Download presentation
Presentation is loading. Please wait.

1
Traumatic Brain Injury
Gill Sviri MD, M.Sc

2
Contents Epidemiology Biomechanics of primary brain injury
Mechanisms of secondary brain injury Clinical classification of head injury Treatment modalities – past, present, and future Controversies

3
Epidemiology 2 million pts/year evaluated in US (ED)
admissions/year 100,000 temporary or permanent disability Additional 30-50,000 die before ED arrival Peaks y.o and > 65 Death 3.4 x more common in males Most common – MVC’s and gun-shot

4
Physiology – Hemodynamics
Oxygen consumption - 20% of total body Requires 15% of normal cardiac output CBF – 50 ml/100g/min Autoregulation maintained btwn MAP 60–150 or CPP hyperTN, alkalosis, hypocarbia = v/c hypoTN, acidosis, hypercarbia, hypoxia = v/d

5
Physiology - ICP Craniospinal space non-expandable
Sum of brain, CSF, and blood constant Insults brain volume – edema CSF – obstruction blood volume – ICH, hematoma, v/d, congestion compensation – up to 50–100 ml CSF displacement 1st brain elasticity

6
Physiology - CPP CPP = MAP – ICP
< autoregulation lost/vasoparalysis vasodilation incr. ICP decr. CPP As ICP approaches MAP CPP ceases cell death

7
Brain Injury dynamic process of… primary injury secondary injury
occurs at time of head trauma irreversible prevention strategies secondary injury minutes to days post injury therapy directed at limiting this further brain cell death

8
Biomechanics – primary injury
direct injury impact by object or compression mechanism external signs of trauma skull plastic deformity absorbs energy fracture if force sufficient transmitted force to brain tissue injury pattern – skull #, epidural, contusion associated indirect injury other injury pattern

9
Biomechanics – primary injury
indirect injury cranial contents set into vigorous motion acceleration/deceleration, rotational, angular forces bridging subdural vessel strain differential acceleration – shear injuries impact of brain on inner aspect of skull injury pattern – subdural, DAI, concussion, countercoup

10
Secondary injury This is where we intervene to limit further brain cell damage mechanisms systemic insults intracranial lesions neuroendocrine disturbance membrane failure abnormal ion fluxes edema

11
Secondary injury

12
PATHOPHYSIOLOGY OF TBI
Primary Brain Damage Energy Failure Glutamate Release Lactate Acidosis Membrane Failure Massive Ca entry Brain Edema Free radicals release Vasodilatation Increased CBV Increased ICP Neuronal Death Secondary Brain Damage

13
Secondary injury - preventable
Treatable secondary insults to the brain in trauma patients include… CPP (goal > 60 mmHg) hypotension (goal SBP > 90) - not related to head injury! ICP (goal < ) hypoxia (goal PaO2 > 60mmHg) can be head injury (brainstem) or other airway/breathing/oxygenation/ventilation anemia (goal Hct > 30%) seizures – increased metabolic demand
 hypotension (goal SBP > 90) - not related to head injury! ICP (goal < ) hypoxia (goal PaO2 > 60mmHg) can be head injury (brainstem) or other airway/breathing/oxygenation/ventilation. anemia (goal Hct > 30%) seizures – increased metabolic demand.")
14
Secondary injury - ?preventable
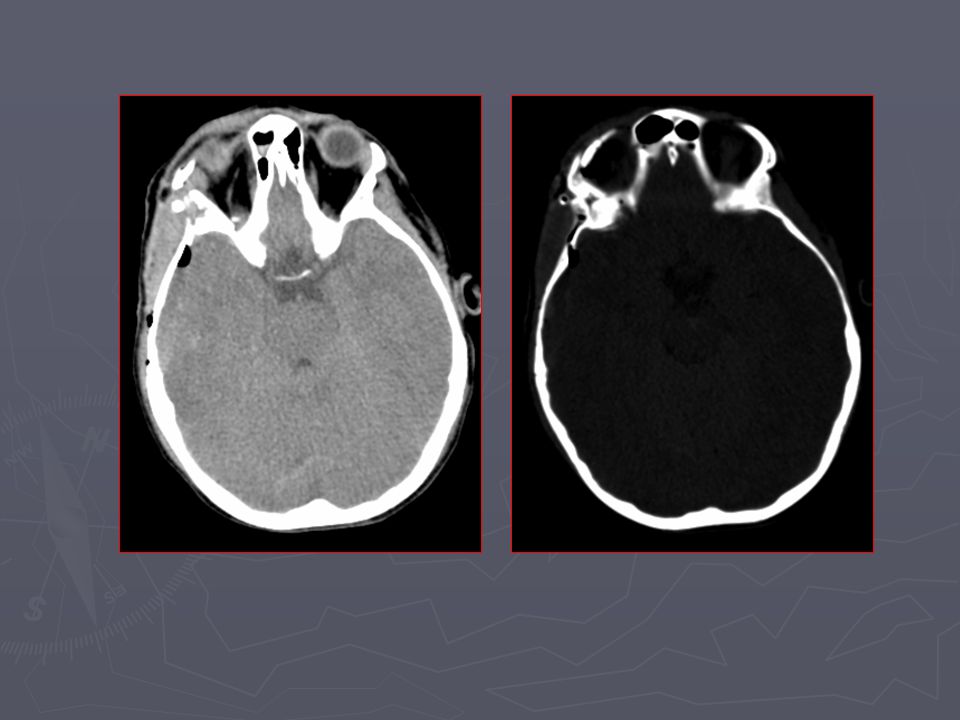
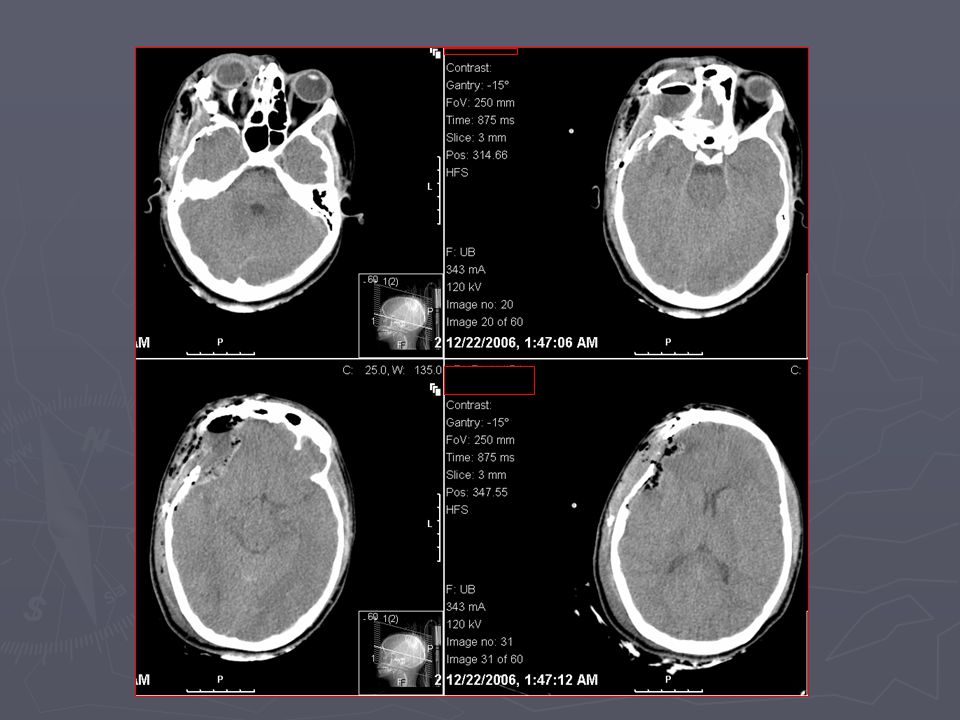
Edema – local/global CBF disturbance diffuse - comprimise ventricles, loss of sulci, effaced basal cisterns focal – hypodensity around lesion +/- shift vasogenic – BBB failure, direct injury to cell membranes, pinocytosis incr. osmotic gradient cytotoxic – membrane pump failure, hypoxia, ischemia

15
Clinical Classification
determined by post-resucitation GCS Minimal – GCS 15 and no LOC/amnesia Mild – GCS 13/14-15 with LOC/amnesia Moderate – GCS 9-12/13 Severe – GCS 8 or less

16
Severe head injury Severe – GCS 8 or less 10% of all TBI 40% mortality
25% require neurosurgical intervention

17
Severe head injury CT findings subdural – 30% epidural – 0.5 – 1%
subarachnoid – 33% intracerebral hematoma – 12% subdural hygroma – 10%

18
Treatment airway and breathing BP Hyperventilation
Hyper-osmotic agents CSF drainage Surgery Seizure prophylaxis

19
Moderate head injury moderate = GCS 9-12/13 10% of all TBI
20% mortality

20
CLASSIFACTION OF CLOSE TBI
Diffuse TBI Focal TBI Skull fractures Intracranial Hemorrhages Brain Contusions Brain Concussion Diffuse Axonal Injury EDH SDH ICH Brain Edema Increased ICP

21
A MAJOR THREAT: INCREASED ICP

22
LINEAR SKULL FRACTURES

25
DEPRESSED SKULL FRACTURES
Skull deformation Compression of brain Higher risk of bleeding

33
DEPRESSED SKULL FRACTURES
Complications: Wound and CSF infections CSF leak Neural injury and deficit

34
BASE SKULL FRACTURES High energy loading CSF leak and infection
Cranial nerve damage

36
ACUTE EPIDURAL HEMATOMA
Lucid interval is suggestive Good prognosis

37
ACUTE EPIDURAL HEMATOMA
Most often due to skull fracture Brain damage is uncommon

38
ACUTE EPIDURAL HEMATOMA

41
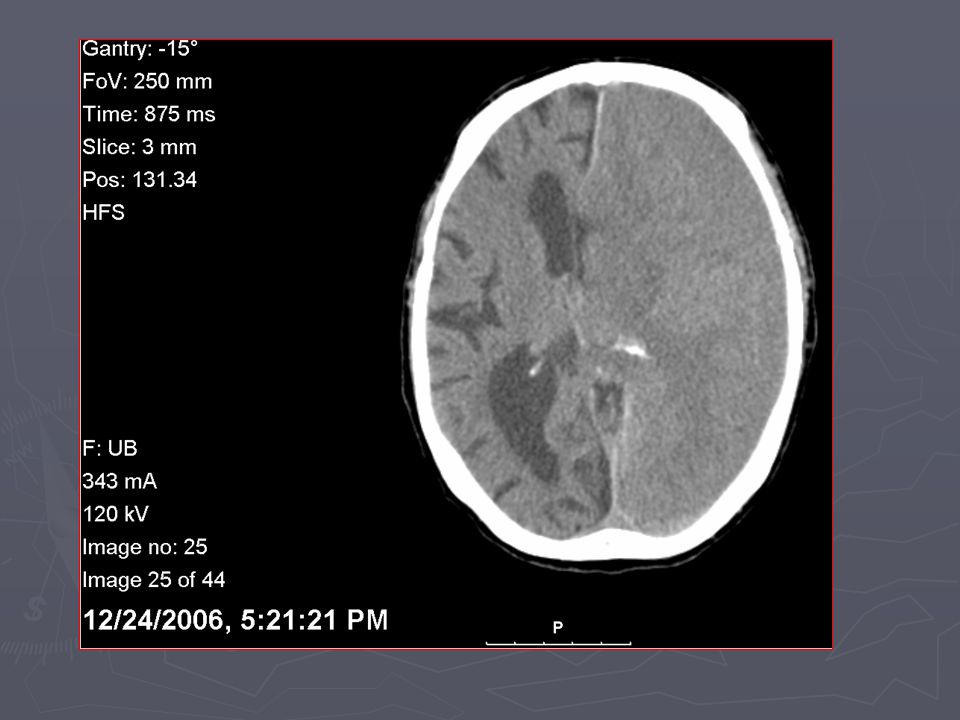
ACUTE SUBDURAL HEMATOMA
Always associated with significant TBI Often grim prognosis

42
ACUTE SUBDURAL HEMATOMA
Massive edema is the rule Disproportionate midline shift High mortality and morbidity

45
BRAIN CONTUSIONS: COUP AND CONTRE-COUP

46
BRAIN CONTUSIONS: PATHOPHYSIOLOGY

47
BRAIN CONTUSIONS: PATHOLOGY

48
EVOLVING BRAIN CONTUSIONS: THE PATIENT WHO TALK AND DIE

50
SUBARACHNOID HEMORRHAGE

52
DIFFUSE AXONAL INJURY:
PATHOPHYSIOLOGY

53
DIFFUSE AXONAL INJURY: “THE DISCONNECTED BRAIN”

54
DIFFUSE AXONAL INJURY: “THE DISCONNECTED BRAIN”

55
DIFFUSE AXONAL INJURY: “THE DISCONNECTED BRAIN”

57
GUN SHOT WOUNDS: E=mc2

58
GUN SHOT WOUNDS: E=mc2 Directly depends on velocity missile
Through and through usually fatal Associates focal and diffuse TBI

Similar presentations