Download presentation
Presentation is loading. Please wait.

2
M. Saleh Massoud, MD. Lecturer of Anesthesiology & Intensive Care Ain-Shams University

3
Case Scenario A 27-year-old male was involved in a high speed RTA. Ambulance services brought him to our ER. Primary survey revealed : A: Clear airway, central trachea B: Respiratory rate 20, Pulse oximetry reading 95% on high flow oxygen C: Heart rate 125, Arterial blood pressure 90 ⁄ 60 mmHg D: Glasgow Coma Scale (GCS) 10 ⁄ 15 (E4, V2, M4), Symmetrical reactive pupils. E: Exposure showed........
 10 ⁄ 15 (E4, V2, M4), Symmetrical reactive pupils. E: Exposure showed")
7
20 min after arrival: The patient became hemodynamically unstable with marked hypotension (BP 60 ⁄ 30), tachycardia (HR 167) Fall in hemoglobin (Hb) level from 11 g.dl -1 to 5 g.dl -1.
, tachycardia (HR 167) Fall in hemoglobin (Hb) level from 11 g.dl -1 to 5 g.dl -1.")
8
Causes of death following multiple trauma Current Orthopaedics (2004) 18, 304–310
 18, 304–310")
9
Hemorrhagic shock Due to inadequate blood flow for tissue oxygenation. Caused by: External blood loss Occult blood loss Inadequate resuscitation Aortic or great vessel injury Diagnosed by: Tachycardia Hypotension Cool clammy skin Decreased loc Low urine output

10
Classification of Hemorrhage American College of Surgeons Committee on Trauma Advanced Trauma Life Support Program CLASS ICLASS IICLASS IIICLASS IV Blood loss (ml)Up to 750750-1,5001,500-2,000 2,000 Blood loss (% blood volume) Up to 15%15%-30%30%-40% 40% Pulse rate<100>100>120 140 Blood pressureNormal Decreased Pulse pressure (mmHg) Normal or increasedDecreased Capillary refill testNormalPositive Respiratory rate14-2020-3030-40>35 Urine output (ml/hr) 30 20-305-15Negligible CNS — mental status Slightly anxiousMildly anxiousAnxious, confused Confused, lethargic
Up to ,5001,500-2,000 2,000 Blood loss (% blood volume) Up to 15%15%-30%30%-40% 40% Pulse rate<100>100>120 140 Blood pressureNormal Decreased Pulse pressure (mmHg) Normal or increasedDecreased Capillary refill testNormalPositive Respiratory rate >35 Urine output (ml/hr) Negligible CNS — mental status Slightly anxiousMildly anxiousAnxious, confused Confused, lethargic")
11
Traditional Trauma Resuscitation Aggressive fluid resuscitation [2 L Crystalloid] Packed RBCs FFP & Cryoprecipitate Transient response No response Active bleeding After 6-10 u PRBC
![Traditional Trauma Resuscitation Aggressive fluid resuscitation [2 L Crystalloid] Packed RBCs FFP & Cryoprecipitate Transient response No response Active bleeding After 6-10 u PRBC](http://images.slideplayer.com/12/3428884/slides/slide_11.jpg "Traditional Trauma Resuscitation Aggressive fluid resuscitation [2 L Crystalloid] Packed RBCs FFP & Cryoprecipitate Transient response No response Active bleeding After 6-10 u PRBC")
12
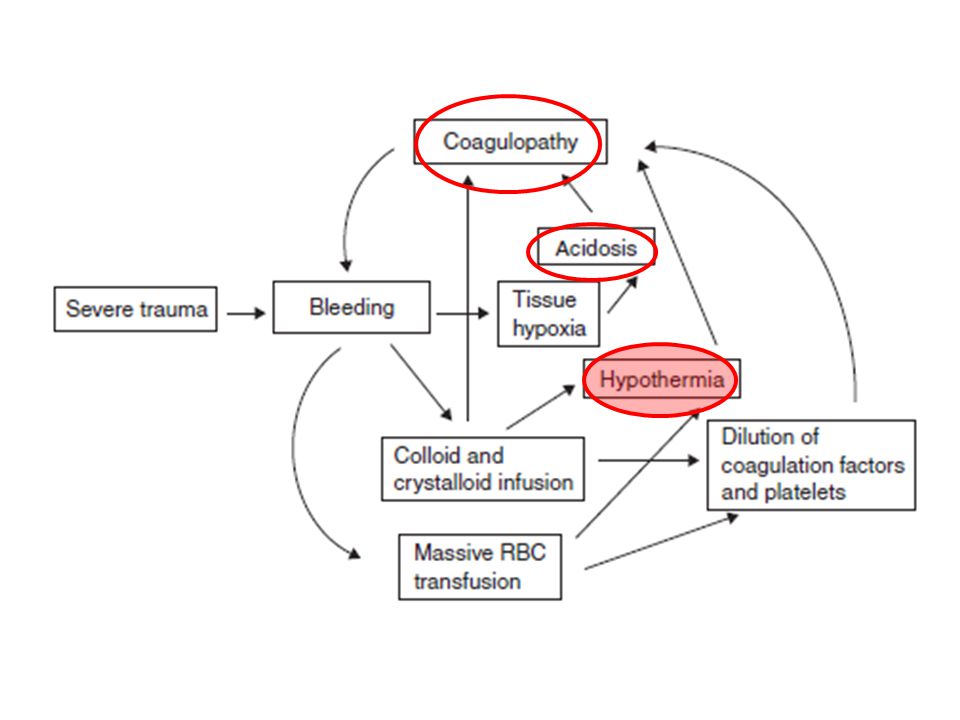
The bloody vicious circle

14
The Lethal Triad in Trauma

16
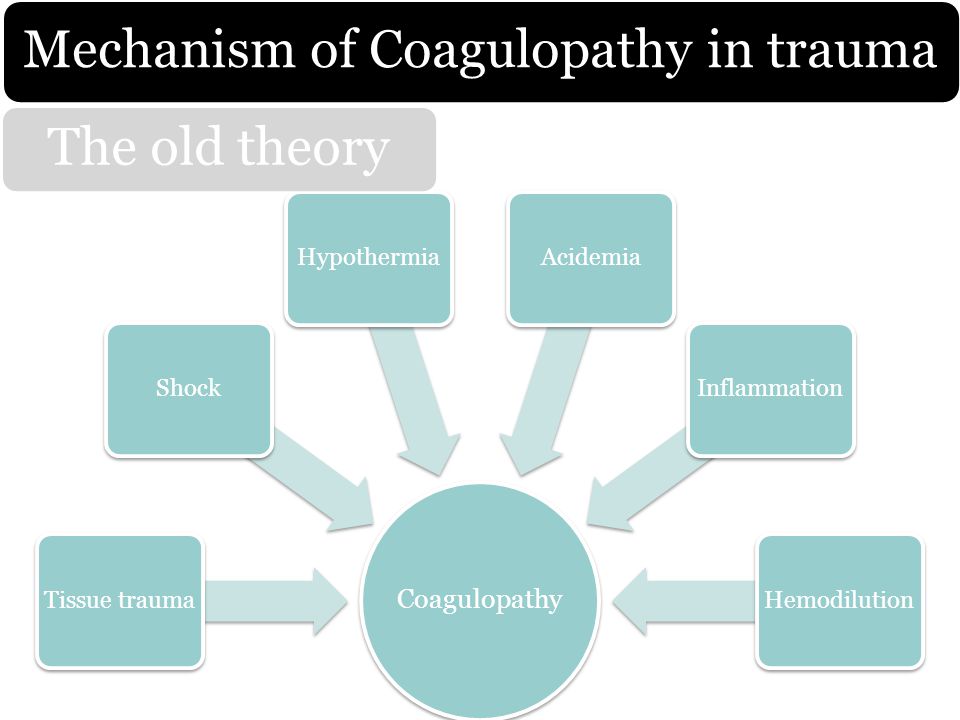
Coagulopathy Tissue traumaShockHypothermiaAcidemiaInflammationHemodilution Mechanism of Coagulopathy in trauma The old theory

17
coagulopathy Systemic anticoagulation Hyperfibrinolysis Mechanism of Coagulopathy in trauma The new theory Endothelium releases tPA Hyper fibrinolysis Fibrinogen depletion Endothelium express thrombomodulin TM complex es with Thrombin Activation of protein C pathway Extrinsic Pathway is inhibited Systemic anticoagulation

20
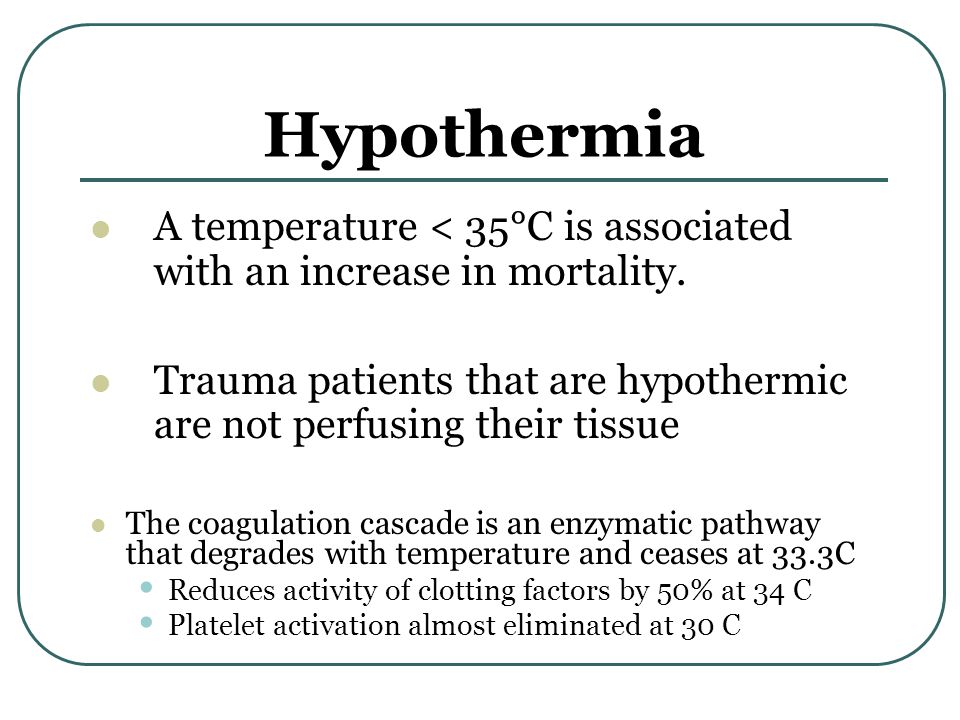
Hypothermia A temperature < 35°C is associated with an increase in mortality. Trauma patients that are hypothermic are not perfusing their tissue The coagulation cascade is an enzymatic pathway that degrades with temperature and ceases at 33.3C Reduces activity of clotting factors by 50% at 34 C Platelet activation almost eliminated at 30 C

22
Acidosis Base deficit (BD) ≥ 6 identifies patients that require early transfusion, increased ICU days and risk for ARDS and MOF BD of ≥ 6 is strongly associated with the need for MT and mortality. Patients have an elevated BD before their blood pressure drops to classic “hypotension” levels. Acidosis contributes more to coagulopathy more than hypothermia (not reversible)
.")
23
The best Policy of Management: Damage Control Resuscitation

24
Definition ‘systematic approach to major trauma combining the catastrophic bleeding, airway, breathing and circulation ( ABC) paradigm with a series of clinical techniques from point of wounding to definitive treatment in order to minimize blood loss, maximize tissue oxygenation and optimize outcome’. (Hodgetts et al., 2007).
..")
25
Inclusion criteria for DCR Rapid pattern recognition Severe Traumatic Injury Abnormal mental status Weak or absent radial pulse Acidosis- Base Deficit > - 6 Coagulopathy – INR > 1.5 Hypotension – Systolic B/P < 90 Hemoglobin - < 11 Temperature - < 35°C

26
Armamentarium of Damage control resuscitation Permissive hypotension Hemostatic Resuscitation

27
Armamentarium of Damage control resuscitation Permissive hypotension Hemostatic Resuscitation

28
Permissive hypotension

29
The concept behind permissive hypotension involves keeping the blood pressure low enough to avoid exsanguination while maintaining perfusion of end organs. However, the concept of permissive hypotension represents a double-edged sword, since a prolonged duration of shock may further aggravate the extent of post-injury coagulopathy.

30
Armamentarium of Damage control resuscitation Permissive hypotension Hemostatic Resuscitation

31
Haemostatic resuscitation aims to restore tissue perfusion and arrest coagulopathy using a combination of blood products and adjuncts early in the resuscitation process (Hodgetts et al., 2007).
.")
32
Aspects of hemostatic resuscitation Minimizing use of crystalloids Early transfusion of RBC (fresh): plasma: PLTs in an optimum ratio Use of thawed plasma and Fresh Whole Blood (when available) Early prevention of hypothermia, acidosis Appropriate use of rFVIIa and fibrinogen containing products such as cryoprecipitate Use POC coagulation assays such as rapid thromboelastography (rTEG) to guide administration of blood products and hemostatic adjuncts Rapid definitive control of bleeding
: plasma: PLTs in an optimum ratio Use of thawed plasma and Fresh Whole Blood (when available) Early prevention of hypothermia, acidosis Appropriate use of rFVIIa and fibrinogen containing products such as cryoprecipitate Use POC coagulation assays such as rapid thromboelastography (rTEG) to guide administration of blood products and hemostatic adjuncts Rapid definitive control of bleeding")
33
Thawed Plasma Thawed plasma should be used as a primary resuscitative fluid. This product should be present upon arrival of the casualty in the ED This approach not only addresses the metabolic abnormality of shock, but initiates reversal of the coagulopathy present.

34
What is the optimal ratio of blood products ?

36
Figure 1. Plasma:RBC product transfusion ratios effect on patient survival. (A) Survival versus ratio. () 24-hour survival; () 30-day survival. (B) Patient characteristics in each ratio group. (C) Patient outcome and characteristics in high (one or more plasma per two RBC products) versus low (less than one plasma per two RBC products) transfusion group. Ave = average.
 Survival versus ratio. () 24-hour survival; () 30-day survival. (B) Patient characteristics in each ratio group. (C) Patient outcome and characteristics in high (one or more plasma per two RBC products) versus low (less than one plasma per two RBC products) transfusion group. Ave = average..")
37
Figure 2. PLT-to-RBC product transfusion ratios effects on patient survival. (A) Survival versus ratio. () 24-hour survival; () 30-day survival. (B) Patient characteristics in each ratio group. (C) Patient outcome and characteristics in high (one or more apheresis PLTs per 20 RBC products) versus low (less than one apheresis PLTs per 20 RBC products) transfusion group. Ave = average.
 Survival versus ratio. () 24-hour survival; () 30-day survival. (B) Patient characteristics in each ratio group. (C) Patient outcome and characteristics in high (one or more apheresis PLTs per 20 RBC products) versus low (less than one apheresis PLTs per 20 RBC products) transfusion group. Ave = average..")
38
Figure 3. Cryoprecipitate-to-RBC product transfusion ratios effects on patient survival. (A) Survival versus ratio. () 24-hour survival; () 30-day survival. (B) Patient characteristics in each ratio group. (C) Patient outcome and characteristics in high (one or more unit of cryoprecipitate per two RBC products) versus low (less than 1 unit of cryoprecipitate per two RBC products) transfusion group. Ave = average.
 Survival versus ratio. () 24-hour survival; () 30-day survival. (B) Patient characteristics in each ratio group. (C) Patient outcome and characteristics in high (one or more unit of cryoprecipitate per two RBC products) versus low (less than 1 unit of cryoprecipitate per two RBC products) transfusion group. Ave = average..")
39
Figure 4. Survival curves for the eight groups: 1) high plasma, high PLT, high cryoprecipitate (n = 50); 2) high plasma, high PLT, low cryoprecipitate (n = 28); 3) high plasma, low PLT, low cryoprecipitate (n = 12); 4) high plasma, low PLT, high cryoprecipitate (n = 10); 5) low plasma, high PLT, high cryoprecipitate (n = 21); 6) low plasma, high PLT, low cryoprecipitate (n = 27); 7) low plasma, low PLT, high cryoprecipitate (n = 6); and 8) low plasma, low PLT, low cryoprecipitate(n = 60). High versus low ratio groups determined as a ratio of 0.5 or more versus less than 0.5. CR = cryoprecipitate; PL = plasma; PT = PLT.
 high plasma, high PLT, high cryoprecipitate (n = 50); 2) high plasma, high PLT, low cryoprecipitate (n = 28); 3) high plasma, low PLT, low cryoprecipitate (n = 12); 4) high plasma, low PLT, high cryoprecipitate (n = 10); 5) low plasma, high PLT, high cryoprecipitate (n = 21); 6) low plasma, high PLT, low cryoprecipitate (n = 27); 7) low plasma, low PLT, high cryoprecipitate (n = 6); and 8) low plasma, low PLT, low cryoprecipitate(n = 60). High versus low ratio groups determined as a ratio of 0.5 or more versus less than 0.5. CR = cryoprecipitate; PL = plasma; PT = PLT..")
40
Component Therapy Vs Fresh Whole Blood in trauma patients

41
PRBC Hct 55% 335 mL Plt 5.5x10 10 50 mL FFP 80% 275 mL So Component Therapy Gives You 1U PRBC + 1U PLT + 1U FFP 660 mL 660 COLD mL Hct 29% Plt 87K Coag activity 65% 750 mg fibrinogen Armand & Hess, Transfusion Med. Rev., 2003 500 mL Warm Hct: 38-50% Hct: 38-50% Plt: 150-400K Plt: 150-400K Coags: 100% Coags: 100% 1500 mg Fibrinogen Dilution is inevitable with component therapy

42
Fresh Whole Blood Fresh whole blood (FWB) must be called for early after ED arrival FWB is the optimal resuscitation fluid for severely injured casualties. FWB is the best fluid for hypotensive resuscitation for hemorrhagic shock.

43
Recombinant factor VIIa as a rescue therapy

44
Mechanism of action of rFVIIa rFVIIa works locally at the site of vascular injury, where tissue factor (TF) is exposed and activated platelets are found 1 Binding of factor VIIa or rFVIIa to TF initiates the coagulation generating small amounts of thrombin 2 At pharmacological doses rFVIIa directly activates factor X on the surface of activated platelets resulting in a “thrombin burst” 3,4 The thrombin burst leads to the formation of a stable haemostatic plug which controls the bleeding 3
 is exposed and activated platelets are found 1 Binding of factor VIIa or rFVIIa to TF initiates the coagulation generating small amounts of thrombin 2 At pharmacological doses rFVIIa directly activates factor X on the surface of activated platelets resulting in a thrombin burst 3,4 The thrombin burst leads to the formation of a stable haemostatic plug which controls the bleeding 3 ")
46
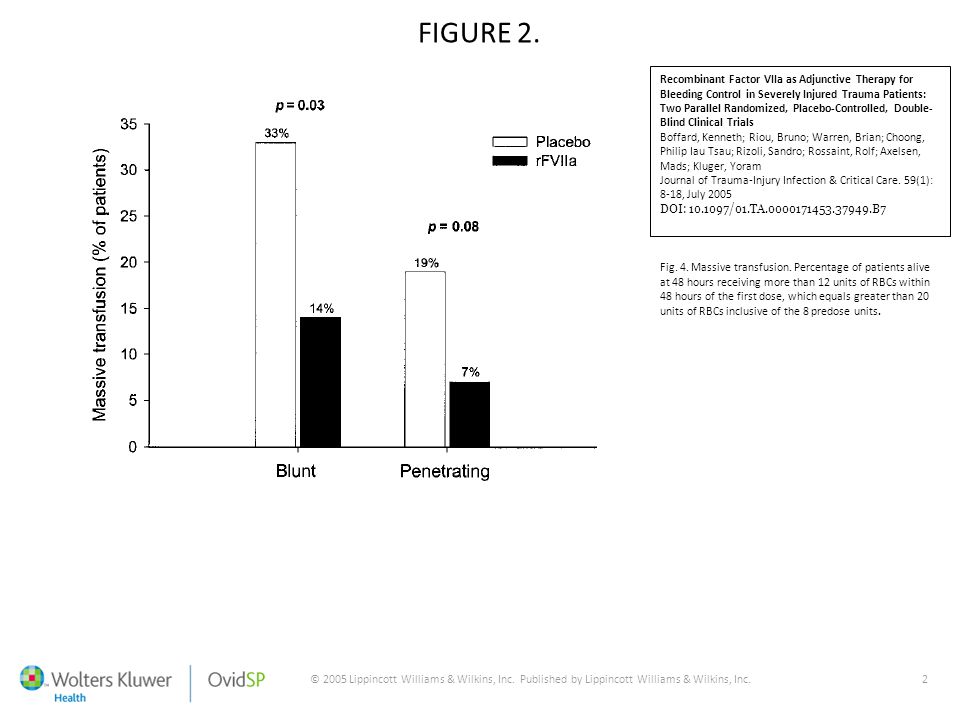
© 2005 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.2 FIGURE 2. Recombinant Factor VIIa as Adjunctive Therapy for Bleeding Control in Severely Injured Trauma Patients: Two Parallel Randomized, Placebo-Controlled, Double- Blind Clinical Trials Boffard, Kenneth; Riou, Bruno; Warren, Brian; Choong, Philip Iau Tsau; Rizoli, Sandro; Rossaint, Rolf; Axelsen, Mads; Kluger, Yoram Journal of Trauma-Injury Infection & Critical Care. 59(1): 8-18, July 2005 DOI: 10.1097/01.TA.0000171453.37949.B7 Fig. 4. Massive transfusion. Percentage of patients alive at 48 hours receiving more than 12 units of RBCs within 48 hours of the first dose, which equals greater than 20 units of RBCs inclusive of the 8 predose units.
: 8-18, July 2005 DOI: /01.TA B7 Fig. 4. Massive transfusion. Percentage of patients alive at 48 hours receiving more than 12 units of RBCs within 48 hours of the first dose, which equals greater than 20 units of RBCs inclusive of the 8 predose units..")
47
© 2005 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.2 FIGURE 2. Recombinant Factor VIIa as Adjunctive Therapy for Bleeding Control in Severely Injured Trauma Patients: Two Parallel Randomized, Placebo-Controlled, Double- Blind Clinical Trials Boffard, Kenneth; Riou, Bruno; Warren, Brian; Choong, Philip Iau Tsau; Rizoli, Sandro; Rossaint, Rolf; Axelsen, Mads; Kluger, Yoram Journal of Trauma-Injury Infection & Critical Care. 59(1): 8-18, July 2005 DOI: 10.1097/01.TA.0000171453.37949.B7 Fig. 4. Survival curves for blunt and penetrating trauma populations. The difference between treatment groups was not significant (log-rank test, not significant).
: 8-18, July 2005 DOI: /01.TA B7 Fig. 4. Survival curves for blunt and penetrating trauma populations. The difference between treatment groups was not significant (log-rank test, not significant)..")
48
Recombinant factor VIIa This benefit was not seen in patients with penetrating trauma in the single randomized controlled trial published to date. rFVIIa increases the SBP at which arterial rebleeding occurs suggesting the formation of a tighter, stronger fibrin plug in the presence of high concentrations of rFVIIa Risk of thomboembolic events ?? Dosing guidelines for hemorrhage (general range, 90-120 mcg/kg of body weight) have yet to be established Cost of rFVIIa is over $3000 / patient
 have yet to be established Cost of rFVIIa is over $3000 / patient.")
49
Recombinant factor VIIa Current evidence indicates that factor VIIa (recombinant) reduces RBC requirements in patients with blunt traumatic hemorrhage. This benefit was not seen in patients with penetrating trauma in the single randomized controlled trial published to date. The effect of factor VIIa (recombinant) on mortality is unknown and is the subject of ongoing investigation. The use of factor VIIa (recombinant) should be considered only after the optimization of blood component administration and surgical intervention, when appropriate.
 on mortality is unknown and is the subject of ongoing investigation. The use of factor VIIa (recombinant) should be considered only after the optimization of blood component administration and surgical intervention, when appropriate..")
50
Guideline for Recombinant factor VIIa in Trauma Patients J. Thromb Haemost 2005; 3: 640-8 Massive bleeding: Loss of entire blood volume in 24h (10 U PRBC in 70kg) Loss of 50% blood in 3h Blood loss rate 150mL/min Blood loss rate 1.5mL/kg for over 20 min Failure to arrest hemorrhage despite: FFP: 10-15mL/kg (4-6U for 70kg) Cryo: 1-2U/10kg (10-15U for 70kg) Platelets: 1-2U/10kg (10-15U for 70kg) Correction of acidosis: pH= 7.2 Warming of hypothermic patients (recommended, not mandatory for rFVIIa)
 Loss of 50% blood in 3h Blood loss rate 150mL/min Blood loss rate 1.5mL/kg for over 20 min Failure to arrest hemorrhage despite: FFP: 10-15mL/kg (4-6U for 70kg) Cryo: 1-2U/10kg (10-15U for 70kg) Platelets: 1-2U/10kg (10-15U for 70kg) Correction of acidosis: pH= 7.2 Warming of hypothermic patients (recommended, not mandatory for rFVIIa).")
51
Guideline for Recombinant factor VIIa in Trauma Patients J. Thromb Haemost 2005; 3: 640-8 Preconditions Fibrinogen 50 mg/dL (100 mg/dL preferred) Platelet 50000*10 9 /L (100000 *10 9 /L preferred) pH 7.2 Treatment Initial 100~140 (120) ug/kg IV bolus, 15 to 20 min repeat 100 ug/kg IV Total dose > 200 ug/kg, check and correct preconditions. If correction not feasible, FFP 10-15mL/kg or 4-6 U/70kg Cryo 1-2 U/10kg or 10-15 U/70kg Platelet 1-2 U/10kg or 10-15 U/70kg Correct pH and calcium Third dose 100 ug/kg IV
 Platelet 50000*10 9 /L ( *10 9 /L preferred) pH 7.2 Treatment Initial 100~140 (120) ug/kg IV bolus, 15 to 20 min repeat 100 ug/kg IV Total dose > 200 ug/kg, check and correct preconditions. If correction not feasible, FFP 10-15mL/kg or 4-6 U/70kg Cryo 1-2 U/10kg or U/70kg Platelet 1-2 U/10kg or U/70kg Correct pH and calcium Third dose 100 ug/kg IV.")
52
“Our own blood is still the best thing to have in our veins” – Frenzel et al., 2008

53
Thank you

Similar presentations















-Score: Probability of Mass Transfusion as Surrogate for Life Threatening Hemorrhage after Multiple Trauma The.>")












