Download presentation
Presentation is loading. Please wait.

1
ACUTE MESENTERIC ISCHEMIA Chirag Patel, MS III St. George’s University SOM Woodhull Medical Center Department of Surgery Clerkship October 25, 2011

2
BACKGROUND AMI syndrome is where there is inadequate blood flow through mesenteric circulation causing ischemia and eventual gangrene of the bowel wall. Overall Prevalence of AMI is 0.1% of all hospital admissions In the last 15 years, mortality rate from AMI averaged as high as 71%. Once bowel wall infarction has occurred, it is as high as 90%.

4
PATHOPHYSIOLOGY Damage ranges from reversible ischemia to transmural infarction with necrosis and perforation. Tissue injury via two mechanisms: (1) ischemic injury to the bowel or (2) reperfusion injury due to oxygen free radical release by leukocytes Arterial insufficiency tissue hypoxia bowel wall reactive spasm vomiting or diarrhea. As hypoxia worsens, bowel wall becomes edematous and cyanotic. Mucosal sloughing may show as blood in the stool.
 ischemic injury to the bowel or (2) reperfusion injury due to oxygen free radical release by leukocytes Arterial insufficiency tissue hypoxia bowel wall reactive spasm vomiting or diarrhea. As hypoxia worsens, bowel wall becomes edematous and cyanotic. Mucosal sloughing may show as blood in the stool..")
5
PATHOPHYSIOLOGY The intestine is able to compensate for about 75% acute reduction in flow for up to 12 hours without substantial injury due to increased oxygen extraction. Within 4 hours after ischemia begins, the mucosal villi become necrotic. As early as 6 hours, full-thickness infarction can be observed Transmural necrosis leads to peritoneal signs which as you would expect has a much worse prognosis.

6
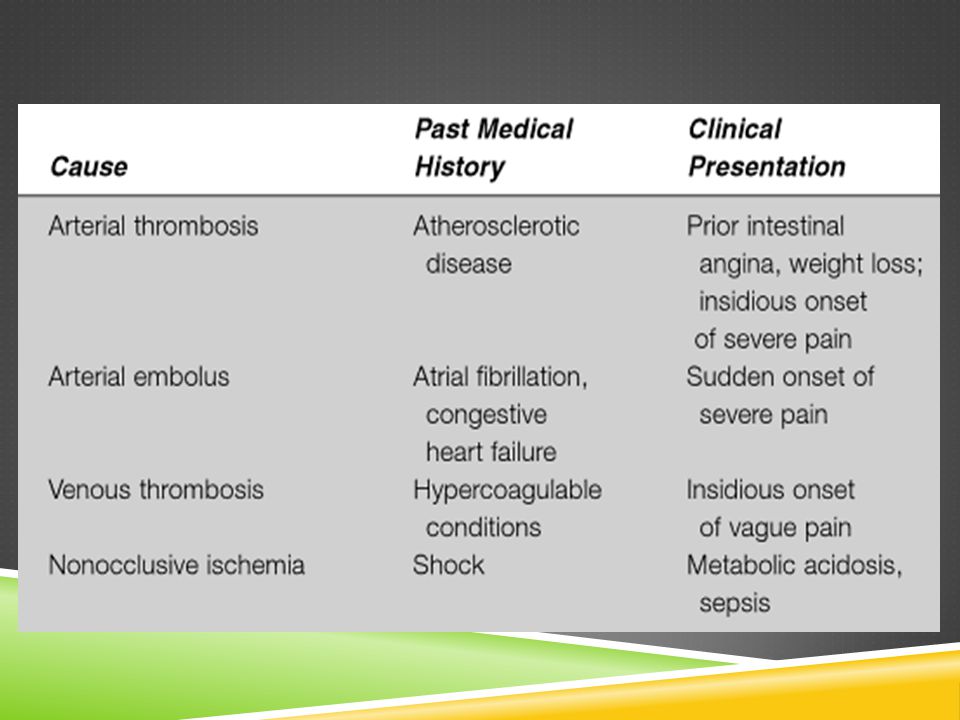
ETIOLOGY Arterial Embolic Disease(50%) Arterial Thrombotic Disease (25%) Non-occlusive Mesenteric Ischemia (20%) Venous Thrombotic Disease (<10%)
 Arterial Thrombotic Disease (25%) Non-occlusive Mesenteric Ischemia (20%) Venous Thrombotic Disease (<10%)")
7
ARTERIAL EMBOLISM Sources of Emboli: Cardiac Emboli (most common)- Mural thrombus after MI, thrombus associated with mitral stenosis and atrial fibrillation, septic emboli from endocarditis Fragments of proximal aortic thrombus due to ruptured atheromatous plaque Vascular occlusion is sudden, so the patient has no chance to develop compensatory increase in collateral flow. Thus, they experience worse ischemia than arterial thrombosis patients.

8
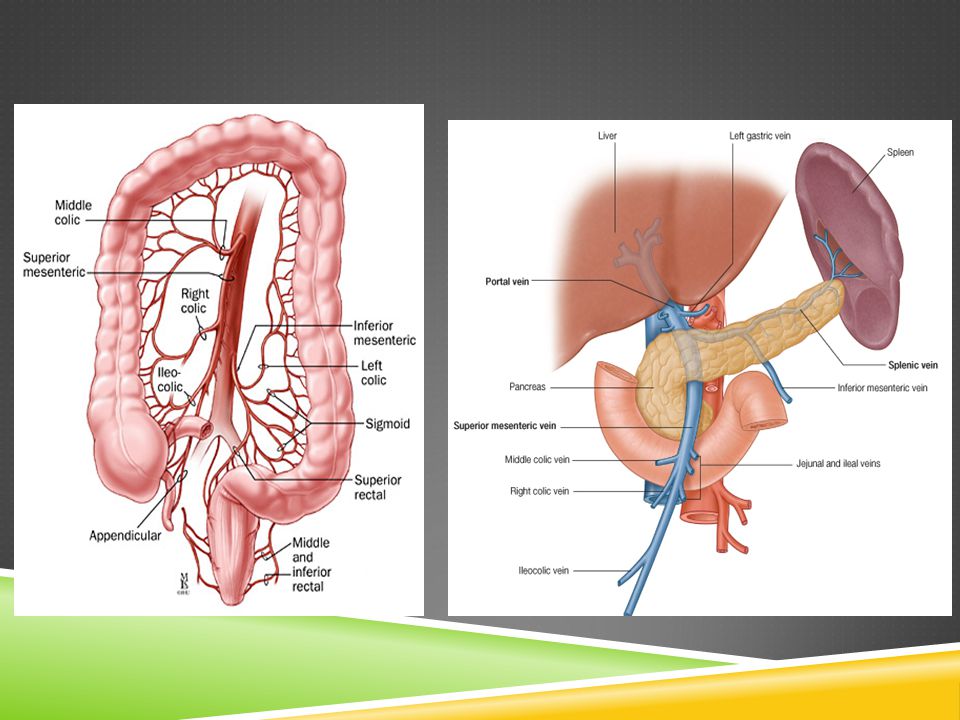
SMA is most susceptible because of its small 45 degree take-off angle from the aorta and because of its large caliber. Most commonly occludes near or at origin of middle colic artery- middle segment of jejunem most often involved

9
ARTERIAL THROMBOSIS Causes: Atherosclerotic vascular disease (most common) Aortic aneurysm, dissection, Abdominal trauma or infection Tends to occur at the origin of the SMA off the aorta, thus causing a widespread infarction. Usually a superimposed phenomenon in patients with history of chronic intestinal ischemia from progressive atherosclerosis. May also show atherosclerosis at other sites such as Coronary Artery Disease, Strokes, Peripheral Arterial Disease. They also frequently present with history of Chronic mesenteric ischemia (intestinal angina).
..")
10
NON-OCCLUSIVE Causes – Hypotension from CHF, MI, sepsis, aortic insufficiency, severe liver or renal disease, recent major cardiac or abdominal surgery – Diuretics, Digitalis, Vasopressive drugs, Ergotamines, Cocaine Any patient who takes digitalis and diuretics and who complains of abdominal pain must be considered to have nonocclusive ischemia until proven otherwise

11
VENOUS THROMBOSIS Causes Hypercoagulability from Polycythemia vera (most common), Pregnancy, OCP use Tumor causing venous compression or hypercoagulability Portal hypertension, Pancreatitis, Sickle Cell disease, s/p splenectomy Often affects a much younger population. Ischemia occurs due to resistance to venous flow, causing bowel wall edema, fluid efflux into bowel lumen with resulting systemic hypotension and increased blood viscosity. Arterial flow is diminished leading to hemorrhage and infarction.

12
PRESENTATION Classic finding: severe diffuse abdominal pain, which is out of proportion to physical exam findings. Nausea, vomiting, diarrhea Early: Abdominal exam may be normal or only reveals abdominal distension or occult blood in stool. No peritoneal signs (which makes the pain seem out of proportion). Later, as transmural bowel infarction develops, the abdomen becomes grossly distended, absent bowel sounds, and peritoneal signs develop.
. Later, as transmural bowel infarction develops, the abdomen becomes grossly distended, absent bowel sounds, and peritoneal signs develop..")
14
DIAGNOSIS Depends on high clinical suspicion, especially in patients with known risk factors such as atrial fibrillation, congestive heart failure, peripheral vascular disease, or history of hypercoagulability. Diagnosis and treatment before infarction occurs is the key to significantly decrease mortality. For this reason, high clinical suspicion of mesenteric ischemia should take preference over diagnostic tests, which would actually delay treatment.

15
INITIAL MANAGEMENT Resuscitation: make every effort to improve cardiovascular status. – Provide Oxygen to maintain 96-99% saturation. – Fluid resuscitation via isotonic normal saline and blood products. – Discontinue/Avoid vasopressors. Insert a NGT for gastric decompression Broad spectrum antibiotics, ie. Clindamycin, Metronidazole, Cefotetan, Cefoxitin Pain control via morphine Once patient is hemodynamically stable, labs and studies may be done. Peritonitis signs such as guarding and rebound tenderness are indications for emergency exploratory laparotomy and resection of infarcted bowel.

16
LABS Nonspecific. Helpful in confirming suspicion if significant, but normal labs do not exclude AMI With serious suspicion of AMI, radiographic studies should be performed without waiting for lab results. Any patient with acute abdominal pain and metabolic acidosis has intestinal ischemia until proven otherwise. Findings may include: Marked leukocytosis and/or left shift Elevated hemaocrit d/t hemoconcentration via third spacing; but decreases with GI bleeding Metabolic acidosis and elevated lactate late in course Elevated serum amylase

17
RADIOGRAPHIC STUDIES

18
ABDOMINAL X-RAY Often normal in presence of AMI, but it is used to exclude other causes of abdominal pain such as perforated viscus with free intraperitoneal air. Positive findings are late and nonspecific: ileus with distended bowel loops, edematous or thickened bowel walls, pneumatosis intestinalis (ie. Submucosal gas), thumbprinting of bowel wall, portal vein gas, air-fluid levels.
, thumbprinting of bowel wall, portal vein gas, air-fluid levels..")
19
ABDOMINAL X-RAY Thumbprinting of the bowel Distended featureless loops of small bowel with wall thickening (arrow) and separation of the bowel loops. These findings are consistent with hemorrhage into the bowel wall secondary to ischemia.

20
CT AND CT ANGIOGRAPHY Arterial occlusion shown via nonenhancement of vessels. CT Angiography has sensitivity of 71-96% and specificity of 92- 94% for AMI. It is noninvasive, readily available. The preferred modality for Mesenteric Venous Thrombosis (90% sensitivity)- failure to opacify mesenteric veins with IV conrast. Most commonly at SMV or Portal Vein Also can show bowel wall edema (most common finding), pneumatosis intestinalis, portal vein gas, thumbprinting, streaking of mesentery.
- failure to opacify mesenteric veins with IV conrast. Most commonly at SMV or Portal Vein Also can show bowel wall edema (most common finding), pneumatosis intestinalis, portal vein gas, thumbprinting, streaking of mesentery..")
21
CT & CT ANGIOGRAPHY Contrast-enhanced CT scan demonstrates extensive air within the anterior wall of the small bowel due to ischemic bowel. Acute thrombosis of SMV.

22
ANGIOGRAPHY Gold standard for diagnosis of AMI (88% sensitivity). Also important for pharmacologic infusion therapy via papaverine and thrombolytics. Findings: Embolus: sharp cutoff of flow near origin of middle colic arery. Thrombus: more tapered occlusion near origin of SMA. Non-occlusive: narrowing of the origins of multiple SMA branches. Alternating dilations and narrowing= ‘String of Sausages’ sign, spasm of arcades Second line study in Mesenteric Venous Thrombosis. May show thrombus at SMV, reflux of contrast into aorta, prolonged arterial phase with accumulation of contrast and thickened bowel walls, extravasation of contrast into bowel lumen, filling defect in portal vein or complete lack of venous phase.

23
ANGIOGRAPHY Superior mesenteric embolus. Abrupt occlusion of the SMA distal to jejunal branches. Contrast angiograms of aorta and mesenteric vessels with nonocclusive mesenteric ischemia. (a) SMA demonstrates distal spasm (b) SMA after intra-arterial papaverine infusion demonstrates improved filling of distal branches
 SMA demonstrates distal spasm (b) SMA after intra-arterial papaverine infusion demonstrates improved filling of distal branches.")
24
ULTRASONOGRAPHY Duplex US is highly specific(92-100%) but not as sensitive(70-89%) as angiography. Cannot detect clots beyond proximal main vessels, and cannot be used to diagnose nonocclusive mesenteric ischemia. Second line study for AMI

25
MRI AND MRA Yield findings similar to those of CT in AMI MRI 100% sensitive and 91% specific. Drawbacks are expense and time required.

26
TREATMENT & CARE Papaverine is useful for all forms of AMI. It relieves the reactive vasospasm in occluded arterial vessels and is the only treatment for nonocclusive ischemia other than resection of grangrenous bowel. Thrombolytics through angiography catheter is risky and should only be given if peritonitis or other signs of bowel necrosis are absent. Heparin anticoagulation is the main treatment of mesenteric venous thrombosis. If no signs of bowel necrosis, patient may not even need operation. Monitor PTT. Later switch patient from heparin to warfarin for at least 6 months, and possibly life-long if permanent hypercoaguble state. Maintain INR in 2-3 range.

27
SURGICAL CARE Before operative management, stabilize the patient via IV fluids, antibiotic prophylaxis, NGT decompression, Foley, heparin or papaverine administration, and blood should be available. In all types of AMI, necrotic bowel resection is required if peritonitis develops. Viable vs. Nonviable bowel can be differentiated via intraoperative fluroescein administration. Viable bowel fluoresces brightly under a Wood lamp. Most patients can benefit from a 24-48 hour “second-look” laparotomy to assess viability of questionable areas of bowel.

28
SURGICAL CARE Embolic AMI Unless bowel is gangrenous, an attempt of reperfusion is necessary Early surgical laparotomy with embolectomy. Embolectomy done via arteriotomy distal to occlusion, and a balloon- tipped Fogarty catheter is passed distally, inflated and clot extracted. Bypass may be required if thrombectomy unsuccessful.

29
BALLOON-TIPPED FOGARTY/EMBOLECTOMY CATHETER

30
SURGICAL CARE Thrombotic AMI Emergency surgical revascularization, unless gangrenous Antegrade Aortomesenteric bypass is the best technique. Simple thrombectomy has little/no benefit as most of these patients have significant atherosclerosis

31
SURGICAL CARE Mesenteric Venous Thrombisis Along with heparin anticoagulation, infarcted bowel must be resected Nonocclusive AMI Primary therapy which is papaverine infusion. Surgical exploration is limited to patients with peritoneal signs.

32
SUMMARY AMI results in mortaility rates >60% Specific risk factors: advanced age, atherosclerosis, CHF, arrhythmias, severe valvular disease, recent MI, intra-abdominal malignancy Early signs and symptoms are nonspecific, which delays the diagnosis. Mesenteric angiography is the gold standard diagnostic study for acute arterial ischemia. CT angiography is gold standard for mesenteric vein thrombosis Goal of treatment is to restore flow rapidly after initial management which includes aggressive hemodynamic monitoring and support, correction of metabolic acidosis, broad spectrum antibiotics, NGT for gastric decompression.

33
THANK YOU

34
REFERENCES Rosenblum JD, Boyle CM, Schwartz LB. The mesenteric circulation. Anatomy and physiology. Surg Clin North Am. Apr 1997;77(2):289-306 Herbert GS, Steele SR. Acute and chronic mesenteric ischemia. Surg Clin North Am. Oct 2007;87(5):1115-34, ix. American Gastroenterological Association Medical Position Statement: guidelines on intestinal ischemia. Gastroenterology 2000; 118:951 McKinsey JF, Gewertz BL. Acute mesenteric ischemia. Surg Clin North Am 1997; 77:307. Glenister KM, Corke CF. Infarcted intestine: a diagnostic void. ANZ J Surg 2004; 74:260
: Herbert GS, Steele SR. Acute and chronic mesenteric ischemia. Surg Clin North Am. Oct 2007;87(5): , ix. American Gastroenterological Association Medical Position Statement: guidelines on intestinal ischemia. Gastroenterology 2000; 118:951 McKinsey JF, Gewertz BL. Acute mesenteric ischemia. Surg Clin North Am 1997; 77:307. Glenister KM, Corke CF. Infarcted intestine: a diagnostic void. ANZ J Surg 2004; 74:260.")
Similar presentations






>")












