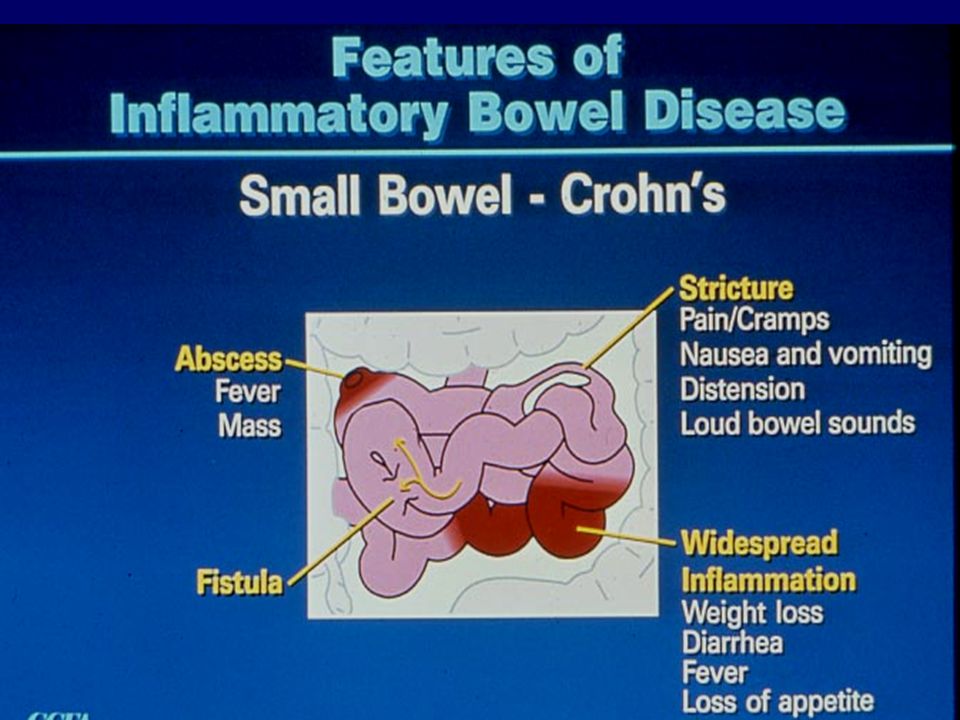
What Is Crohn’s Disease?
Crohn’s disease (CD) is an inflammatory bowel disorder that may affect any part of the gastro-intestinal (GI) tract The inflammation penetrates the lining of the GI tract and often causes ulcers to form Esophagus Small Intestine Stomach Large Intestine (Colon) Rectum Appendix
 is an inflammatory bowel disorder that may affect any part of the gastro-intestinal (GI) tract. The inflammation penetrates the lining of the GI tract and often causes ulcers to form. Esophagus. Small. Intestine. Stomach. Large. Intestine. (Colon) Rectum. Appendix.")
41
Case 3 Key Points in History

42
Case 3 Key Points in History Crohn’s disease Previous surgical history
No Crohn’s Rx Chronic symptoms Weight loss No fevers Crampy pain

43
Case 3 Physical Exam Diagnostic Studies? Differential Dx

44
Crohn’s Disease

45
Crohn’s Disease

46
Crohn’s Disease Medical vs Surgical Management

51
Case 4 22yo UNC student presents with 3 mos of increasing “bloody diarrhea”, going to the bathroom 15-20x/day. “It rules my life!” Key Points in History

52
Case 4 22yo UNC student presents with 3 mos of increasing “bloody diarrhea”, going to the bathroom 15-20x/day. “It rules my life!” Key Points in History Diarrhea Bleeding

53
Case 4 Physical Exam Diagnostic Studies?

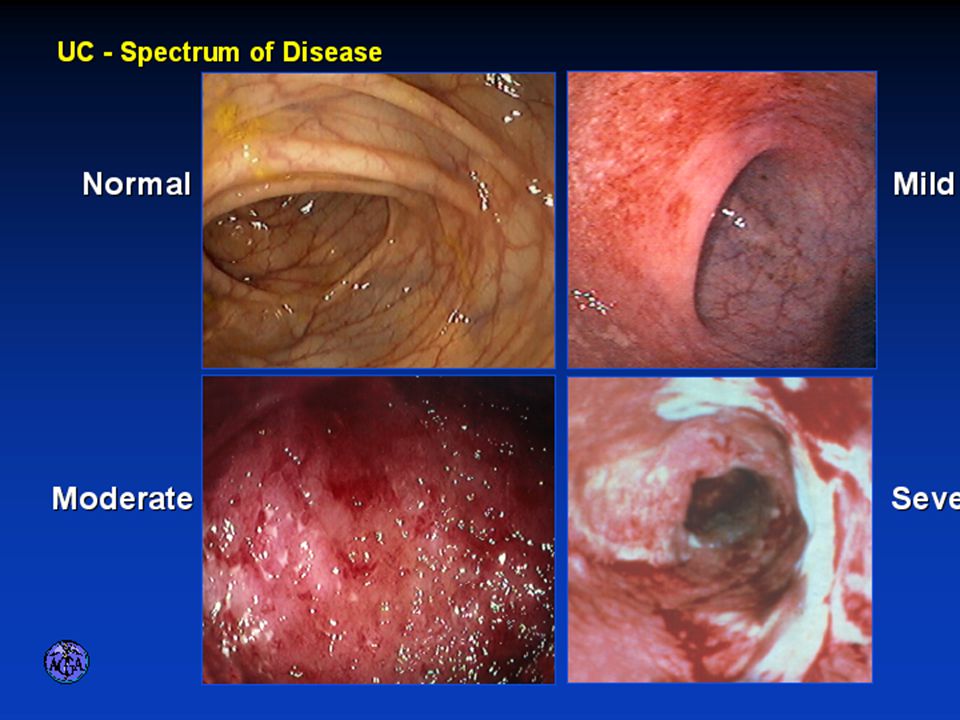
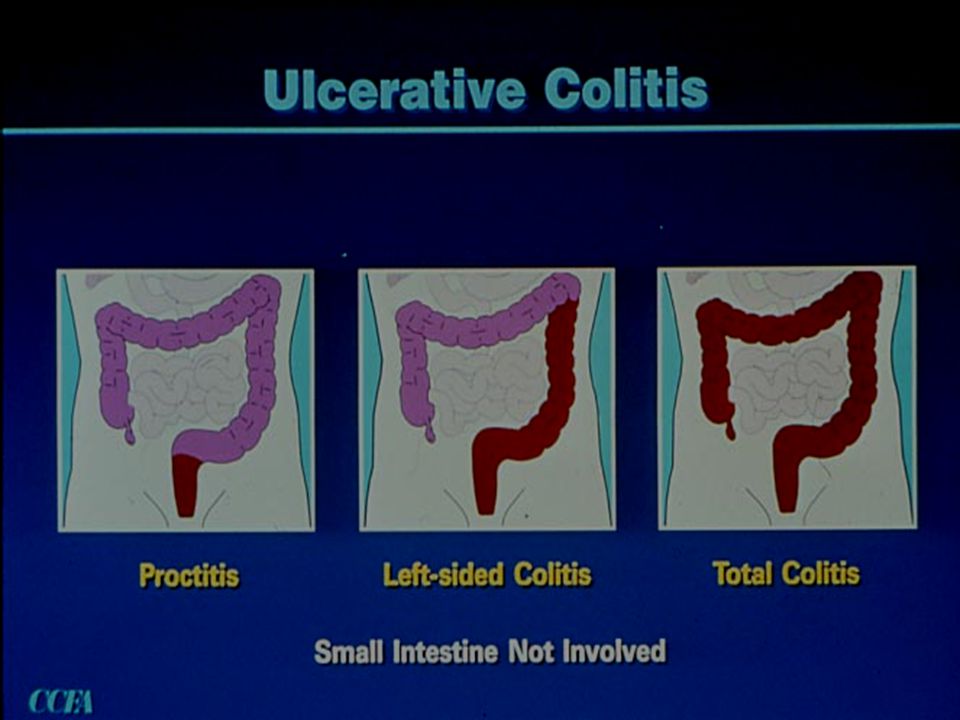
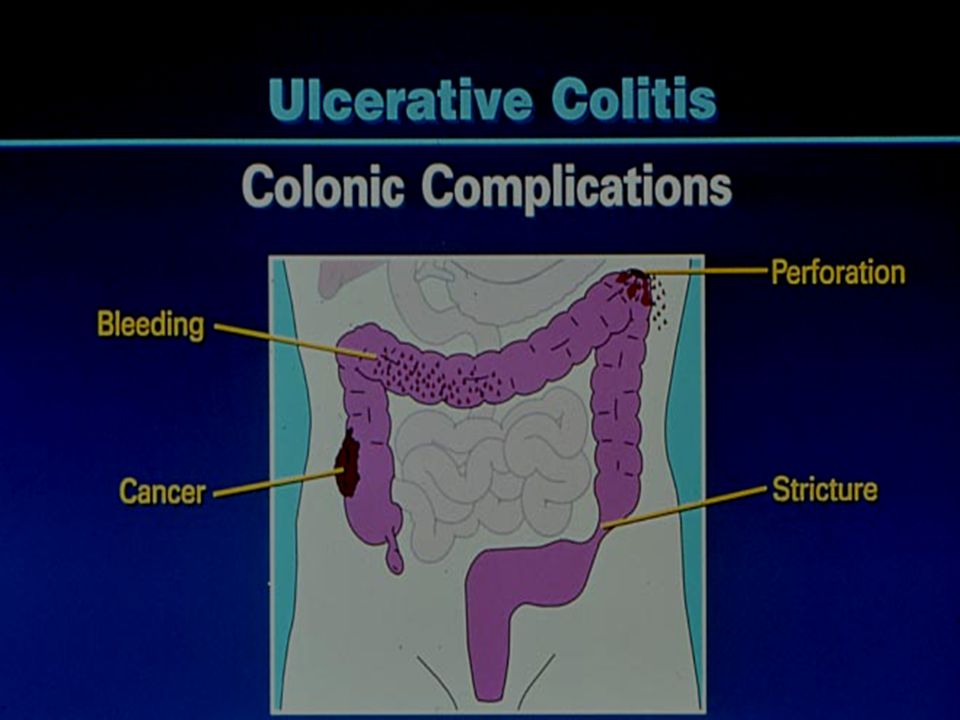
56
Ulcerative Colitis

Similar presentations