Download presentation
Presentation is loading. Please wait.

1
Traditional One-Lung Ventilation & ALI; Have we been killing our Patients? Philip M. Hartigan, MD Brigham & Women’s Hospital Harvard Medical School

2
Case Report: 54 y/o male Smoking History COPD Persistent cough

3
CXR - Large RUL mass Cytology = NSCCA Metastatic w/u Negative Scheduled for a Right Pneumonectomy Case Report:

4
CASE REPORT: General Anesthetic: Thoracic Epidural A-Line TIVA L-DLT VT =10 ml/kg PEEP = O

5
CASE REPORT: Hospital Course – POD # 2: Dyspnea Hypoxemia Pulmonary Edema

7
CASE REPORT: Hospital Course (cont.): Respiratory Failure Reintubation PCWP < 16 cmH 2 O Diuretics Fluid Restriction ARDS MSOF Death
: Respiratory Failure Reintubation PCWP < 16 cmH 2 O Diuretics Fluid Restriction ARDS MSOF Death")
8
What Just Happened ?

9
“ Traditional” OLV“Protective” OLV VT = 10 ml/kgVT = 6 ml/kg PEEP = 0PEEP = 5 cmH 2 O

10
Impact:Incidence: 2 - 9% Mortality: 35 – 72% “ALI/ARDS is emerging as the most prominent cause of perioperative mortality following pulmonary resection as other complications have become better controlled” Peter Slinger 2006

11
Known Causes of ALI / ARDS: Infection Aspiration BPF Cardiac Failure Pulmonary Embolic events TRALI Other (pancreatitis, trauma, CPB…)
")
12
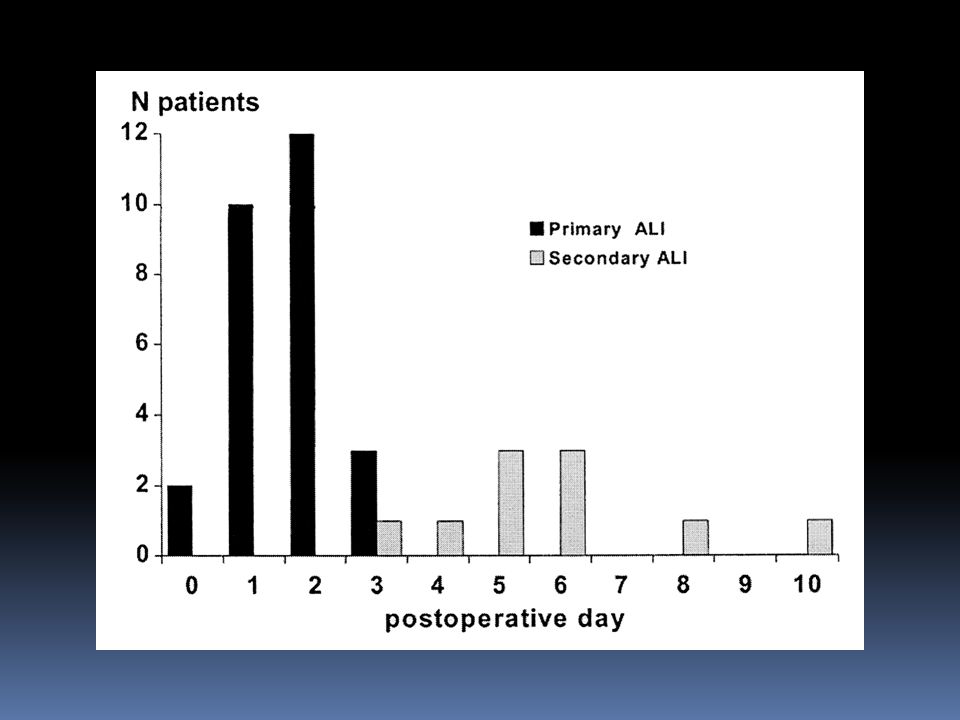
Post-Pneumonectomy Pulmonary Edema ALI following Pulmonary Resection Primary ALI following Thoracic Surgery Idiopathic ALI following Pulm Resection Nomenclature

13
Hypothesis: “Traditional OLV Causes ALI “ Extrapolated Evidence Retrospective Studies Animal Studies Clinical Studies

14
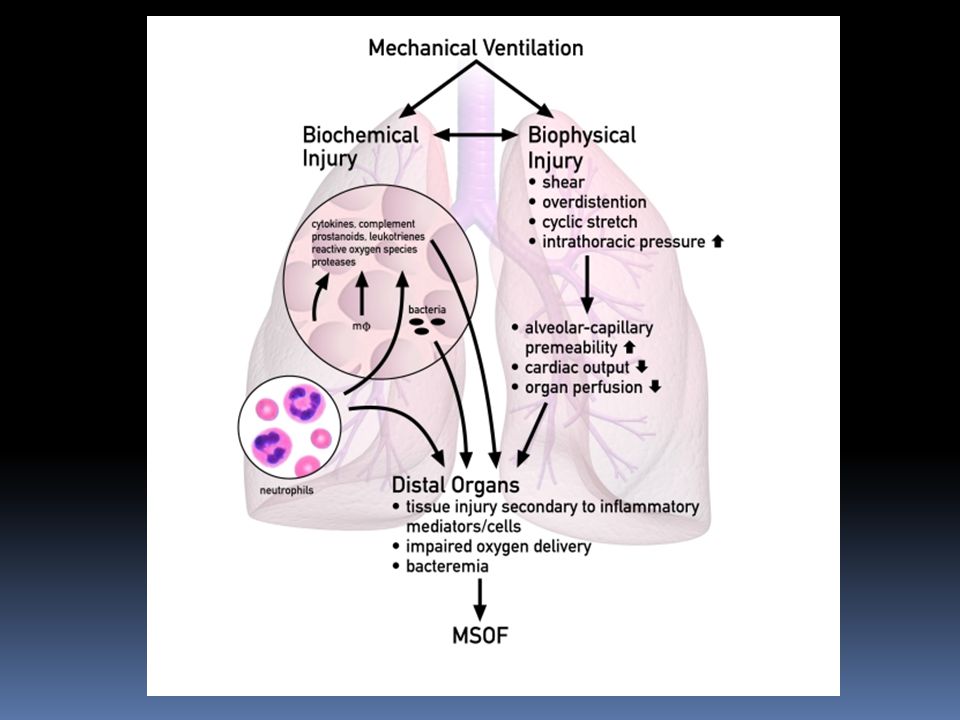
Extrapolated Evidence: ARDS Literature: Reduced ARDS Mortality with Protective Ventilation VILI Literature: Volutrauma Atelectrauma Inflammatory Response Alveolar Systemic

16
“The finding of small changes in cytokine concentrations is in no way indicative of a causal link with outcome” Dreyfuss Didier, 2003

17
Hypothesis: “Traditional OLV Causes ALI “ Extrapolated Evidence – (Weak) Retrospective Studies Animal Studies Clinical Studies
 Retrospective Studies Animal Studies Clinical Studies")
18
Retrospective Studies; Factors Associated w/ ALI: High Perioperative Fluid Balance Extent of Surgery Side of Surgery (R > L) Duration of Surgery Alcoholism / Chemotherapy Increased Vent Pressures/Volumes
 Duration of Surgery Alcoholism / Chemotherapy Increased Vent Pressures/Volumes")
19
Retrospective Studies: Van der Werff ‘97 190 Pts PIPs > 40 assoc. w/ Pulm Edema Licker ‘03879 Pts Ventilatory Hyperpressure Index Fernandez -170 Pts VT assoc with -Perez ‘06Resp Failure 8.3 vs 6.7 ml/kg

21
Risk Factors for Primary ALI Licker, et al: Anesth Analg 2003;97:1558 Pneumonectomy Excessive Fluid Alcoholism Ventilatory Hyperpressure Index

22
Risk Factors for Primary ALI Licker, et al: Anesth Analg 2003;97:1558 Pneumonectomy Excessive Fluid Alcoholism Ventilatory Hyperpressure Index (P-Plateau > 10 cmH 2 0 x Duration OLV)
")
23
Hypothesis: “Traditional OLV Causes ALI “ Extrapolated Evidence - (weak) Retrospective Studies – (weak) Animal Studies Clinical Studies
 Retrospective Studies – (weak) Animal Studies Clinical Studies")
24
Animal Studies: De Abreu, et al. Anesth Analg 2003 Control – 2LV @ 8 ml PEEP = 2 Protect - OLV @ 4 ml PEEP = 2 Tradit’l – OLV @ 8 ml PEEP = 0

25
OLV in the Rabbit Lung Model De Abreu, et al. Anesth Analg 2003; 96:220 PIP MPAP TXB2 WG 2-LV (CTRL)Protect OLVTraditional OLV
Protect OLVTraditional OLV.")
26
Hypothesis: “Traditional OLV Causes ALI “ Extrapolated Evidence – (weak) Retrospective Studies – (weak) Animal Studies – (suggestive) Clinical Studies
 Retrospective Studies – (weak) Animal Studies – (suggestive) Clinical Studies")
27
Clinical Studies: Schilling, et al 2005 Schilling, et al 2007 Schilling, et al 2011 Traditional vs Protective OLV: Proinflammatory Cytokines Inhalational Agents are protective

28
Schilling T, et al. Anesth Analg 2005;101:957 Protective OLV and Inflammatory Mediators Design: 32 Pts for thoracotomy OLV @ 5 vs 10 ml/kg PEEP = 0 BAL at 3 time points Findings: Traditional OLV was associated with: Proinflammatory cytokines Antiinflammatory cytokines I

29
IL-8TNF-a sICAM IL-10 VT = 10 ml/kgVT = 5 ml/kg Schilling ‘05

30
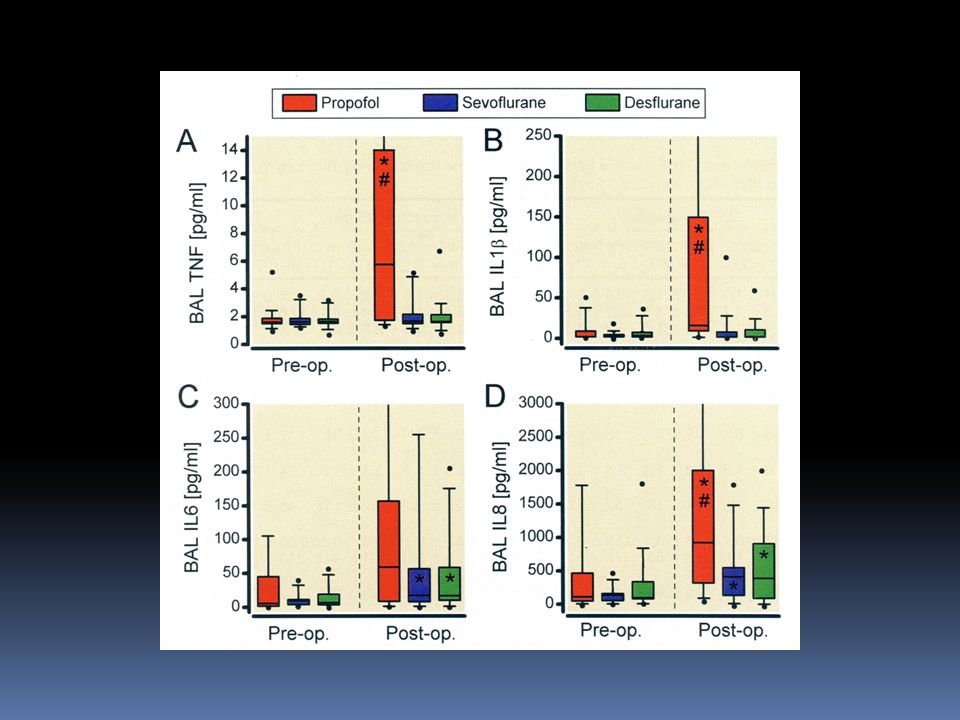
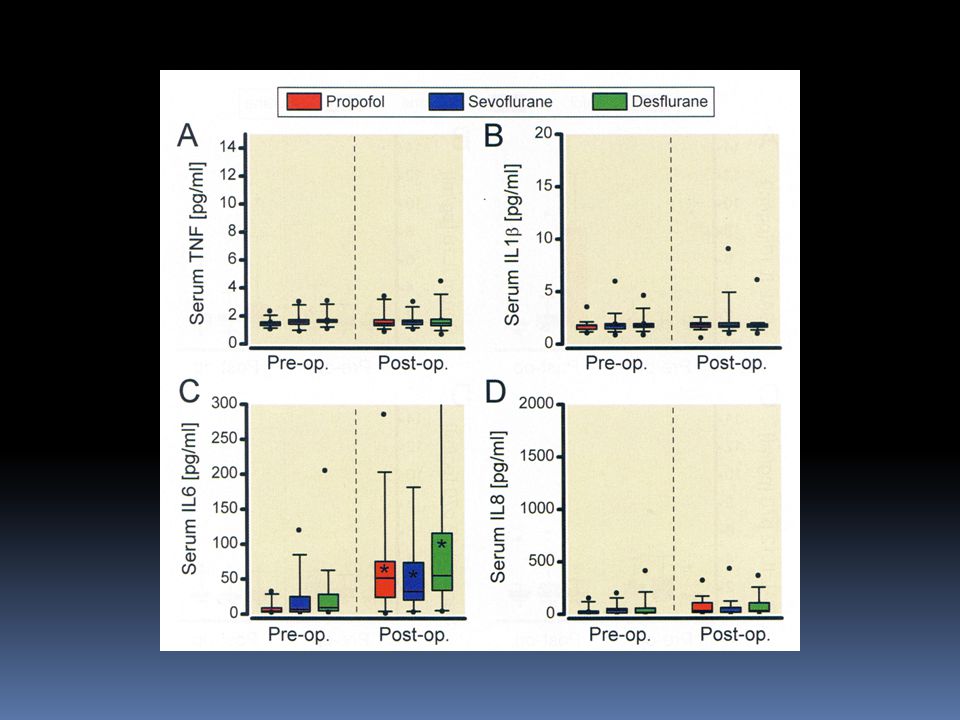
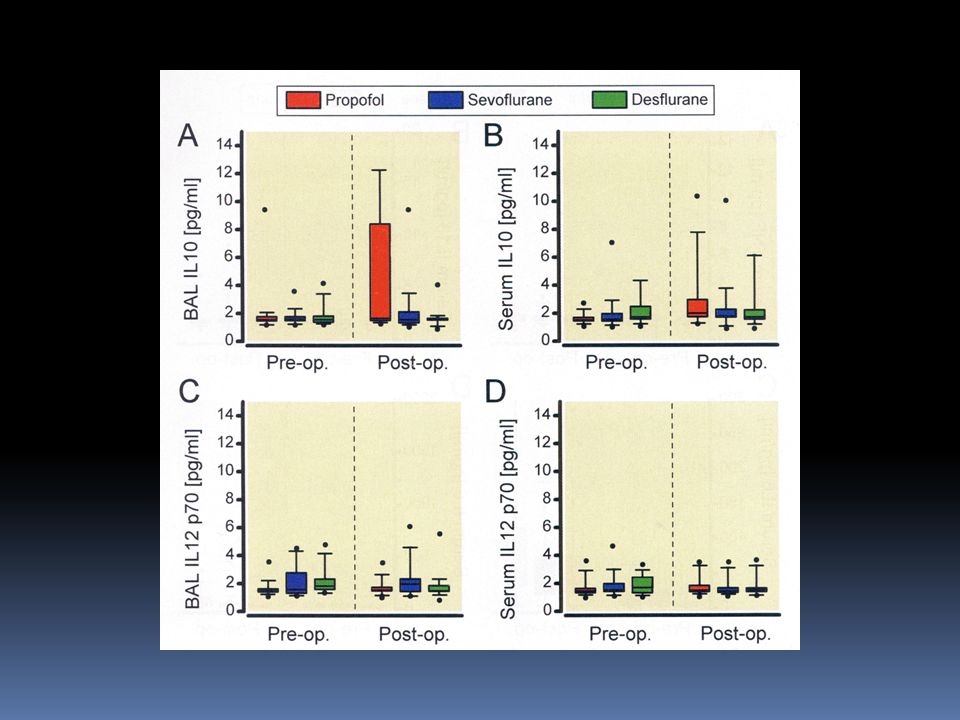
Schilling T, et al. Anesthesiology 2011;115:65 Effect of Volatile Anesthetics on Systemic and Alveolar Inflammatory Response Design: 63 Pts for thoracotomy 21 – Propofol (4mg/kg/hr) 21 – Desflurane (1 MAC) 21 – Sevoflurane (1 MAC) OLV @ 7 ml/kg PEEP = 5 BAL before & after OLV Findings: Desfl & Sevo attenuate proinflammatory changes even with protective OLV compared to Propofol. III
 21 – Desflurane (1 MAC) 21 – Sevoflurane (1 MAC) 7 ml/kg PEEP = 5 BAL before & after OLV Findings: Desfl & Sevo attenuate proinflammatory changes even with protective OLV compared to Propofol. III.")
32
Hypothesis: “Traditional OLV Causes ALI “ Extrapolated Evidence – (weak) Retrospective Studies – (weak) Animal Studies – (suggestive) Clinical Studies – (suggestive)
 Retrospective Studies – (weak) Animal Studies – (suggestive) Clinical Studies – (suggestive)")
33
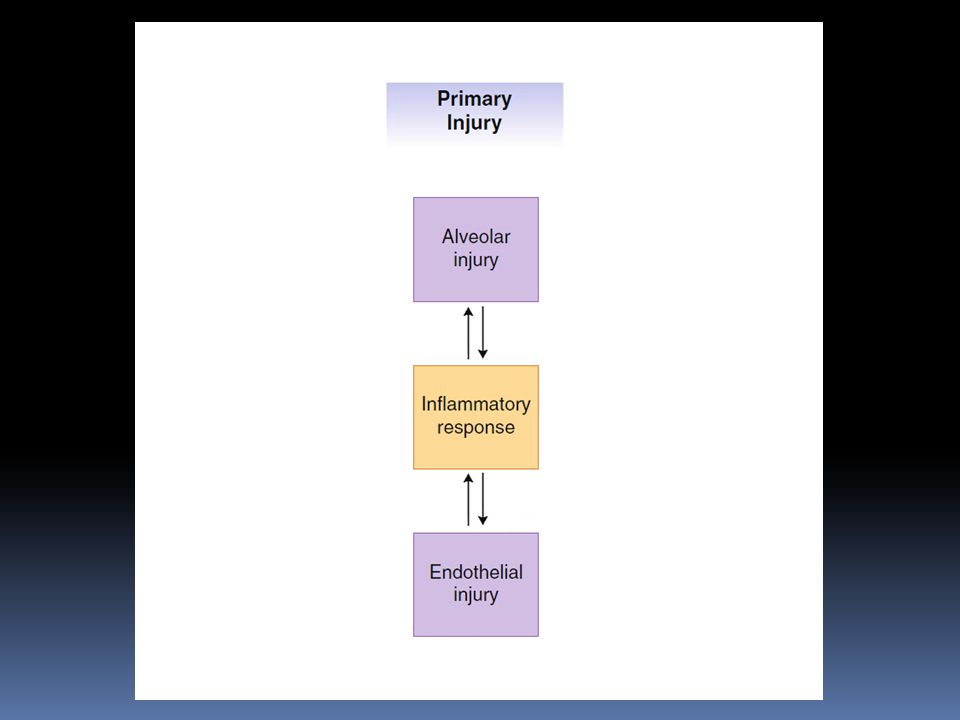
Death OLV Inflammatory Response ALI / ARDS

34
Death Unbalance Drainage Chemo / XRT Extent of Surgery Duration of Surg Alcoholism Genetic Unrecognized: Infection Aspiration Emboli TRALI Cardiac Pneumonectomy Impaired Lymphatics Excessive Fluids OLV Inflammatory Response ALI / ARDS

35
Death Unbalance Drainage Chemo / XRT Extent of Surgery Duration of Surg Alcoholism Genetic Unrecognized: Infection Aspiration Emboli TRALI Cardiac Pneumonectomy Impaired Lymphatics Excessive Fluids Low VT PEEP Sevoflurane Desflurane Low FiO2 OLV Inflammatory Response ALI / ARDS

36
CO 2 Injury The Balancing Act of OLV O2O2

38
Schilling T, et al. Br J Anaesth 2007;99:368 OLV & Inflammatory Mediators: Propofol vs Desflurane Design: 30 Pts for thoracotomy 15 – Propofol (4mg/kg/hr) 15 – Desflurane (1 MAC) OLV @ 10 ml/kg PEEP = 0 BAL at 3 time points Findings: Desflurane attenuates the proinflammatory changes of non-protective OLV II
 15 – Desflurane (1 MAC) 10 ml/kg PEEP = 0 BAL at 3 time points Findings: Desflurane attenuates the proinflammatory changes of non-protective OLV II.")
39
TNF-a IL-8 IL-10 sICAM-1 PropofolDesflurane Schilling ‘07

42
Postulated Causes VILI from “Traditional” OLV Oxygen Toxicity Hyperperfusion Stress Injury Inflammatory Response to Surgery Postoperative Hyperexpansion Unrecognized, Known Etiologies

43
Known Causes of ALI / ARDS: Infection Aspiration BPF Cardiac Failure Pulmonary Embolic events TRALI VILI Other (pancreatitis, trauma, CPB…)
")
48
Factors Associated with ALI High Perioperative Fluid Balance Extent of Surgery Side of Surgery (R > L) Duration of Surgery Alcoholism / Chemotherapy
 Duration of Surgery Alcoholism / Chemotherapy")
50
Idiopathic ALI following Pulm Resection 2-9% following pneumonectomy 35 – 50% Mortality Clinical / Histology resembles ALI/ARDS Low PCWP, high alveolar protein Diagnosis of Exclusion

51
Acute Lung Injury Bilateral Pulmonary Infiltrates PCWP < 18 mmHg PaO 2 /FiO 2 < 300 mmHg ARDS PaO 2 /FiO 2 < 200 mmHg Definitions: ALI & ARDS

52
Hypothesis: “Traditional OLV Causes ALI “ Extrapolated Evidence Retrospective Studies Animal Studies Clinical Studies

53
OLV Mech Stress Injury ALI ARDS DEATH Inflamm Mediators

55
Perspective Does Traditional OLV Cause ALI ? Potential contributing factor Theoretical risk Not currently strongly supported by evidence

56
Recommendations: Initial VT = 5-6 ml/kg PEEP = 5

Similar presentations















>")








 Dr. Meg-angela Christi Amores.>")
