Download presentation
Presentation is loading. Please wait.

1
Hemodynamic Monitoring for the Respiratory Therapist
Jane Reynolds, MS, RN, RRT

2
Definition of terms Preload – amount of blood in the ventricle before contraction – End diastolic volume EDV determines the amount of ‘stretch’ that is placed on the myocardial muscle That ‘stretch’ determines the strength of the next contraction The strength of the contraction determines how much blood is pumped out of the ventricle during the next systole ‘stroke volume’ The stroke volume determines the blood pressure and perfusing pressures

3
Definition of terms Afterload - resistance to blood flow from the ventricle; work that must be done to pump blood from the ventricle to the circulation Resistance determined by size of valve opening, blood viscosity and blood pressure in pulmonary or systemic circulation Work – is the oxygen consumed by the myocardium to overcome the resistance to flow

4
C i r c u l a t I o n

5
Normal Circulatory Pressures
Preload to RV Afterload to RV Preload to LV Afterload to LV 5 3 2 3 1

6
Circulation

7
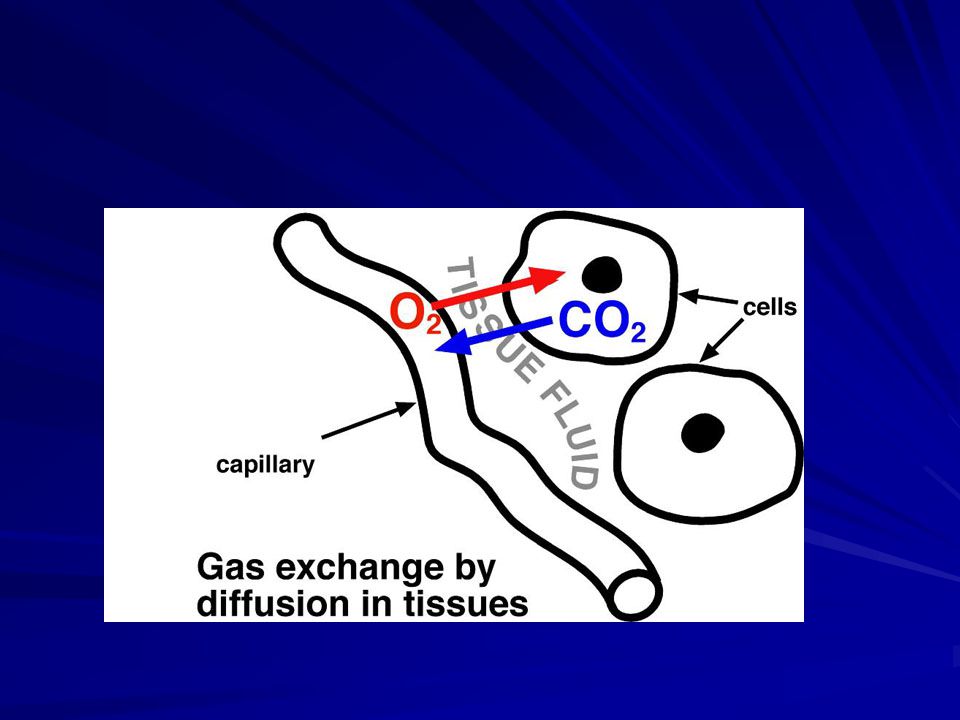
Alveolar Capillary Membrane

9
Normal Alveolar Capillary Membrane

10
Begin Pulmonary Edema

11
Interstitial Edema

12
Pulmonary Edema - Late

13
Pulmonary Artery Catheter

15
Pulmonary Artery Catheter

16
Arterial Blood Gas Interpretation

17
Oxygenation Saturation PO2 27 mmHg 50% 40 mmHg 75% 60 mmHg 90% 95 mmHg
97% 150 mmHg 100%

18
Oxyhemoglobin Dissociation Curve

19
Pulmonary Artery Catheter in Wedge Position

20
Case Study 1 An 18 year old white male was brought to the ED by CFD after being rescued from his car following a high speed collision with a parked truck. He is conscious, c/o of chest pain and is anxious. He was wearing his seat belt but still hit his chest on the steering wheel. His vital signs are: T 37, P 113, RR 23, B/P 100/ 70. CT scan of chest was unremarkable and he was brought to SICU for observation. He continued to have fluctuations in his blood pressure. A pulmonary artery catheter was placed.

21
Case Study 1 Area Normal 8 am 10:30 11:00 CVP 10 4 8 PAP 28 6 22 PWP
0 to 8 10 4 8 PAP 10 to 22 28 6 22 PWP 5 to 12 15 7 MAP 70 to 105 85 40 70 CO 4 to 8 LPM 5.9 2.5 5.7 HR 60 to 100 110 160 95 pH 7.35 to 45 7.37 7.22 7.39 PCO2 35 to 45 45 52 41 PaO2 80 to 100 65 50 88 PvO2 39 to 42 39 21 38

22
Cardiac Tamponade

23
Case Study 2 A 72 year old white female was admitted to the MICU with an exacerbation of COPD. She has emphysema and chronic bronchitis and a 40 pack year history of cigarette smoking. Breath sounds are bilaterally diminished, crackles and rhonchi. She has JVD and pedal edema. A pulmonary artery catheter was placed as she had sustained hypotension and SOB. Her VS are: T 37, P118, RR 32, B/P 150/90, FiO2 .28, HB 22 Gm%.

24
Case Study 2 Normal Noon 1600 1800 CVP 0 to 8 25 20 18 PAP 10 to 22 50 35 32 PWP 5 to 12 15 12 10 MAP 70 to 105 60 72 75 CO 4 to 8 LPM 3.9 4.5 4.7 HR 60 to 100 110 90 88 pH 7.35 to 45 7.35 7.39 7.38 PCO2 35 to 45 69 55 51 PaO2 80 to 100 46 85 78 PvO2 39 to 42 38 39

25
Case Study 3 A 25 year Hispanic male was admitted to the SICU after a thoracotomy for repair of his aorta following a gun shot wound to his chest. He has bilateral chest tubes. He is intubated and receiving full ventilatory support. His chest tube drainage for the last hour was 400 ml. He has bloody sputum and urine. His last CaO2 was 10.4 volumes% with a PaO2 of 110 and saturation of 95%. VS T 36, P148, RR 14, B/P 65/44.

26
Case Study 3 Normal 3 am 5:30 11:00 CVP 0 to 8 2 4 8 PAP 10 to 22 10 15 PWP 5 to 12 6 5 MAP 70 to 105 48 40 60 CO 4 to 8 LPM 2.94 3.5 5.7 HR 60 to 100 150 160 140 pH 7.35 to 45 7.22 7.20 7.32 PCO2 35 to 45 55 49 PaO2 80 to 100 110 94 PvO2 39 to 42 29 27 39

27
Case Study 4 A 52 year old white male with shortness of breath and chest pain was admitted to the ED. ECG showed ST elevation in 4 leads and his cardiac enzymes were markedly elevated. His vital signs were stable, SpO2 on NC at 2 LPM was 95%. He was taken to the cardiac cath lab and a diagnostic cardiac angiogram revealed 99% occlusion of his LAD. A coronary stent was placed and 15 minutes post intervention he began complaining again of severe SOB and chest pain. He was taken back to the cath lab. A pulmonary artery catheter was placed. A left heart catheterization revealed progression of the MI. His LVEDP is 32 and an intra aortic balloon was placed and counter pulsation started at 1:1.

28
Case Study 4 Normal 9 am 10:30 1600 CVP 0 to 8 10 8 PAP 10 to 22 28 20 PWP 5 to 12 35 15 MAP 70 to 105 72 47 65 CO 4 to 8 LPM 4.9 2.5 4.4 HR 60 to 100 110 80 pH 7.35 to 45 7.39 7.26 7.32 PCO2 35 to 45 40 50 38 PaO2 80 to 100 48 75 PvO2 39 to 42 36

29
Intra Aortic Balloon Counter Pulsation

30
Case Study 5 A 55 year old AA male was admitted to the MICU with acute SOB, cough, HTN and hypoxemia. He is oliguric and has required hemodialysis for the past 2 years. He is depressed and has not been following his dietary and fluid restrictions and has skipped his last 2 dialysis appointments. His VS are now T 37, P118, RR 35, B/P 200/135. He is receiving oxygen via venturi mask, FiO2 50%. He has a pulmonary artery catheter in place to monitor his cardiac status.

31
Case Study 5 Normal 8 am 10:30 11:00 CVP 0 to 8 25 19 12 PAP 10 to 22 40 32 28 PWP 5 to 12 22 18 15 MAP 70 to 105 150 110 100 CO 4 to 8 LPM 3.4 4.1 5.7 HR 60 to 100 95 86 pH 7.35 to 45 7.32 7.39 PCO2 35 to 45 49 38 PaO2 80 to 100 60 79 PvO2 39 to 42 34

32
Case Study 6 A 36 year old female was admitted to the ED with a CC of SOB and chest pain. She has no significant PMH, she does not smoke. She says that she hurt her ankle about two weeks ago and never went to the doctor about it. It is very painful and she has been almost immobilized for the past two weeks because it is just too painful to walk on. She has a cough and says her SOB came on rather suddenly after she went down to her basement to put some clothes in the laundry this morning. She is tachypneic, her MV is 12 LPM.

33
Case Study 6 Normal 5 am 24 hours later CVP 0 to 8 25 12 PAP 10 to 22 40 29 PWP 5 to 12 10 9 MAP 70 to 105 65 75 CO 4 to 8 LPM 6.4 5.1 HR 60 to 100 110 84 pH 7.35 to 45 7.36 7.39 PCO2 35 to 45 45 38 PaO2 80 to 100 85 PvO2 39 to 42 41

34
Saddle Pulmonary Embolism

36
Questions?? Thank you! You were great!!

38
Thoraco-abdominal Pump Mechanism

39
Small Vessels

41
Venous return

42
Oxygen carried in the blood

44
Chest x-ray of ARDS

45
Normal Chest x-ray

46
CT Scan of ARDS 35-year-old bone marrow transplant patient with respiratory failure from noncardiogenic pulmonary edema. The chest x-ray (left) shows a right sided pnbeumothorax, and bilateral ground glass density in the lungs. The HRCT scan (right) demonstrates relatively "airless" lungs despite high positive end expiratory pressure. The bronchovascular bundles are normal (A) suggesting that the hydrostatic pressure within the pulmonary capillaries is normal.
 shows a right sided pnbeumothorax, and bilateral ground glass density in the lungs. The HRCT scan (right) demonstrates relatively airless lungs despite high positive end expiratory pressure. The bronchovascular bundles are normal (A) suggesting that the hydrostatic pressure within the pulmonary capillaries is normal.")
48
Left-Sided Heart Failure
Pulmonary congestion occurs when left ventricle cannot pump well Dyspnea upon exertion, orthopnea, and paroxysmal nocturnal dyspnea Oliguria

49
Right-Sided Heart Failure
Congestion of viscera and peripheral tissues when right ventricle fails Jugular vein distention Dependent edema Hepatomegaly Ascites Weakness, anorexia, and nausea Weight gain

51
Sphincters Open

52
Sphincters Closed

53
Path of Blood

54
Major Blood Vessels

Similar presentations

















 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")

, awareness of heartbeat.>")






 It is the amount of blood pumped out by each side of the heart (actually each ventricle) in 1 minute.>")