Download presentation
Presentation is loading. Please wait.

2
Objectives By the end lecture we will be able 1.To know what is normal liver and Spleen. 2. To know about various causes of hepatosplenomegaly. 3.How to do the clinical examination of the patients. 4. How will we do the workup of the patients.

3
Case-1 A previously well 25 year-old Man presented to the emergency department with 2 weeks history of jaundice which was associated with right upper quadrant pain, nausea and lethargy.

4
What is your diagnosis?

5
Case-2 A 35 year-old female presented with one week history of fever. On examination she was looking pale, had ting of jaundice with tip of palpable spleen.

6
What is your diagnosis?

7
Case-3 A 39-year-old female presented with a 3- months history of itching with recent change in color of her skin. On examination she had scratch marks on her body with hepato-splenomegaly?

8
What is your diagnosis?

9
4 A 51-year-old man presents to your outpatient clinic with H/O pain right Hypochondrium. Physical exam reveals liver palpable 5 cm below the right costal margin which was tender and smooth. There is ankle edema.

10
What is your diagnosis?

11
Case-5 A man of 45 consults his general practitioner (GP) with a 6-month history of reduced appetite with dragging pain in right hypochondrium. On Examination He has nine spider naive on his upper trunk with gynacomasia. There is pitting edema of his ankles. There is hepato-splenomegaly.

12
What is your diagnosis?

13
Case-6 A 34-year-lady is sent to your clinic with a chief complaint of fever with rigors and right upper quadrant pain for 2 weeks. Her liver is palpable by 7 cms and is tender.

14
What is your diagnosis?

15
Definition Hepatomegaly is swelling of the liver beyond its normal size. If both the liver and spleen are enlarged, it is called hepatosplenomegaly.

16
Liver span It is vertical distance between uppermost and lower most points of liver dullness-in Rt mid clavicular line- Normal-12-15 cm

17
The spleen is a functionally diverse organ with active roles in immunosurveillance and hematopoiesis. It lies within the left upper quadrant of the peritoneal cavity and abuts ribs 9-12, the stomach, the left kidney, the splenic flexure of the colon, and the tail of the pancreas. A normal spleen weighs 150 g and is approximately 11 cm in craniocaudal length Poulin et al defined splenomegaly as moderate if the largest dimension is 11-20 cm, and severe if the largest dimension is greater than 20 cm.

18
Questions What are the causes? How would you investigate? How would you manage?

19
The doctor will examine you and ask questions such as: Did you notice a fullness or lump in the abdomen? What other symptoms do you have? Is there any abdominal pain?abdominal pain Is there any yellowing of the skin (jaundice)?jaundice Is there any vomiting? Is there any unusual-colored or pale-colored stools?pale-colored stools Have you had any fever? What medications are you taking? How much alcohol do you drink?
 jaundice Is there any vomiting. Is there any unusual-colored or pale-colored stools pale-colored stools Have you had any fever. What medications are you taking. How much alcohol do you drink .")
21
patient has hepatosplenomegaly. (Determine which is the predominantly enlarged organ eg massive liver with small spleen or massively spleen with small liver; determine if there is any Cs liver findings such as pulsatile liver; if both are mildy enlarged then combine the causes) Mildly Enlarged(4cm</1-2FB) Acute malaria Chronic haemolytic – Thalassemia, AI, HS, ITP Myeloproliferative, Lymphoproliferative Infections Viral – CMV,EBV SBE, splenic abscesses, leptospirosis, Meliodosis, TB, Typhoid, Brucellosis(farmer) Infiltrative – Amylodosis, Sacoidosis Endocrine – Acromegaly, thyrotoxicosis Collagen vascular – SLE, Felty’s
 Mildly Enlarged(4cm</1-2FB) Acute malaria Chronic haemolytic – Thalassemia, AI, HS, ITP Myeloproliferative, Lymphoproliferative Infections Viral – CMV,EBV SBE, splenic abscesses, leptospirosis, Meliodosis, TB, Typhoid, Brucellosis(farmer) Infiltrative – Amylodosis, Sacoidosis Endocrine – Acromegaly, thyrotoxicosis Collagen vascular – SLE, Felty’s.")
22
Moderately Enlarged (4 to 8 cm/ 2-4 FB) Myeloproliferative Lymphoproliferative Haemotological – AI, ITP, Thalassemia and HS Chronic malaria Cirrhosis Massive Splenomegaly (>8 cm) CML Myelofibrosis PRV Chronic malaria Kala-azar (visceral leshmaniasis) Others(Gaucher’s, rapidly progressive lymphoma)
 Myeloproliferative Lymphoproliferative Haemotological – AI, ITP, Thalassemia and HS Chronic malaria Cirrhosis Massive Splenomegaly (>8 cm) CML Myelofibrosis PRV Chronic malaria Kala-azar (visceral leshmaniasis) Others(Gaucher’s, rapidly progressive lymphoma)")
23
Massive Liver HCC/Secondaries/myeloprolif RVF Alcoholic liver disease Mild-moderate Liver As above plus Infection Viruses – EBV, CMV, hepatitis A & B Bacteria – Weil’s disease (leptospirosis), meliodosis, abscesses, TB, brucellosis, syphilitic gumma
, meliodosis, abscesses, TB, brucellosis, syphilitic gumma")
24
Protozoal – hydatid cysts, amoebic abscess Malignancy – lymphoproliferative, myeloproliferative, primary, secondary, adenoma from OCP Infiltrative – sarcoid (erythema nodosum, lupus pernio), amyloid, fatty liver Endocrine – acromegaly, hyperthyroid Collagen Vascular disease Chronic hemolytic anaemia( AI, thalassemia, HS) Reidel’s lobe Possibility of minimal CLD signs with just hepatomegaly
, amyloid, fatty liver Endocrine – acromegaly, hyperthyroid Collagen Vascular disease Chronic hemolytic anaemia( AI, thalassemia, HS) Reidel’s lobe Possibility of minimal CLD signs with just hepatomegaly")
25
Tender Liver Liver abscess/infective (viral/bacterial/parasitic) HCC/Secondaries Right Heart Failure/Budd chiari Pulsatile Liver TR HCC AVM Hard/Irregular Liver Mitotic (primary/Secondary) Macronodular cirrhosis (post hepatitis B/C, Wilson’s and AAT) Amyloidosis/Hydatid cyst/granulomatous disease/gummatous disease/APCKD
 HCC/Secondaries Right Heart Failure/Budd chiari Pulsatile Liver TR HCC AVM Hard/Irregular Liver Mitotic (primary/Secondary) Macronodular cirrhosis (post hepatitis B/C, Wilson’s and AAT) Amyloidosis/Hydatid cyst/granulomatous disease/gummatous disease/APCKD ")
26
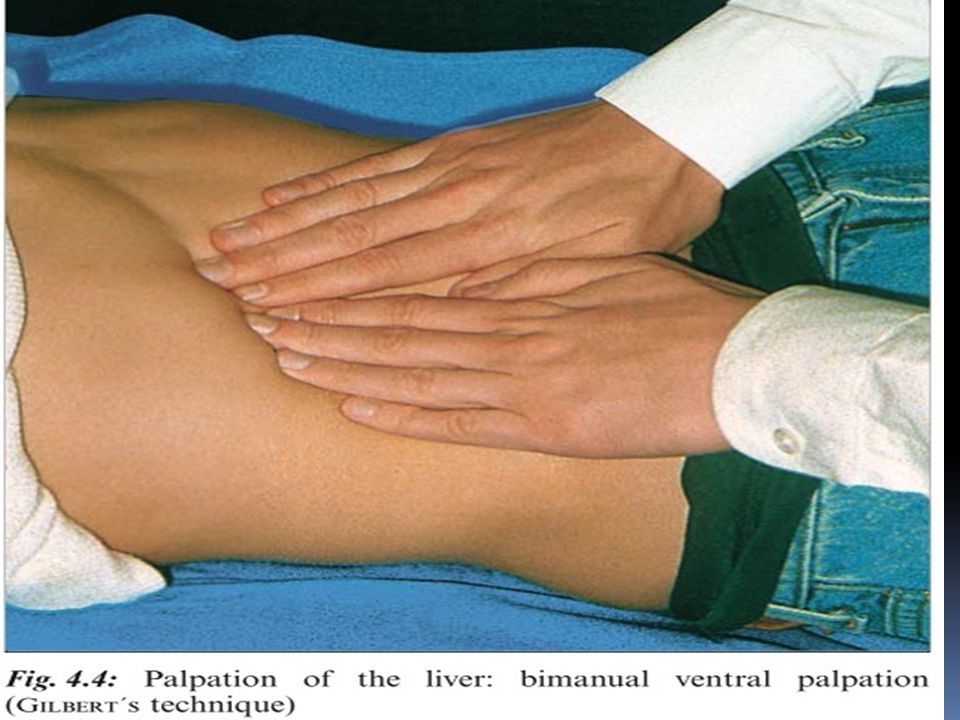
Palpation of the liver “One good feel of the liver is worth any two liver function tests” (F.M. Hanger, jr., 1971).
..")
27
Determining the liver size is considered to be the “simplest” and “cheapest” liver function test and, chronologically speaking, it is also the “first”

29
The liver is enlarged Size, edge, surface, consistency, tender, bruit or pulsatile The spleen is enlarged Size, edge, surface, consistency, tender Kidneys are not enlarged and no associated ascites Peripheral examination CLD stigmata, jaundice, bruises Hepatic encephalopathy Causes Pallor, cachexia, Cx LNs, PRV Toxic, rashes, tonsils Chronic ethanol ingestion CCF SBE, SLE, RA, Hemolytic anaemia

30
It would be a tremendous loss if palpation and percussion of the liver and spleen were inadequately learned, inappropriately performed and no longer mastered as a basic examination technique for interpretative purposes on account of ultrasound methods.

31
Workup of patients with Hepato- spenomegaly Initial lab tests: Complete blood count (CBC) with differential, platelet count, and peripheral blood smear in cases of splenomegaly. Urea,creatinine,electrolytes,glucose

32
Tests to determine the cause of the hepatospleno-megaly Liver function tests, including blood clotting tests Liver function tests Ultrasound of the liver (must be done to confirm the condition if the doctor thinks your liver feels enlarged during a physical exam) CT scan of the abdomen CT scan of the abdomen Other tests for suspected causes
 CT scan of the abdomen CT scan of the abdomen Other tests for suspected causes")
33
Investigations to consider (based on history and examination) amination) Liver blood tests (“LFT’s”) FBC Prothrombin time Viral serology (hepatitis A,B,C,D,E, CMV, EBV and HIV, Herpes simplex) Amoebic and hydatid serology. Consider toxoplasmosis and schistosomiasis. Autoantibodies including LKM antibodies Immunoglobulins (IgM/IgG) Haematinics (particularly Iron/ferritin) Copper, caeruloplasmin, α 1 Anti trypsin, α Feto-Protein Imaging: Abdominal USS ± Microbubble USS, CT, MRI etc ?admit via A+E (eg severe abdominal pain, jaundice, cachexia, haematemesis etc)
 Haematinics (particularly Iron/ferritin) Copper, caeruloplasmin, α 1 Anti trypsin, α Feto-Protein Imaging: Abdominal USS ± Microbubble USS, CT, MRI etc admit via A+E (eg severe abdominal pain, jaundice, cachexia, haematemesis etc).")
34
Common presentations/diagnoses NAFLD (mildly ↑ AST and ALP) RUQ pain and stones on USS ( ↑ AST and ALP, sometimes ↑ bilirubin) Possible haemangioma on USS (normal LFT’s) Cystic disease seen on USS (normal LFT’s) Autoimmune hepatitis ( ↑ ALT ± ALP and bilirubin) Jaundice (Haemolytic (pre hepatic), Congenital, Cholestatic (liver parenchymal and CBD obstruction: cholangiocarcinoma and carcinoma of the head of pancreas) Cirrhotic liver found on USS incidentally
 RUQ pain and stones on USS ( ↑ AST and ALP, sometimes ↑ bilirubin) Possible haemangioma on USS (normal LFT’s) Cystic disease seen on USS (normal LFT’s) Autoimmune hepatitis ( ↑ ALT ± ALP and bilirubin) Jaundice (Haemolytic (pre hepatic), Congenital, Cholestatic (liver parenchymal and CBD obstruction: cholangiocarcinoma and carcinoma of the head of pancreas) Cirrhotic liver found on USS incidentally")
35
Jaundice (a sign not a diagnosis) Haemolytic (pre hepatic) Congenital Cholestatic (liver parenchymal and CBD obstruction)
 Haemolytic (pre hepatic) Congenital Cholestatic (liver parenchymal and CBD obstruction)")
36
“Even though you read and learn so much, your learning does not mean that you know; let your eyes be your professors.” (Theophrastus Bombastus von Hohenheim, known as PARACELSUS)
")
37
THANK YOU THANK YOU

Similar presentations



MRCP(LONDON) ASSOCIATE PROFESSOR MEDICINE.>")
,MRCP(LONDON).>")









>")






