Download presentation
Presentation is loading. Please wait.

2
OHSS is a serious, potentially life- threatening, iatrogenic complication of “controlled” ovarian stimulation. To optimize the ovarian response without provoking OHSS is the best compromise that should be reached by an ideal regimen of stimulation, which is unfortunately still not consistently achievable.

3
PCO-like ovarian ultrasound features (more than 10 follicles) are a predictive factor for OHSS in IVF. Increased risk for OHSS in patients with a LH/FSH ratio of more than 2. The incidence of OHSS in PCOS patients is 6% Tibi, 1989 Delvigne, Human Reprod 1993 Brinsden, Br J Obstet Gynecol 1995

4
Clomiphen citrate Nonstimulated – natural cycle Low dose gonadotropin protocols › Agonist › Antagonist Trigger the ovulation Luteal phase support Metformin IVM Coasting

5
Patients with PCOS are unlikely to benefit from this procedure since their success in development of a single follicle leading to the retrieval of a single, good quality oocyte during a spontaneous cycle remains uncertain.

6
Ovulation is restored in 80%, but pregnancy is achieved in 35% of patients 75% of the pregnancies occur within the first three cycles of CC treatment 20-25% of PCOS patients remain resistant to CC CC is rarely associated with severe OHSS Imani, Fertil Steril 2002 Gysler, Fertil Steril 1982 Kistner, Obstet Gynecol Surv 1965

7
Two reviews from The Cochrane Library on clinical trials investigating gonadotropin therapy for ovulation induction in women with clomipheneresistant PCOS, concluded that no significant benefit could be demonstrated from urinary FSH versus hMG in terms of pregnancy rate, but a significant reduction in OHSS associated with FSH was observed. Hughes 1997, Nugent 2002

8
Early reports suggested a relationship between the type of gonadotropin preparation utilized and the risk of OHSS. More recent comparisons between recombinant follicle-stimulating hormone (rFSH) and human menopausal gonadotropins (hMG) did not show significant differences among variable drug regimens.
 and human menopausal gonadotropins (hMG) did not show significant differences among variable drug regimens..")
9
The clinical pregnancy rates per cycle started were higher with rFSH than uFSH, although the magnitude of the observed difference was small, 3.7%. No significant differences were detected in the rates of miscarriage, multiple pregnancy and OHSS. European and Middle East Orgalutran Study Group, Human Reprod 2001

10
During cycles without GnRH-a suppression, either a significant LH surge or at least marked luteinization will limit continued gonadotropin stimulation and thus lead to a concomitantly lower risk of OHSS.

11
FIVNAT results showed that the use of GnRH-a led to significantly higher preovulatory estradiol concentrations, and to more frequent severe hyperstimulation (4.6% vs. 0.6% for nonGnRH-a/hMG cycles). FIVNAT, Contracept Fertil Sex 1989
. FIVNAT, Contracept Fertil Sex")
12
The type of GnRH agonist to be used in patients at risk of OHSS has not been extensively studied. It is obvious that the short protocol should not be proposed, as the initial flare-up effect could lead to an excessive ovarian response. In the long protocol, depot formulation versus daily injection and follicular versus luteal start have not been compared prospectively in patients at risk of OHSS.

13
It has been proposed that a longer period of desensitization (30 instead of 15 days) is of benefit by reducing androgen levels. The longer duration of treatment did not improve pregnancy rates but did apparently decrease the incidence of hyperstimulation. Salat-Baroux, Human Reprod 1988

14
Patients receiving antagonist treatment have lower estradiol serum levels at the time of hCG administration, mostly because of a lower number of follicles, which could explain the lower incidence of OHSS. Ludwig M, Arch Gynecol Obstet 2000

15
There was a statistically significant reduction in incidence of severe OHSS with antagonist protocol. The relative risk ratio was 0.61 (P=0.01; 95% CI 0.42 - 0.89). In addition, interventions to prevent OHSS (e.g. coasting, cycle cancellation) were administered more frequently in the agonist group (P=0.03; OR 0.44, 95% CI 0.21 - 0.93). Al-Inany, Cochrane Database 2006
. In addition, interventions to prevent OHSS (e.g. coasting, cycle cancellation) were administered more frequently in the agonist group (P=0.03; OR 0.44, 95% CI ). Al-Inany, Cochrane Database")
16
The GnRH-antagonist protocol involved starting gonadotropins on day 3 of the menstrual cycle. Transvaginal ultrasound monitoring was commenced on day 5 of ovarian stimulation and repeated every 2-3 days.

17
150 IU 225 IU 3th day 7th day USG 300 IU USG 12th day HCG Antagonist (start at 6th day)
")
18
The starting dose for gonadotropin is based on › age, › body mass index (BMI) › existence of PCOS, › previous history of OHSS or high response.
 › existence of PCOS, › previous history of OHSS or high response.")
19
Two comparative prospective studies of the conventional regimen, with the chronic low-dose step-up protocol using urinary FSH or rhFSH for ovulation induction in PCOS patients, showed that the low-dose approach eliminated complications of OHSS and multiple pregnancies without jeopardizing the incidence of pregnancy. Homburg, Fertil Steril 1995 Hedon, Human Reprod 1998

20
150 IU 225 IU 3th day 7th day USG 300 IU USG 12th day HCG Agonist Mid luteal

21
75 IU 150 IU 3th day 7th day USG HCG Agonist Mid luteal

22
75 IU 3th day 14th day USG 112.5 IU 150 IU 21st day USG

23
The step-down protocol applies decremental doses of gonadotropins once ovarian response is established, but the starting dose is higher than in the step-up approach. Monitoring of follicular growth is, however, more stringent than with the step-up approach. In addition, the long half-life of currently available FSH preparations makes it difficult to judge the correct reduction of dose. Clinical results are similar to those obtained with the step-up approach. van Santbrink, Human Reprod 1995

24
Agonist 3th day 6th day USG 150 IU 300 IU HCG Mid luteal

25
Unlike a step-up protocol, which continuously rescues follicles from atresia, a step-down protocol will allow more follicles to undergo atresia, thus reducing the overall number of follicles capable of secretory activity by the time hCG is administered.

26
An alternative method for ovulation induction with FSH in PCOS patients is the so-called sequential protocol, which combines an initial step-up gonadotropin administration followed by a step-down regimen after follicular selection (leading follicle > 14 mm). In a comparative study with the standard low-dose step-up regimen, both approaches were shown to be safe and effective. Hugues, Human Reprod 1996

27
More recently, Filicori et al. proposed conducting the end of stimulation using a treatment composed of low-dose hCG. Low-dose hCG as a source of LH activity was associated with FSH or was used alone in the second part of the follicular phase. Filicori, Human Reprod Update 2002

28
Ovarian stimulation with daily late follicular phase administration of low-dose human chorionic gonadotropin for in vitro fertilization: a prospective, randomised trial Serafini, et al, Fertil Steril 2006

29
Ovarian stimulation with daily late follicular phase administration of low-dose human chorionic gonadotropin for in vitro fertilization: a prospective, randomised trial Serafini, et al, Fertil Steril 2006

30
Use a combination of frequent serum estradiol measurements and ultrasonographic assessments of follicular growth.

31
Decrease in hCG dose › 10.000 IU vs. 5.000 IU or 3.000 IU no difference The use of GnRH antagonists could further decrease the incidence of OHSS in high-risk patients when replacing hCG by a GnRH agonist to trigger ovulation. A recent prospective study found a lower pregnancy rate in patients in whom GnRH agonists were used to trigger ovulation.

32
There was no statistically significant difference between rhCG vs uhCG regarding the incidence of OHSS. A multicenter double-blind study revealed that new recombinant human LH can be as effective as hCG in inducing the final follicular maturation in IVF treatment with a lower incidence of OHSS. European Recombinant LH Study Group 2001 Al-Inany, Cochrane Database 2005

33
The odds of OHSS were more than 2-fold higher with treatments involving hCG than with progesterone alone (OR 3.06, 95% CI 1.59 to 5.86). Comparing routes of progesterone administration, reductions in clinical pregnancy rate with the oral route, compared to the intramuscular or vaginal routes, did not reach statistical significance, but there was evidence of benefit of the intramuscular over the vaginal route for the outcomes of ongoing pregnancy and live birth. Daya, Gunby, Cochrane Database 2004

34
Due to the abundance of follicles in the ovary, PCOS patients present an excellent clinical opportunity for the retrieval of unstimulated immature eggs and do In Vitro Maturation.

35
The immature oocytes are retrieved from antral follicles of unstimulated (or minimally stimulated) ovaries via the transvaginal approach. The oocytes are subsequently matured in vitro in a special formulated culture medium for 24-48 h. The mature oocytes are fertilized, usually by intracytoplasmic sperm injection (ICSI), and the selected embryos are transferred to the uterus 2-3 days later.
, and the selected embryos are transferred to the uterus 2-3 days later..")
36
Because no expensive gonadotropin stimulation and no extensive monitoring scans are required, the cost of IVM treatment is lower than that of IVF. The IVM treatment schedule is shorter, causing less stress, and it is not necessary to wait for 2 to 3 months between treatment cycles because no stimulation is involved. The risk of OHSS can be avoided by IVM treatment, especially in women with PCO/PCOS. Child, Obstet Gynecol 2002

37
ART ServiceParisMontrealTaipeiHelsinkiSeoul Cycles (n)13825468239203419 Oocytes retrieved 12.111.922.58.015.516.4 Maturation rate (%) 61.778.874.258.655.373.2 Fertilization rate (%) 6269.272.851.375.179.0 Transferred embryo 2.43.43.85.04.3 Clinical Pregnancy rate(%) 24.524.033.826.621.932.7 Tan SL, et al. In vitro Maturation of Human Oocytes, 2007

38
Clinical pregnancy rate 35% per cycle Implantation rate 15% per embryo Al-Sunaidi, Fertil Steril 2007

39
Metformin has been studied and mostly shown to restore menstrual cycles and confirm ovulation in anywhere between 25 - 90% of cases. A recent analysis of 13 randomized controlled trials showed that metformin increased the ovulation rate almost four times compared to placebo when it was administered in combination with clomiphene citrate.

40
No metformin (n=159)Metformin (n=128) Age34.833 BMI27.227.8 HMG ampoules37.141.1 Oocytes retrieved23.818.8 Embryos tranferred2.83 Clinical pregnancies37.630.5 Moderate and severe OHSS*201 Khattab, Reprod Biomed Online, 2006
Metformin (n=128) Age BMI HMG ampoules Oocytes retrieved Embryos tranferred2.83 Clinical pregnancies Moderate and severe OHSS*201 Khattab, Reprod Biomed Online, 2006")
41
Metformin (n=52)Placebo (n=49) Cancellation %9.64.1 Nr of eggs17.316.2 Nr of embryos transferred22 Clinical preg rate %38.516.3* Live birth rate %32.712.2* Severe OHSS %3.820.4* Tang, Human Reprod, 2006 * p< 0.05
Placebo (n=49) Cancellation % Nr of eggs Nr of embryos transferred22 Clinical preg rate % * Live birth rate % * Severe OHSS % * Tang, Human Reprod, 2006 * p< 0.05")
42
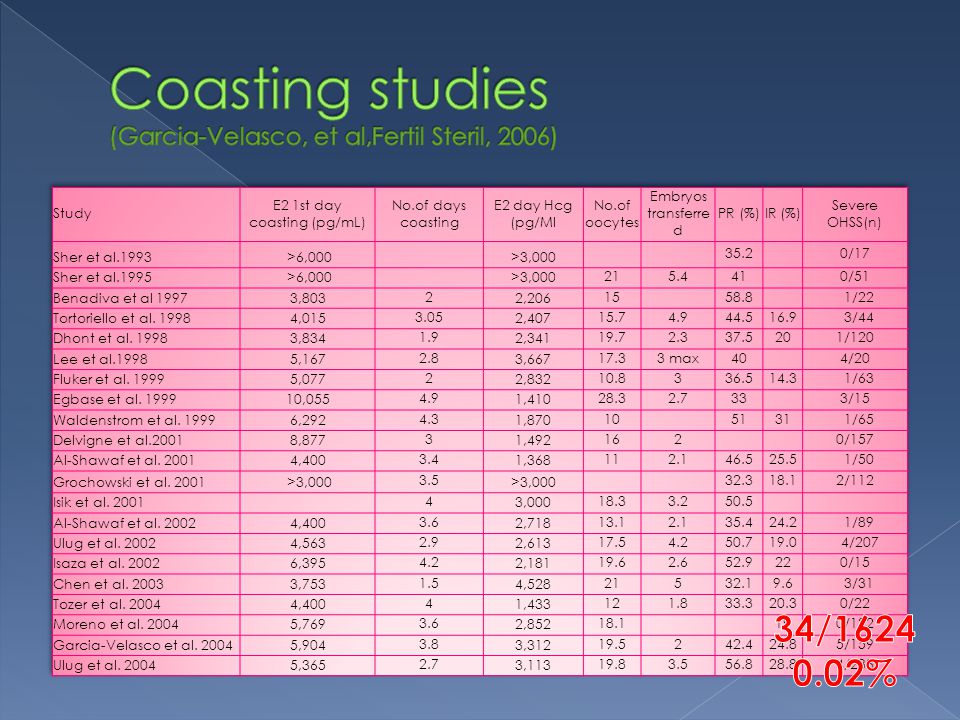
First described and applied by Sher et al in 1993 hCG administration postponed until the patients serum E2 level decreases to a safer zone. E2 levels usually rise rapidly in the 48 h following initiation of the coasting period, then plateaued and began to fall 96-168 h after the gonadotropins were stopped.

43
Cochrane review identified 13 studies of which only one trial met the inclusion criteria. There was no difference in the incidence of moderate and severe OHSS and in the clinical pregnancy rate between the groups. D’Angelo et al., Cochrane Library, 2002

44
A recent review of ten studies showed that < 2% of women developed OHSS while maintaining acceptable pregnancy rates (36.5-63%) when coasting was continued until serum estradiol levels fell below 3000 pg/ml. Levinson-Tavor, Human Reprod 2003

46
Coasting < 4 days (n=983) Coasting >4 days (n=240) Age30.229.9 Oocytes retrieved*16.514.9 Mean no of embryos trans2.993.03 Clin pregnancy rate*52.035.9 Implantation rate*26.318.2 Mansour, et al., Fertil Steril, 2005
 Coasting >4 days (n=240) Age Oocytes retrieved* Mean no of embryos trans Clin pregnancy rate* Implantation rate* Mansour, et al., Fertil Steril, 2005")
47
Coasting is a good alternative that can avoid cycle cancellation in high responders, who have high risk of developing severe OHSS Even if OHSS develops after coasting both its incidence and severity will be diminished

48
No one gonadotropin is superior to others for reducing the incidence of OHSS Antagonist-low dose step up is the best protocol available Monitoring of the E2 and USG of follicles is crucial Luteal phase support with hCG increases the incidence of OHSS. Progesterone intravaginally or i.m. should be used for the patients at risk of OHSS

49
IVM is a novel method and must be developed for better results Coasting is an effective method for preventing severe OHSS No method has been developed that will completely prevent severe OHSS after ovarian stimulation.

50
r FSHu FSH Bergh, Hum Reprod 19975.11.7 Out, Hum Reprod 19953.22.0

Similar presentations











 Is It Safe? Mustafa Uğur Zekai Tahir Burak Women’s Health Education and Research Hospital, Ankara, Turkey.>")
 produced.>")


 Director, IVF Center, HKSH Specialist.>")


 6.6.6 Discuss the ethical issues associated.>")

