Download presentation
Presentation is loading. Please wait.

1
Gastric Obstruction post “Sleeve gastrectomy”
Hussein Mcheimech, MD

2
26 yr old female patient underwent laparoscopic sleeve gastrectomy 9 month ago, complaining of post prandial vomiting for the last 7 month . Dysphagia only to solids , with no other symptoms. Total weight loss since surgery = 60 kg

3
PSHx : laparoscopic sleeve gastrectomy 9 m ago Lap. Cholecystectomy 8 m ago PMHx: none NKDA To note a hiatal hernia is detected on follow up upper GI on day 2 post op.

4
Physical exam: no Abnormal findings.
Vitals signs within normal parameters. Abdomen : soft , bs + , non tender with no signs of organomegaly.

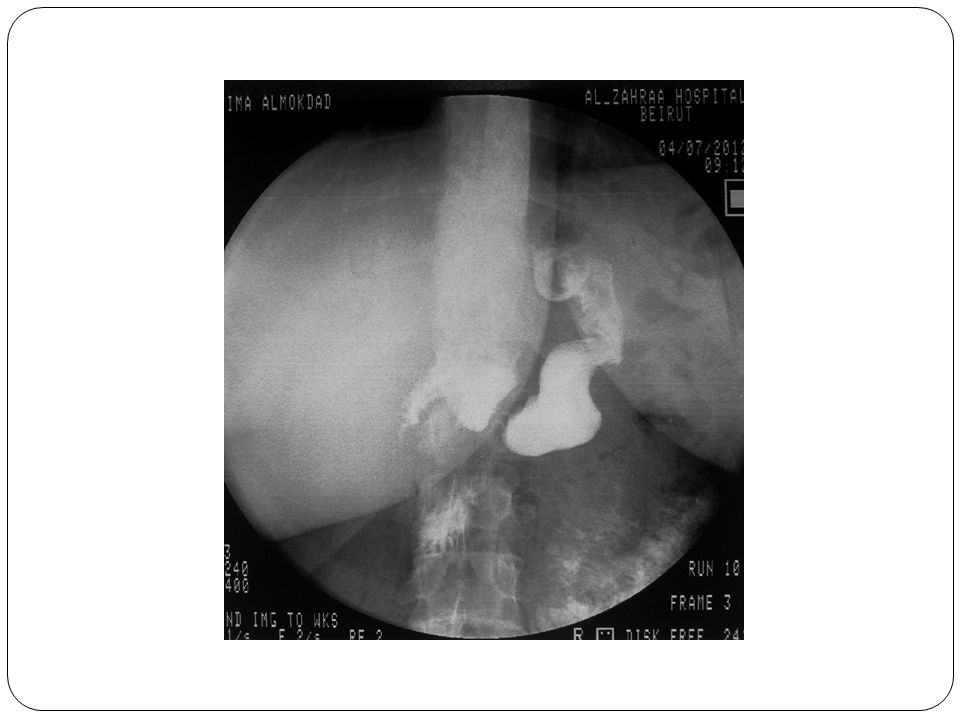
5
Upper GI at 2m post op

11
Gastroscopy

12
abdominal CT 8/2/13 Good esophageal passage of contrast
Presence of a 25mm stenotic not obstructive segment at the level of the stomach body To note food debris in the fundus after 6h of fasting.

18
Post op Upper GI

22
Report Passage of contrast from the stomach to the jejunal loop.
No passage of contrast thru the duodenum

23
Gastric outlet obstruction following sleeve gastrectomy

24
Complication rate of LSG : 0.7 – 4%
Gastric outlet obstruction less frequent than leaks. Rarely discussed in the literature.

25
Symptoms Dysphagia Nausea and vomiting
Symptoms of obstruction when moving from fluids to solid food Sticking to fluids consumption, not progressing to solids Saliva or food regurgitation Impaction of food (especially meat or bread) De novo gastroesophageal reflux disease symptoms
 De novo gastroesophageal reflux disease symptoms.")
26
Studies Upper GI will show : Endoscopy is the prefered modality
thin stenotic ring Kinking tortuosity in the sleeve lack of progression of the contrast column Endoscopy is the prefered modality An unsurpassable stretch of lumen when using a 9.8mm endoscope should be considered a stricture

27
Causes Early (Acute): gastric mucosal edema
external compression (mainly hematoma) Kinking at the incisura angularis (acute angle created by oversewing ) Late: Strictures (due to : pouch ischemia , retraction due to scarring) Adhesions.
 Kinking at the incisura angularis (acute angle created by oversewing ) Late: Strictures (due to : pouch ischemia , retraction due to scarring) Adhesions.")
28
Avoiding strictures Faucher tube, endoscope:
Allows a safe distance between the incisura angularis and the stapling edge. Prevents thru and thru stitching if oversweing is performed. Meticulous lesser curvature dissection Prevent ischemia Twisting of the gastric tube: Can be prevented by keepin a straight stappling line

29
Treatment: Surgery as last resort EXCEPT in the early post op period.
For early cases, surgery to : Manage a hematoma Release over sewn stitches relieve pressure or ischemia. in case of kinking , fixating the incisura.

30
Late cases Endoscopic balloon dilation:
In cases of stenosis or adhesions. 5 dilations as following: Last dilation + needle cautery cuts at 4 quadrants. 78 % success rate (7/9 pts, 5 stenosis , 2 adhesions)
")
32
Endoscopic stenting Eubanks et al and Scott 7-day period of stenting(success rate of 83% ( small sample n=6) Stents removed after 1 week due to pain. Dilation and stenting are contraindicated in cases of long segment stenosis. Final approach in case of failure: R en Y gastric bypass or total gastrectomy

33
Conclusion Gastric outlet obstruction following LSG is a rare complication. The condition presents as early or late Early obstruction is surgery dependant Late presentation is dependant on the patient’s attitude, inflammation, fibrosis as well as surgical technique.

34
Treatment should be tailored to each patient.
The most effective treatment is conversion to Roux en Y gastric bypass loop bypass with or without gastrectomy

Similar presentations
























>")







