Download presentation
Presentation is loading. Please wait.

1
Nephrotic Syndrome Ali Derakhshan MD Shiraz University of Medical Sciences, Shiraz-Iran

3
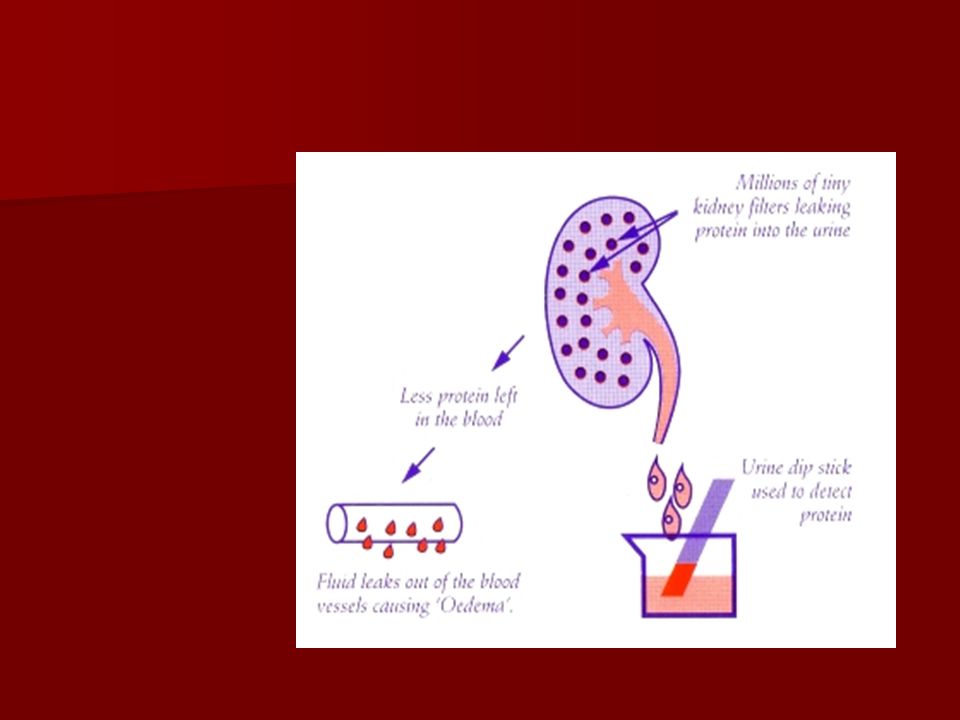
DEF: Heavy proteinuria, Hypoalbuminemia, edema and Hyperlipidemia

5
Classification Etiologic: Primary* (Idiopathic) and secondary Etiologic: Primary* (Idiopathic) and secondary Clinical: Steroid responsive &resistant Clinical: Steroid responsive &resistant Pathologic:{MCNS, FSGS,DMESPGN} → idiopathic Pathologic:{MCNS, FSGS,DMESPGN} → idiopathic : MPGN,MGN, CGN→ non-idiopathic : MPGN,MGN, CGN→ non-idiopathic Congenital N/S Congenital N/S *The most common type in children
 and secondary Etiologic: Primary* (Idiopathic) and secondary Clinical: Steroid responsive &resistant Clinical: Steroid responsive &resistant Pathologic:{MCNS, FSGS,DMESPGN} → idiopathic Pathologic:{MCNS, FSGS,DMESPGN} → idiopathic : MPGN,MGN, CGN→ non-idiopathic : MPGN,MGN, CGN→ non-idiopathic Congenital N/S Congenital N/S *The most common type in children")
6
Etiologies of Nephrotic Syndrome Idiopathic(primary) : MCNS, FSGS, MesPGN, **MPGN, MN, IgM nephropathy,C1q nephropathy Secondary Genetic:AR(NPHS2 mutations), AD Infections: Hepatitis B&C, HIV, Malaria, Schistosomaiasis Metabolic Diseases: Fabry’s dis.,Glutaric acidemia, GSD, Mitochondrial cytopathies Hematologic and oncologic diseases: Leukemia,Hodgkin’s(MCNS) lymphoma, sickle cell disease, colon carcinoma,bronchgenic carc. Drugs: NSAIDS, gold, penicillamine, Ampicillin, ACEIs, Pamidronate, interferon, Mercury, Heroin, Lithium Allergy: pollen, fungi, cow's milk, bee sting, house dust Others: Obesity (FSGS), oligomeganephronia, pregnancy
, oligomeganephronia, pregnancy.")
7
Genes and NS Finnish / DMS NPHS1nephrinAR FSGSNPHS2podocinAR FSGSACTN4alpha actinin 4AD FSGSTRPC6 transient receptor potential cation channel homolog of 6 AD FSGSCD2AP CD2 associated protein AR/AD DMSPLCE1 phospholipase C epsilon 1 AR Denys Drash (DMS) / Frasier (FSGS) WT1 wilms tumor suppressor protein AD
 / Frasier (FSGS) WT1 wilms tumor suppressor protein AD")
8
Genes and NS Schimke immuno-osseous dysplasia SMARCAL1 (AR) Pierson syndrome LAMB2 (AR) AMRF syndrome SCARB2/LIMP2 (AR) Nail patella syndrome LMX1B (AD) Galloway Mowat syndrome (AR) Mitochondrial cytopathies COQ2 deficiency COQ2 Leigh syndrome PDSS2 MELAS Steroid sensitive NS - linkage chromosome 2p12- 13.2 in 11 German families with AR NS Familial forms of nephrotic syndrome. Carid et al. 2010 Ped Nephrol 25:241-252

9
Epidemiology 8 new cases/yr in children<16 yr/100000 8 new cases/yr in children<16 yr/100000 Peak incidence of MCNS &FSGS(80%)<6yrs at onset Peak incidence of MCNS &FSGS(80%)<6yrs at onset Median age MCNS 2.5 yr, FSGS 6 yr Median age MCNS 2.5 yr, FSGS 6 yr Younger age M/F,3/2 then M=F Younger age M/F,3/2 then M=F 3.4% of MCNS familial 3.4% of MCNS familial
<6yrs at onset Peak incidence of MCNS &FSGS(80%)<6yrs at onset Median age MCNS 2.5 yr, FSGS 6 yr Median age MCNS 2.5 yr, FSGS 6 yr Younger age M/F,3/2 then M=F Younger age M/F,3/2 then M=F 3.4% of MCNS familial 3.4% of MCNS familial")
10
Associated Disorders in N/S Atopy 30-60% Atopy 30-60% IgE>1500IU/ml IgE>1500IU/ml Malignancy (Hodgk., Thymoma, M gravis, IDMM) Malignancy (Hodgk., Thymoma, M gravis, IDMM) MHC :HLA-B8,B12 MHC :HLA-B8,B12
 Malignancy (Hodgk., Thymoma, M gravis, IDMM) MHC :HLA-B8,B12 MHC :HLA-B8,B12")
11
DEFINITION of PROTEINURIA >4mg/m ² /hr,in adults>150mg/24hr >4mg/m ² /hr,in adults>150mg/24hr Measurement of urine protein Measurement of urine protein Qualitative: Qualitative: False (+)or ↑+ with high SG, Alk.PH,detergent, ↑No of G-bacteria False (+)or ↑+ with high SG, Alk.PH,detergent, ↑No of G-bacteria Semiquant.: Pr/Cr in a urine sample, 0.2significant Semiquant.: Pr/Cr in a urine sample, 0.2significant >1?nephrotic,>2-3definite nephrotic (pr/cr)×0.65=gm/m²/day >1?nephrotic,>2-3definite nephrotic (pr/cr)×0.65=gm/m²/day Quantitative: 40mg/m²/hr or>2gm/m²/day or Quantitative: 40mg/m²/hr or>2gm/m²/day or 50mg/kg/day is defined as nephrotic range. 50mg/kg/day is defined as nephrotic range. 1+ 30-99 mg% 2+ 100-299 mg% 3+300-999mg% 4+ >1000mg% >1000mg% ↑↑

12
Pathophysiology Of edema in N/S ↓ Alb. → ↓ oncotic pressure→edema ↓ Alb. → ↓ oncotic pressure→edema ↓ Alb. → ↑ADH→water retention→edema ↓ Alb. → ↑ADH→water retention→edema ↑Aldost.→salt and water retention ↑Aldost.→salt and water retention Vascular permeability factor ---------→edema Vascular permeability factor ---------→edema

13
count.... Clinical and Paraclinical Features of N/S Sudden onset of periorbital edema Sudden onset of periorbital edema Anasarca,ascites Anasarca,ascites Pleural effusion,scrotal edema Pleural effusion,scrotal edema Abd.pain due to edema,peritonitis,thrombosis, pancreatitis Abd.pain due to edema,peritonitis,thrombosis, pancreatitis Diagnosis:Nephrotic range proteinuria &……………… Diagnosis:Nephrotic range proteinuria &……………… U/A: Fat bodies,Hyaline cast,micro.Hematuria5-15%of MCNS,67%of FSGS, Gross Hematuria none in MCNS but 3%of FSGS also glucosuria and Aminoaciduria+ in FSGS U/A: Fat bodies,Hyaline cast,micro.Hematuria5-15%of MCNS,67%of FSGS, Gross Hematuria none in MCNS but 3%of FSGS also glucosuria and Aminoaciduria+ in FSGS Urine Na<1-5mmol/L Urine Na<1-5mmol/L Total protein<5gm%in80% &<4gm%in 40%(Alb.<2gm% Total protein<5gm%in80% &<4gm%in 40%(Alb.<2gm%

14
Clinical and Para-clinical Features of N/S ↓ Alb., ↑ α2-globulin, ↑ β-globulin, ↓ γglobulin, ↓ Alb., ↑ α2-globulin, ↑ β-globulin, ↓ γglobulin, ↓ IgG, ↓ IgA, ↑IgM, ↑IgE, ↑Fibrinogen, ↓ Anti-thrombin3 ↓ IgG, ↓ IgA, ↑IgM, ↑IgE, ↑Fibrinogen, ↓ Anti-thrombin3 ↑Lipid due to↑Hepatic synth.(lipoproteins,CHO,TG) ↑Lipid due to↑Hepatic synth.(lipoproteins,CHO,TG) and ↓ catabolism ↓ Lipoprotein Lipase activity and ↓ catabolism ↓ Lipoprotein Lipase activity ↑LDL, ↓ HDL, ↑urine loss of HDL ↑LDL, ↓ HDL, ↑urine loss of HDL Hypocalcemia Hypocalcemia BUN,Cr,NL or ↑ BUN,Cr,NL or ↑ Hb,HCT NL or↑ Hb,HCT NL or↑ ↑Platelet ↑Platelet Diagnostic Criteria: Edema, Nephrotic range proteinuria, ↓ Alb<2.5gm/dl, ↑TG&CHO Diagnostic Criteria: Edema, Nephrotic range proteinuria, ↓ Alb<2.5gm/dl, ↑TG&CHO Selective proteinuria Selective proteinuria
 ↑Lipid due to↑Hepatic synth.(lipoproteins,CHO,TG) and ↓ catabolism ↓ Lipoprotein Lipase activity and ↓ catabolism ↓ Lipoprotein Lipase activity ↑LDL, ↓ HDL, ↑urine loss of HDL ↑LDL, ↓ HDL, ↑urine loss of HDL Hypocalcemia Hypocalcemia BUN,Cr,NL or ↑ BUN,Cr,NL or ↑ Hb,HCT NL or↑ Hb,HCT NL or↑ ↑Platelet ↑Platelet Diagnostic Criteria: Edema, Nephrotic range proteinuria, ↓ Alb<2.5gm/dl, ↑TG&CHO Diagnostic Criteria: Edema, Nephrotic range proteinuria, ↓ Alb<2.5gm/dl, ↑TG&CHO Selective proteinuria Selective proteinuria")
15
count.. Treatment of Nephrotic Syndrome Diet :salt restriction for edema,protein 130-140%of RDA Diet :salt restriction for edema,protein 130-140%of RDA Fat restriction Fat restriction Diuretic Diuretic TB Test, U/C, search for site of infection TB Test, U/C, search for site of infection Antibiotic & immunization Antibiotic & immunization Albumin infusion if abd. pain, oliguria and pre-renal azotemia.... Albumin infusion if abd. pain, oliguria and pre-renal azotemia.... For children 1-12 yrs and no( Gross Hematuria,severe HTN and renal failure) start prednisolone60mg/m ² /day (divided tid)×6wks then40mg/m ² QOD single dose *6wks and taper in 4wks For children 1-12 yrs and no( Gross Hematuria,severe HTN and renal failure) start prednisolone60mg/m ² /day (divided tid)×6wks then40mg/m ² QOD single dose *6wks and taper in 4wks ≈90%may respond to steroid (usually within 2wks) ≈90%may respond to steroid (usually within 2wks) Steroid – Resistant :ISKDC*: If no response to prednisolone 2mg/kg *4wks Steroid – Resistant :ISKDC*: If no response to prednisolone 2mg/kg *4wks French society of pediatric nephrology*:no response to 4wks steroid+3pulses of Methyl-Prednisolone French society of pediatric nephrology*:no response to 4wks steroid+3pulses of Methyl-Prednisolone Nelson text:If no response to steroid within 8 wks Nelson text:If no response to steroid within 8 wks ISKDC*:international study of kidney disease in children ISKDC*:international study of kidney disease in children
 start prednisolone60mg/m ² /day (divided tid)×6wks then40mg/m ² QOD single dose *6wks and taper in 4wks For children 1-12 yrs and no( Gross Hematuria,severe HTN and renal failure) start prednisolone60mg/m ² /day (divided tid)×6wks then40mg/m ² QOD single dose *6wks and taper in 4wks ≈90%may respond to steroid (usually within 2wks) ≈90%may respond to steroid (usually within 2wks) Steroid – Resistant :ISKDC*: If no response to prednisolone 2mg/kg *4wks Steroid – Resistant :ISKDC*: If no response to prednisolone 2mg/kg *4wks French society of pediatric nephrology*:no response to 4wks steroid+3pulses of Methyl-Prednisolone French society of pediatric nephrology*:no response to 4wks steroid+3pulses of Methyl-Prednisolone Nelson text:If no response to steroid within 8 wks Nelson text:If no response to steroid within 8 wks ISKDC*:international study of kidney disease in children ISKDC*:international study of kidney disease in children.")
16
Induction Use of Albumin:- Albumin (20 % salt poor)+ Lasix Albumin (20 % salt poor)+ Lasix 1-Severe edema 1-Severe edema 2-Ascites 2-Ascites 3-Pleural effusion 3-Pleural effusion 4-Genital edema 4-Genital edema 5-Low serum albumin 5-Low serum albumin 6- prerenal azotemia 6- prerenal azotemia
+ Lasix Albumin (20 % salt poor)+ Lasix 1-Severe edema 1-Severe edema 2-Ascites 2-Ascites 3-Pleural effusion 3-Pleural effusion 4-Genital edema 4-Genital edema 5-Low serum albumin 5-Low serum albumin 6- prerenal azotemia 6- prerenal azotemia")
17
Treatment of Nephrotic Syndrome 60-70%of steroid responders may relapse 60-70%of steroid responders may relapse Steroid dependent: relapse upon tapering or within 2-4 wks of D/C prednisolone Steroid dependent: relapse upon tapering or within 2-4 wks of D/C prednisolone Freq.relapsers:*2 Relapse in 6months or Freq.relapsers:*2 Relapse in 6months or *4 Relapse in 1 yr (0.1-0.5mg/kg pred. Q.O.D FOR 1yr) *4 Relapse in 1 yr (0.1-0.5mg/kg pred. Q.O.D FOR 1yr) Rx of relapse:daily steroid till protein free*3-4d then Qod Rx of relapse:daily steroid till protein free*3-4d then Qod Relapse on <0.5mg/kg pred.Q.O.D,pred *1-1.5yr Relapse on <0.5mg/kg pred.Q.O.D,pred *1-1.5yr Relapse on >0.5mg/kg Q.O.D or steroid side effects: levamisole or cyclophosphamide(CTX) 2mg/kg/day*3months(total of 180mg/kg) or MMF Relapse on >0.5mg/kg Q.O.D or steroid side effects: levamisole or cyclophosphamide(CTX) 2mg/kg/day*3months(total of 180mg/kg) or MMF After CTX if relapse on prednisolone >0.5mg/kgQ.O.D kidney biopsy and consider Cyclosporin5mg/kg/day* 1yr After CTX if relapse on prednisolone >0.5mg/kgQ.O.D kidney biopsy and consider Cyclosporin5mg/kg/day* 1yr Stress dose of steroid Stress dose of steroid
 *4 Relapse in 1 yr ( mg/kg pred. Q.O.D FOR 1yr) Rx of relapse:daily steroid till protein free*3-4d then Qod Rx of relapse:daily steroid till protein free*3-4d then Qod Relapse on <0.5mg/kg pred.Q.O.D,pred *1-1.5yr Relapse on <0.5mg/kg pred.Q.O.D,pred *1-1.5yr Relapse on >0.5mg/kg Q.O.D or steroid side effects: levamisole or cyclophosphamide(CTX) 2mg/kg/day*3months(total of 180mg/kg) or MMF Relapse on >0.5mg/kg Q.O.D or steroid side effects: levamisole or cyclophosphamide(CTX) 2mg/kg/day*3months(total of 180mg/kg) or MMF After CTX if relapse on prednisolone >0.5mg/kgQ.O.D kidney biopsy and consider Cyclosporin5mg/kg/day* 1yr After CTX if relapse on prednisolone >0.5mg/kgQ.O.D kidney biopsy and consider Cyclosporin5mg/kg/day* 1yr Stress dose of steroid Stress dose of steroid.")
18
Steroid Toxicity Cushingoid habitus Cushingoid habitus Obesity Obesity cataract cataract Striae Striae Hirsutism Hirsutism Acne Acne Growth failure Growth failure Avascular necrosis Avascular necrosis Osteoporosis Osteoporosis

19
Indication of kidney Biopsy in N/S Before treatment : age <6mo,macroscopic Hematuria, (mic.hematuria +persistent HTN), ↓ C3,renal failure Before treatment : age <6mo,macroscopic Hematuria, (mic.hematuria +persistent HTN), ↓ C3,renal failure ±Biopsy:Age6-12mo,>12yr,persistant HTN orMic.Hematuria ±Biopsy:Age6-12mo,>12yr,persistant HTN orMic.Hematuria After Treatment: Steroid Resistant N/S and frequent relapsers before 3 rd line drug After Treatment: Steroid Resistant N/S and frequent relapsers before 3 rd line drug Secondary nephrotic synd. Secondary nephrotic synd.

20
Pathology and clinico-pathlogic correlations MCNS: 85%of INS 95%steroid responders MCNS: 85%of INS 95%steroid responders MesPGN:5%of INS 50- 60%st.responders MesPGN:5%of INS 50- 60%st.responders FSGS:10%of INS<20%respnds to all med. FSGS:10%of INS<20%respnds to all med.

21
Complications of N/S Infections: peritonitis, sepsis, pneumonia,cellulitis, meningitis due to ↓ IgG, ↑urinary loss of factor B, impaired Tcell function, ↓ splenic function,Edema and ascites, Infections: peritonitis, sepsis, pneumonia,cellulitis, meningitis due to ↓ IgG, ↑urinary loss of factor B, impaired Tcell function, ↓ splenic function,Edema and ascites, Risk of viral infection after steroid therapy (chiken pox) Risk of viral infection after steroid therapy (chiken pox) Peritonitis:>250 WBC in perit.fluid and >50%poly Peritonitis:>250 WBC in perit.fluid and >50%poly ARF: Pre-Renal, RVT, ATN ARF: Pre-Renal, RVT, ATN CRF:3% of steroid responders and >50%of resistant CRF:3% of steroid responders and >50%of resistant Growth retardation, cataract, hirsutism, striae Growth retardation, cataract, hirsutism, striae Thrombosis 3%:Hypercog.state due to ↓ Alb., immobilization, ↑platelet agg., ↑fibrinog.,↑factor 5,7,10-13, ↓ factor11,12,Anti-thrombin3 and heparin co-factors (C &S) Thrombosis 3%:Hypercog.state due to ↓ Alb., immobilization, ↑platelet agg., ↑fibrinog.,↑factor 5,7,10-13, ↓ factor11,12,Anti-thrombin3 and heparin co-factors (C &S) Alb. 6gm/Lit and anti-thrombin3 6gm/Lit and anti-thrombin3 < 70%of Nl start warfarin

22
SUMMARY Longer courses of Prednisolone associated with reduced subsequent relapses Cyclophosphamide, Levamisole, Cyclosporine – all effective steroid sparing agents, effect not sustained in later two. New drugs : MMF, TAC, Rituximab – further evidence awaited In SDNS, daily steroids for 7 days may prevent post-viral relapses Genetic forms are usually resistant to therapy Supportive treatment with aldosterone inhbition, control of blood pressure and hyperlipidemia improves prognosis

Similar presentations

 Acute GN Definition (Hricik et al, 1998) Syndrome characterized by the abrupt onset of macroscopic hematuria; oliguria; acute renal failure; manifested.>")
 FSGS Secondary FSGS 1. Familial/genetic.>")



>")
>")
 Definition NS is an accumulation of symptoms and signs and is characterized by proteinuria, hypoproteinemia, edema, and hyperlipidemia.>")

 saying that her legs have been swollen for a month. On examination you find that she has.>")






 Membranous glomerulonephritis Focal segmental glomerulosclerosis.>")


 Characteristics : Proteinuria ( urine protein loss > 2 gm/day ) Hypo-proteinemia ( serum albumin < 2.5 gm/dL ) Edema Hyperlipidemia.>")