Download presentation
Presentation is loading. Please wait.

1
ברקע: סכרת מסוג II, ידועה 20 שנה, אינה מאוזנת היטב מחלת לב איסכמית, עברה אוטם שריר הלב לפני 5 שנים עישון של חפיסת סיגריות ליום מזה 40 שנה בחודשים האחרונים שמה לב לנפיחות גוברת ברגליים, נפיחות בבטן וקוצר נשימה במאמצים קלים. עלתה 7 ק"ג במשקלה ב- 3 החודשים האחרונים. מ.כ., בת 65

2
Approach to the adult with edema Ilan Krause Dept. of Medicine E Rabin Medical Center, Beilinson Hospital

3
Palpable swelling produced by expansion of the interstitial fluid volume several litersThe expansion takes several liters before overt manifestations of edema (i.e. weight gain of several kg.) Massive and generalized edema = Anasarca Edema
 Massive and generalized edema = Anasarca Edema.")
4
Clinical conditions associated with the development of edema Increased capillary hydraulic pressure A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including nephrotic syndrome b. Drugs: minoxidil, NSAIDS, estrogens c. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2 Local venous obstruction C. Decreased arteriolar resistance 1. Calcium channel blockers 2. Idiopathic edema Hypoalbuminemia A. Protein loss 1. Nephrotic syndrome 2. Protein-losing enteropathy B. Reduced albumin synthesis 1. Liver disease 2. Malnutrition Increased capillary permeability A. Idiopathic edema B. Burns C. Trauma D. Inflammation or sepsis E. Allergic reactions, F. Diabetes mellitus G. Interleukin-2 therapy H. Malignant ascites Lymphatic obstruction or interstitial oncotic pressure A. Postmastectomy B. Nodal enlargement due to malignancy C. Hypothyroidism D. Malignant ascites

5
Ernest Henry Starling 1866 - 1927

6
PATHOPHYSIOLOGY Alteration in capillary hemodynamics movement of fluid from vascular space into the interstitium. increased capillary hydrostatic pressure

7
Ernest Henry Starling 1866 - 1927

8
PATHOPHYSIOLOGY Alteration in capillary hemodynamics movement of fluid from vascular space into the interstitium. decreased capillary oncotic pressure increased capillary hydrostatic pressure

9
Ernest Henry Starling 1866 - 1927

10
PATHOPHYSIOLOGY Alteration in capillary hemodynamics movement of fluid from vascular space into the interstitium. increased capillary hydrostatic pressure decreased capillary oncotic pressure increased capillary permeability

11
The three most important causes of edema Right-sided heart failure Nephrotic-range proteinuria Cirrhosis

12
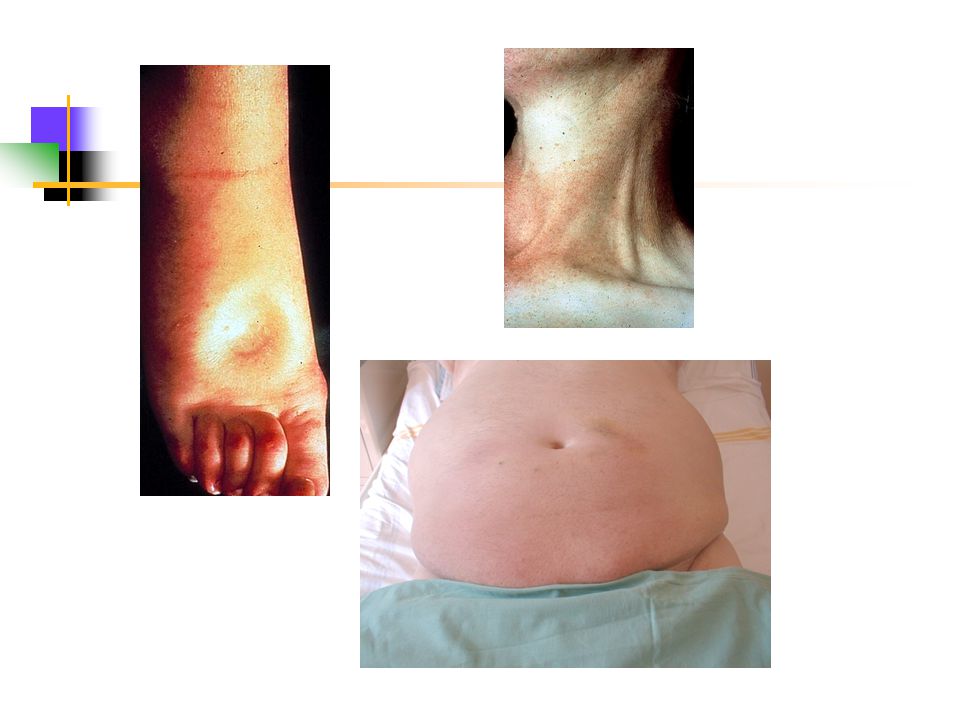
Right Heart Failure Increased venous pressure behind the right side of the heart increased capillary hydrostatic pressure –Congested jugular veins –Enlarged & tender liver –Peripheral edema Anasarca –Shortness of breath

13
Cirrhosis Increased venous pressure below the diseased liver Ascites edema in the lower extremities. Signs of portal hypertension (distended abdominal wall veins & splenomegaly) Primary liver disease vs. Cardiac cirrhosis
 Primary liver disease vs. Cardiac cirrhosis.")
14
Nephrotic syndrome Heavy proteinuria (> 3.0 g/day) Hypoalbuminemia Hyperlipidemia Peripheral edema
 Hypoalbuminemia Hyperlipidemia Peripheral edema")
15
Edema in Nephrotic syndrome 2 factors: 1.sodium retention due to underlying renal disease 2.diminished transcapillary oncotic pressure gradient Typically- periorbital and peripheral edema, occasionally also ascites

16
Other causes of Edema

17
Venous insufficiency limited to the lower extremities may be unilateral postphlebitic syndrome poor response to diuretics

18
Drug-induced edema NSAIDs Antihypertensive agents –Calcium channel antagonists –Minoxidil –Hydralazine –Clonidine –Methyldopa Glucocorticoids Anabolic steroids Estrogens Progestins Cyclosporine Growth hormone Interleukin 2

19
Premenstrual edema Retention of water and increase in weight which occurs during or preceding menstruation. The etiology is poorly understood The edema tends to be generalized, and resolves during a diuresis that occurs with the onset of menses.

20
Idiopathic edema Young women (usually obese) No cardiac, hepatic, or renal disease Periodic episodes of edema (unrelated to menstrual cycle) Orthostatic retention of sodium and water Frequently accompanied by abdominal distention Pathogenesis- unknown (capillary leak? diuretic-induced edema?) Treatment: low-sodium diet stop diuretic therapy
 Treatment: low-sodium diet stop diuretic therapy.")
21
Nonpitting edema Lymphedema Pretibial myxedema Post mastectomy Lymphatic disease Malignancy Infection thyroid diseases

22
Clinical conditions associated with the development of edema Increased capillary hydraulic pressure A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including nephrotic syndrome b. Drugs: minoxidil, NSAIDS, estrogens c. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2. Local venous obstruction C. Decreased arteriolar resistance 1. Calcium channel blockers 2. Idiopathic edema Hypoalbuminemia A. Protein loss 1. Nephrotic syndrome 2. Protein-losing enteropathy B. Reduced albumin synthesis 1. Liver disease 2. Malnutrition Increased capillary permeability A. Idiopathic edema B. Burns C. Trauma D. Inflammation or sepsis E. Allergic reactions, F. Diabetes mellitus G Interleukin-2 therapy H. Malignant ascites Lymphatic obstruction or interstitial oncotic pressure A. Postmastectomy B. Nodal enlargement due to malignancy C. Hypothyroidism D. Malignant ascites

23
Clinical conditions associated with the development of edema Increased capillary hydraulic pressure A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including nephrotic syndrome b. Drugs: minoxidil, NSAIDS, estrogens c. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2. Local venous obstruction C. Decreased arteriolar resistance 1. Calcium channel blockers 2. Idiopathic edema

24
Increased capillary hydrostatic pressure A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including nephrotic syndrome b. Drugs: minoxidil, NSAIDS, estrogens c. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2. Local venous obstruction

25
Clinical conditions associated with the development of edema Increased capillary hydraulic pressure A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including nephrotic syndrome b. Drugs: minoxidil, NSAIDS, estrogens c. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2. Local venous obstruction C. Decreased arteriolar resistance 1. Calcium channel blockers 2. Idiopathic edema Hypoalbuminemia A. Protein loss 1. Nephrotic syndrome 2. Protein-losing enteropathy B. Reduced albumin synthesis 1. Liver disease 2. Malnutrition Increased capillary permeability A. Idiopathic edema B. Burns C. Trauma D. Inflammation or sepsis E. Allergic reactions, F. Diabetes mellitus G Interleukin-2 therapy H. Malignant ascites Lymphatic obstruction or interstitial oncotic pressure A. Postmastectomy B. Nodal enlargement due to malignancy C. Hypothyroidism D. Malignant ascites

26
Clinical conditions associated with the development of edema Hypoalbuminemia A. Protein loss 1. Nephrotic syndrome 2. Protein-losing enteropathy B. Reduced albumin synthesis 1. Liver disease 2. Malnutrition

27
Hypoalbuminemia A. Protein loss 1. Nephrotic syndrome 2. Protein-losing enteropathy B. Reduced albumin synthesis 1. Liver disease 2. Malnutrition

28
Clinical conditions associated with the development of edema Increased capillary hydraulic pressure A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including nephrotic syndrome b. Drugs: minoxidil, NSAIDS, estrogens c. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2. Local venous obstruction C. Decreased arteriolar resistance 1. Calcium channel blockers 2. Idiopathic edema Hypoalbuminemia A. Protein loss 1. Nephrotic syndrome 2. Protein-losing enteropathy B. Reduced albumin synthesis 1. Liver disease 2. Malnutrition Increased capillary permeability A. Idiopathic edema B. Burns C. Trauma D. Inflammation or sepsis E. Allergic reactions, F. Diabetes mellitus G Interleukin-2 therapy H. Malignant ascites Lymphatic obstruction or interstitial oncotic pressure A. Postmastectomy B. Nodal enlargement due to malignancy C. Hypothyroidism D. Malignant ascites

29
Clinical conditions associated with the development of edema Increased capillary permeability A. Idiopathic edema B. Burns C. Trauma D. Inflammation or sepsis E. Allergic reactions, F. Diabetes mellitus G. Interleukin-2 therapy H. Malignant ascites

30
Increased capillary permeability A. Idiopathic edema B. Burns C. Trauma D. Inflammation or sepsis E. Allergic reactions, F. Diabetes mellitus G. Interleukin-2 therapy H. Malignant ascites

31
Clinical conditions associated with the development of edema Increased capillary hydraulic pressure A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including nephrotic syndrome b. Drugs: minoxidil, NSAIDS, estrogens c. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2. Local venous obstruction C. Decreased arteriolar resistance 1. Calcium channel blockers 2. Idiopathic edema Hypoalbuminemia A. Protein loss 1. Nephrotic syndrome 2. Protein-losing enteropathy B. Reduced albumin synthesis 1. Liver disease 2. Malnutrition Increased capillary permeability A. Idiopathic edema B. Burns C. Trauma D. Inflammation or sepsis E. Allergic reactions, F. Diabetes mellitus G Interleukin-2 therapy H. Malignant ascites Lymphatic obstruction or interstitial oncotic pressure A. Postmastectomy B. Nodal enlargement due to malignancy C. Hypothyroidism D. Malignant ascites

32
Clinical conditions associated with the development of edema Lymphatic obstruction or interstitial oncotic pressure A. Postmastectomy B. Nodal enlargement due to malignancy C. Hypothyroidism D. Malignant ascites

33
Lymphatic obstruction or increased interstitial oncotic pressure A. Postmastectomy B. Nodal enlargement due to malignancy C. Hypothyroidism D. Malignant ascites

34
History taking

35
Any disorder or drug that can cause cardiac, hepatic, or renal disease (IHD, COPD, HTN, alcohol abuse etc.) Is the edema intermittent or persistent? Where is the edema located?

36
Physical examination

37
Pitting vs. non-pitting Distribution of the edema Localized or diffuse ? Periorbital ? Jugular veins ? Ascites ? Legs Stigmata of chronic liver disease Physical findings of heart failure

38
Further evaluation Chest X rays Cardiomegally? Pulmonary congestion? Pleural effusion?

39
Further evaluation Echocardiography Chest X rays Wall motion abnormalities LV function RV function Pulmonary hypertension ?

40
Further evaluation Abdominal US Chest X rays Echocardiography Liver size & morphology Hepatic veins Presence of ascites Renal morphology

41
Further evaluation 24h urinary protein excretion Levels of liver enzymes, INR, albumin Chest X rays Echocardiography Abdominal US

42
Principals of therapy Reversal of the underlying disorder (if possible, but usually not) Dietary sodium restriction Diuretic therapy Only for pitting edema!
 Dietary sodium restriction Diuretic therapy Only for pitting edema!")
43
Before initiating diuretics, consider the following questions: When must edema be treated? What are the consequences of the removal of edema fluid? How rapidly should edema fluid be removed?

44
When must edema be treated? Almost never !

45
What are the consequences of the removal of edema fluid? Sodium and water retention by the kidney is compensatory! – it raises the effective circulating volume. Diuretic therapy may have a deleterious effect on systemic hemodynamics even though it reduces the edema!! Therefore- use diuretics, but cautiously ! monitoring the Urea and creatinine concentration

46
Use of Diuretics Start with a loop diuretic (furosemide) Watch for electrolyte complications: –Hypokalemia –Hyponatremia –Metabolic alkalosis For resistant edema- –Use high-dose intravenous loop diuretics – Use combination of diuretics to act at different sites in the nephron Thiazides, Spironolactone
 Watch for electrolyte complications: –Hypokalemia –Hyponatremia –Metabolic alkalosis For resistant edema- –Use high-dose intravenous loop diuretics – Use combination of diuretics to act at different sites in the nephron Thiazides, Spironolactone")
47
Diuretic dose Dose-response curve Diuresis begins with as little as 10 mg of fusid, with maximal effect at IV 40 mg. The effective dose is higher in CHF, advanced cirrhosis, or renal failure, due to decreased renal perfusion.

48
Intravenous vs. oral therapy Onset of diuresis is earlier and the peak diuresis is greater with IV therapy This difference is not likely to be important in stable patients The intravenous equivalent for Fusid is one-half the oral dose

49
Special considerations NS Cirrhosis Higher than usual doses of a loop diuretic may be required Renal failure Binding of the loop diuretic by albumin in the tubular lumen

50
Special considerations NS Cirrhosis Spironolactone is the preferred initial diuretic The diuresis should proceed very slowly ! In patients with tense ascites, consider paracentesis

51
בת 65 ברקע: סכרת מסוג II, ידועה 20 שנה, אינה מאוזנת היטב מחלת לב איסכמית, עברה אוטם שריר הלב לפני 5 שנים עישון של חפיסת סיגריות ליום מזה 40 שנה בחודשים האחרונים שמה לב לנפיחות גוברת ברגליים, נפיחות בבטן וקוצר נשימה במאמצים קלים. עלתה 7 ק"ג במשקלה ב- 3 החודשים האחרונים. ובחזרה אל מ.כ....

52
בבדיקה גופנית Pitting edema of the lower limbs Distended jugular veins Distended abdomen with “ shifting dulness ” Dullness on percussion of right lung

54
Chest X-rays

55
בדיקות עזר נוספות אקו לב- –ירידה בינונית בתפקוד חדר שמאל –הרחבת חדר ימין וירידה קשה בתפקודו –יתר לחץ-דם ריאתי איסוף שתן לחלבון ליממה: 6.5 גרם

56
אבחנות Anasarca IHD, s/p Myocardial infarction Congestive heart failure Pulmonary HT with cor pulmonale Diabetes mellitus type II Nephrotic syndrome

57
Management Stop smoking Control hyperglycemia Specific therapy for heart failure: –ACE inhibitors – blockers –Diuretic therapy- fusid (consider adding spironolactone) Closely watch urine output, rate of weight reduction, levels of urea & creatinine
 Closely watch urine output, rate of weight reduction, levels of urea & creatinine")
58
Thank you !

Similar presentations


 fluid volume. Weight gain precedes overt edema Massive and.>")







>")
 Definition NS is an accumulation of symptoms and signs and is characterized by proteinuria, hypoproteinemia, edema, and hyperlipidemia.>")

 intracellular. (1/3)extracellular (interstitial fluid) 5% blood plasma. edema = an accumulation of interstitial.>")


 saying that her legs have been swollen for a month. On examination you find that she has.>")


