Download presentation
Presentation is loading. Please wait.

1
Student Name: Dr Gerhardus Coetzer Student No: 1999061854 Patient No: 3 Date: 10/09/2011 Diagnosis: AC Joint Ligament Strain Gr 1

2
PATIENT DETAILS 27 year old male patient Professional rugby player

3
COMPLAINT Complaining of pain in right shoulder after tackling another player. Painful to lift up shoulder and horizontal flexion.

4
FURTHER HISTORY FAMILY HISTORY – Normal MEDICAL HISTORY – Normal EXERCISE – Professional rugby player during in season – 2 sets of weight training per week – 5 x functional exercise and contact sessions

5
CLINICAL EXAMINATION Observation – Normal Passive Movements – Most pain with horizontal flexion – Minimal pain with abduction Active – Same as above Against Resistance – Same as above – Strength is equal bilateral – More pain experienced with resistance

6
SPECIAL INVESTIGATIONS Paxinos Test – Positive (AC Joint compression) – No Ultra sound done – No MRI scan done
 – No Ultra sound done – No MRI scan done")
7
BIOMECHANICAL EXAMINATION Biomechanical Examination – Normal X-Ray – Normal

8
SUMMARY CLINICAL – Patient has a GR 1 AC joint sprain of the right shoulder PERSONAL – Patient is worried about the time that he will not be able to train. – Worried about loss of match fitness – Worried about loss of match fees CONTEXTUAL – Professional rugby player with a GR 1 AC joint sprain of the right shoulder

9
PROBLEM LIST ACTIVE – Reducing inflammation restoring pain free R.O.M PASSIVE – Improving strength and stability in the AC joint capsule through isometric weight training – Maintain cardio vascular fitness

10
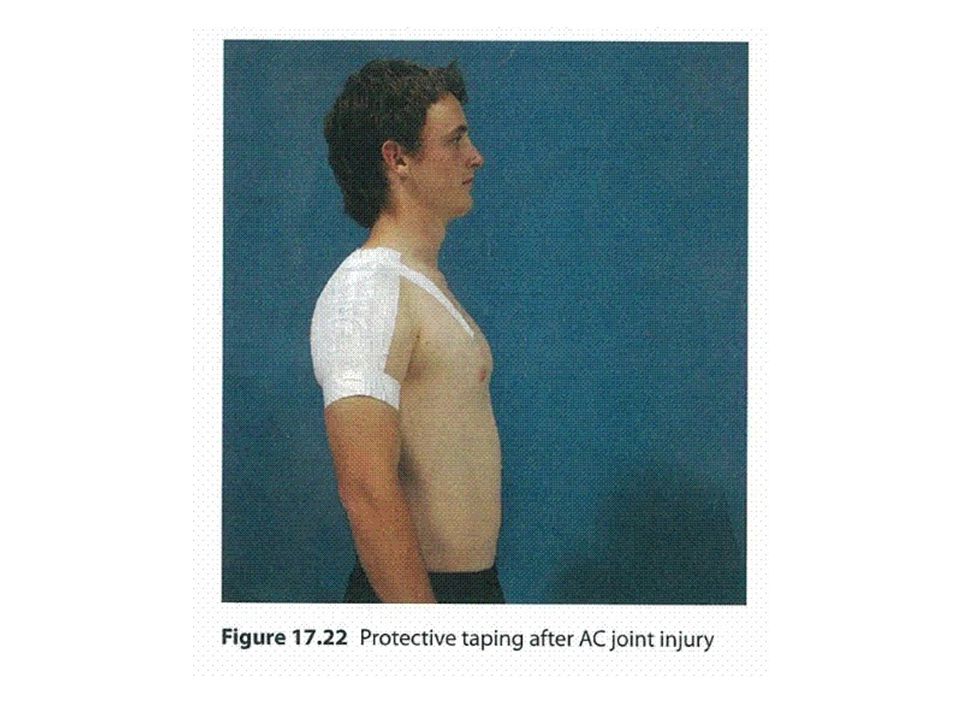
PLAN Rested injury for 3 days Started with daily sessions of physiotherapy U/S to reduce inflammation and improving R.O.M through stretching. Isometric weight training as soon as pain allows. As prescribed by bio kinetics. To return to sport as soon as there is pain free R.O.M, isometric weight training and functional exercise. Strapping the AC joint when returning to contact.

12
PROGRESSION The patient started weight training after 10 days since original injury. Progressed to contact and playing again in 3 weeks.

13
DISCUSSION Anatomy of the AC Joint BONES – Consists of distal part of clavical and acromion of the scapula. – The boney part of the clavical has a slightly convexed facet where as the acromion has a slightly concave facet. – Both articular surfaces are covered by fibro-cartelidge. The lateral end of the clavical tend to override the cromion, which together with the slope of their articulating surfaces favours displacement of the acromion downwards and under the clavical in dislocations.

14
JOINT CAPSULE – The AC joint is covered by the joint capsule which is a fibrous capsule. – The capsule is thickest and strongest above where it is reinforced by the fibres of trapezius. LIGAMENTS – Apart from the capsular thickening the strength of the AC joint is provided by an extra capsular accessory ligament, the coracoclavicular ligament. – The coracoclavicular ligament is made up by 2 different ligaments, named the trapezoid ligament, anterolateral and the conoid ligament posteromedial.

16
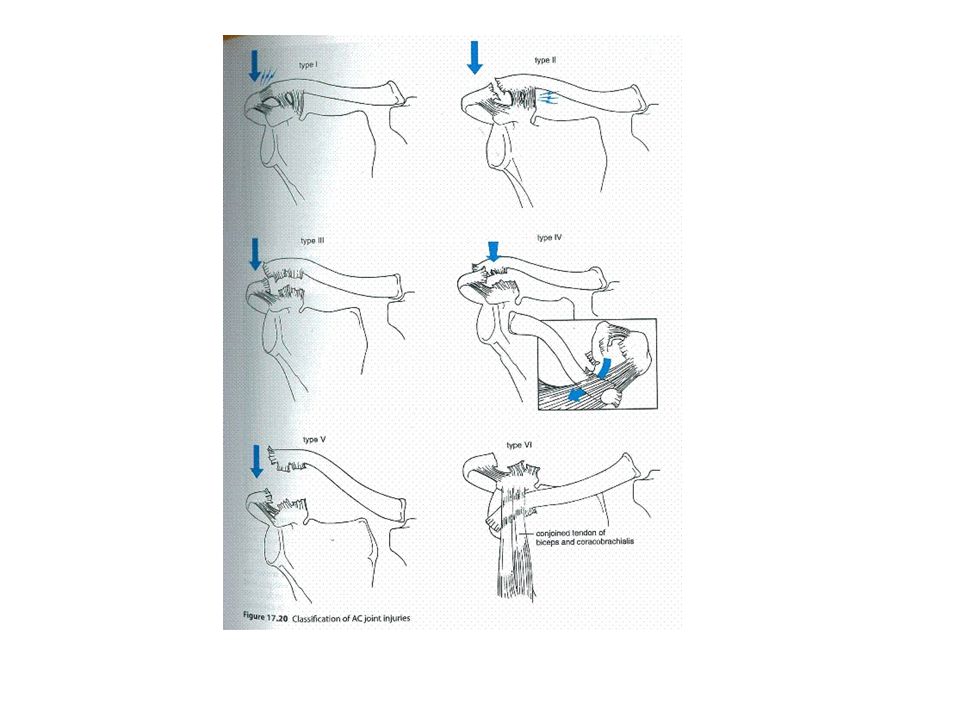
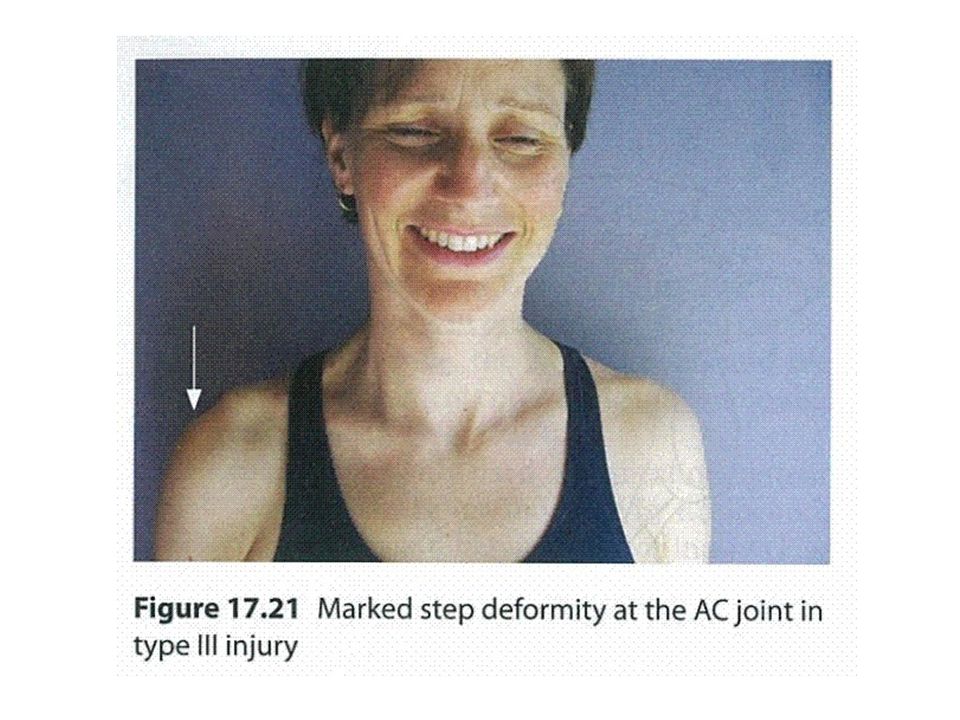
DISCUSSION (cont) AC Joint Injuries ACUTE AC JOINT INJURIES – Most common way of injuring AC joint is falling onto the tip of the shoulder. – The most common form of classification form AC joint injuries is the modified Rockwood classification, which recognises 6 different types of injuries, being Type 1 injury corresponds to sprain of the capsule. Type 2 corresponds to a complete tear of the AC ligaments with sprain of the coracoclavicular ligament, usually a palpable step deformity. Type 3 &5 consist of complete tears of the coracoclavicular ligaments and a marked stepped deformity is present.

17
Type 3 – 5 injuries can be distinguished from each other radiographically by the amount of displacement. Type 4 injuries are characterised by post terior displacement of the clavical and type 6 injuries have inferiorly displaced clavical into either a subacromial or subcoracoid position.

20
DISCUSSION (cont) Management Management is based on the general principles of management of ligamentous injuries. Applying ice and wearing a sling for pain relief is usually the first step. Isometric strengthening should be commenced once pain permits. GR 3 injuries is controversial, most of these injuries have been treated surgically. A new study has proven that immobilisation through the use of a K-wire has similar outcomes as to more invasive surgery. (Bernd et al, 2009) Return to sport is possible when there is no further localised tenderness and full pain free R.O.M.
 Return to sport is possible when there is no further localised tenderness and full pain free R.O.M..")
21
LEARNING EXPERIENCE Learnt the correct management and classification of AC joint injuries.

22
REFERENCED TEXT 1.Anatomy and Human Movement – Structure and Function. 5 th Edition – Nigel Palastanga, Derek Field, Roger Soames 2.Clinical Sport Medicine. 3 rd Edition – Peter Brukner, Karim Khan 3.Mid-term outcomes comparing temporary K- wire fixation versus PDS augmentation of Rockwood grade III acromioclaciular joint seperations. – Bernd A Leidel, Volker Braunstein, Susann Pilotto, Wolf Mutschler, Chlodwig Korchoff, 2011.

Similar presentations


 Joint Sprain. What is the AC joint? Its a joint in the shoulder that consists of the lateral end of the clavicle and the acromion.>")



 Is one of a pair of ligaments that are found in the middle.>")













