Download presentation
Presentation is loading. Please wait.

1
Haney A. Mallemat, MD Department of Critical Care Dartmouth-Hitchcock Medical Center

2
77 M AAA repair POD #3 Extubated Stable vitals Hb 8.1

3
2U PRBC No indication documented

5
Respiratory distress 85% sat 85/50 P: 125 STAT Airway Levophed

7
Definition Epidemiology Pathogenesis Diagnosis Treatment Prognosis

8
Definition Epidemiology Pathogenesis Diagnosis Treatment Prognosis

9
Pulmonary Hypersensitivity Reaction Allergic Pulmonary Edema Non-Cardiogenic Pulmonary Edema Pulmonary Leucoagglutinin Reaction

10
Transfusion-Associated Popovoskitis

11
TR ansfusion A ssociated L ung I njury

12
No formal definition

13
ALI from blood products P/F ratio <300 B/L infiltrates No circulatory overload No previous ALI No causes ALI

14
“Classic” TRALI < 6 h ▪ ~30-120 min “Delayed” TRALI 6 – 72 h

15
Definition Epidemiology Pathogenesis Diagnosis Treatment Prognosis

16
#1 transfusion-related mortality >Infection >ABO mismatch Under recognized / reported Mortality 5-10%

17
PRBC 1 in 5000 Plasma 1 in 2000 Platelets 1 in 2000 IVIG Cryoprecipitate Stem cells

18
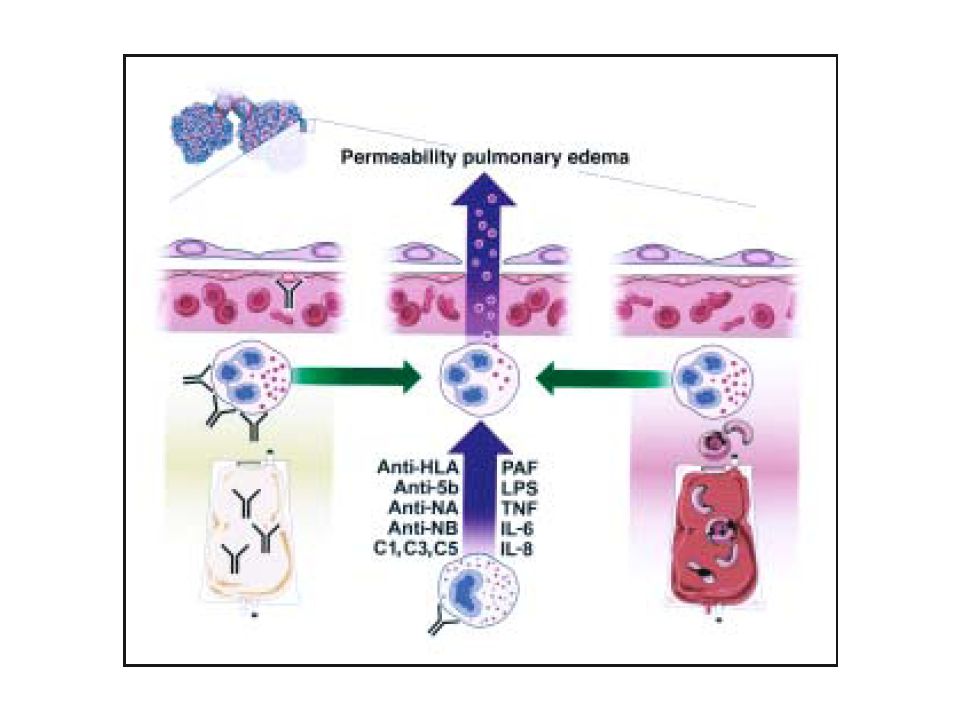
HOST M = F Recent surgery Active infections Recent transfusion Cytokine treatment Thrombocytopenia Increased age Ethanol use Tobacco Severe illness DONOR Multi-parous female donors Prolonged blood storage

19
Definition Epidemiology Pathogenesis Diagnosis Treatment Prognosis

20
1. Anti-granulocyte antibody 2. Endothelial-cell priming 3. “Two-hit” hypothesis

23
Definition Epidemiology Pathogenesis Diagnosis Treatment Prognosis

24
Mild symptoms Death

25
Fever Dyspnea Tachypnea Tachycardia Hypotension Hypertension No lung findings Crackles Retractions No S3 Frothy sputum Cough No JVD No cardiomegaly Non-cardiac edema Leukopenia Thrombocytpoenia Hyponatremia

28
<6 hours Hypoxemia P/F <300 O2sat <90% B/l infiltrates No evidence of HF

30
Aspiration Pneumonia Toxic inhalation Lung contusion Near drowning Severe sepsis Shock Trauma Burns Pancreatitis Bypass surgery Drug overdose

31
CHF Nephrotic syndrome Fluid overload Post-sepsis ESRD AKI

32
Frothy sputum Hypoxia Tachycardia Hypotension Fever

33
CXR

35
Rare and subtle diagnosis Subtlety is your specialty Notice changes first Key to diagnosis Stick to your guns

37
Definition Pathogenesis Epidemiology Diagnosis Treatment Prognosis

38
Stop transfusion! Report reaction Supportive Care

39
Hemodynamic support Fluids +/- pressors No diuresis! “Wet” CXR confusing Ventilatory support NIPPV vs. Intubate Lung protective strategy

40
Need transfusion? Single donor units Leukodepleted blood Newer blood

41
Definition Pathogenesis Epidemiology Diagnosis Treatment Prognosis

42
Live

43
Die

44
Recovery 24 – 96 No long-term sequelae CXR lingers

47
Transfusion + Clinical decline = TRALI

48
What is the #1 cause of #1 transfusion related mortality? What transfusion reaction is very under reported and under-recognized? What can any blood product cause? What should you think about if there is any clinical change within 6 hours of transfusion? Who is the most important person to recognize TRALI?

49
Supportive Good prognosis Question all transfusions!

Similar presentations












 line inserted into one of your blood.>")
 1:100 TACO1:100 TRALI1:5,000 Sepsis1:5,000 Acute hemolytic1:75,000 HBV1:160,000.>")




 – Leukocytes (WBCs) – Thrombocytes (platelets) Plasma – 90% water – 10% solutes – Proteins,>")

 presents to the Emergency Room with a 2 day history of weakness.>")
 Dr. Meg-angela Christi Amores.>")




: Clinical and Laboratory Aspects David Stroncek, MD Chief, Laboratory Services Section Department of Transfusion.>")



