Download presentation
1
Capillary rethink time Andrew Magnay University Hospital of North Staffordshire NHS Trust NHS Trust

2
Introduction Resuscitation of the critically ill or injured child is an APLS/PHPLS (&ATLS/PHTLS) “standard scenario”, tested in the *PLS courses The method emphasises the approach of “as one identifies a critical problem, so one treats or enables its treatment” The purpose: Prevent progression of illness whilst enabling definitive care Purpose achieved by ABCDE
 standard scenario , tested in the *PLS courses The method emphasises the approach of as one identifies a critical problem, so one treats or enables its treatment The purpose: Prevent progression of illness whilst enabling definitive care Purpose achieved by ABCDE")
3
Agenda Use & abuse of CRT - an indirect clinical assessment tool Dehydration vs. Hypovolaemia Consequences of too much fluid? –Trauma and cautiously hypovolaemic resus n –Special problems: Meningitis / raised ICP Cardiogenic shock & other non-hypovolaemic shock ARDS Infancy

4
Recognition of the ill child A,B APLS & ATLS GIVE OXYGEN ASSESS –A –Airway patent? –B –Breathing Rate Normal Values APLSATLS 7 th Ed < 1yr <40 <60 1 - 2yr <35 <40 1 - 2yr <35 <40 2 – 5yr <30 <35 2 – 5yr <30 <35 5-12yr <25 <30 5-12yr <25 <30 >12yr 12yr <20 <30 –Accessory resps, colour & consciousness

5
Recognition of the ill child C APLS & ATLS OXYGEN ASSESS –Pulse rate Normal Values <1yr < 160 1 - 5yr < 140 5 - 12yr < 120 >12 yr< 100 Capillary refill –Colour, Capillary refill, Coolness, Exsanguinating haemorrhage –Consciousness (under-perfusion)
")
6
Circulation Restoration of volume ATLS APLS (or 10+10ml/kg) CRYSTALLOID / COLLOID 20 ml/kg (or 10+10ml/kg) BLOODBLOOD SURGERY IF TRAUMA Assess response C CRYSTALLOID / COLLOID 20 ml/kg Consider FFP, Cryo etc Assess response
 CRYSTALLOID / COLLOID 20 ml/kg (or 10+10ml/kg) BLOODBLOOD SURGERY IF TRAUMA Assess response C CRYSTALLOID / COLLOID 20 ml/kg Consider FFP, Cryo etc Assess response")
7
Case Illustration A.1 12 yr boy, fall from tree 14 ft onto rough. Adm. A&E, facial injury no stridor or blood Resp 18 /min, normal air entry Bruising over lower left chest HR 134, CRT 4 sec, BP 80/50 GCS 9 (E2,V2,M5), PERL, Neuro L=R
, PERL, Neuro L=R.")
8
Case Illustration A.1 12 yr boy, fall from tree 14 ft onto rough. Adm. A&E, facial injury no stridor or blood Resp 18 /min, normal air entry Bruising over lower left chest HR 134, CRT 4 sec, BP 80/50 GCS 9 (E2,V2,M5), PERL, Neuro L=R 20ml/kg Saline HR 130 CRT 4 BP 85/45 20ml/kg Saline HR 126 CRT 4 BP 88/50 +Surg n
, PERL, Neuro L=R 20ml/kg Saline HR 130 CRT 4 BP 85/45 20ml/kg Saline HR 126 CRT 4 BP 88/50 +Surg n.")
9
Case Illustration A.1 12 yr boy, fall from tree 14 ft onto rough. Adm. A&E, facial injury no stridor or blood Resp 18 /min, normal air entry Bruising over lower left chest HR 134, CRT 4 sec, BP 80/50 GCS 9 (E2,V2,M5), PERL, Neuro L=R 20ml/kg Saline HR 130 CRT 4 BP 85/45 20ml/kg Saline HR 126 CRT 4 BP 88/50 +Surg n Blood HR 124 CRT 4 BP 88/50
, PERL, Neuro L=R 20ml/kg Saline HR 130 CRT 4 BP 85/45 20ml/kg Saline HR 126 CRT 4 BP 88/50 +Surg n Blood HR 124 CRT 4 BP 88/50.")
10
Case Illustration A.1 12 yr boy, fall from tree 14 ft onto rough. Adm. A&E, facial injury no stridor or blood Resp 18 /min, normal air entry Bruising over lower left chest HR 134, CRT 4 sec, BP 80/50 GCS 9 (E2,V2,M5), PERL, Neuro L=R 20ml/kg Saline HR 130 CRT 4 BP 85/45 20ml/kg Saline HR 126 CRT 4 BP 88/50 +Surg n Blood HR 124 CRT 4 BP 88/50 GCS=14 (E4,V3,M6) Splenectomy
, PERL, Neuro L=R 20ml/kg Saline HR 130 CRT 4 BP 85/45 20ml/kg Saline HR 126 CRT 4 BP 88/50 +Surg n Blood HR 124 CRT 4 BP 88/50 GCS=14 (E4,V3,M6) Splenectomy.")
11
Case Illustration A.1 12 yr boy, fall from tree 14 ft onto rough. Adm. A&E, facial injury no stridor or blood Resp 18 /min, normal air entry Bruising over lower left chest HR 134, CRT 3 sec, BP 80/50 GCS 9 (E2,V2,M5), PERL, Neuro L=R CRT 4 20ml/kg Saline HR 130 CRT 4 BP 85/45 CRT 4 20ml/kg Saline HR 126 CRT 4 BP 88/50 CRT 4 Blood HR 124 CRT 4 BP 88/50 GCS=14 (E4,V3,M6) Splenectomy Suppose his temp was 35 6 C on arrival to O.R.? Suppose his temp was 35 6 C on arrival to O.R.?
, PERL, Neuro L=R CRT 4 20ml/kg Saline HR 130 CRT 4 BP 85/45 CRT 4 20ml/kg Saline HR 126 CRT 4 BP 88/50 CRT 4 Blood HR 124 CRT 4 BP 88/50 GCS=14 (E4,V3,M6) Splenectomy Suppose his temp was 35 6 C on arrival to O.R.. Suppose his temp was 35 6 C on arrival to O.R. .")
12
Case Illustration A.2 12 yr boy, fall from tree 14 ft onto rough. Adm. A&E, facial injury no stridor or blood Resp 18 /min, normal air entry Bruising over lower left chest HR 68, CRT 4 sec, BP 120/76 GCS 9 (E2,V2, M5), PERL, Neuro L=R
, PERL, Neuro L=R.")
13
Case Illustration A.2 12 yr boy, fall from tree 14 ft onto rough. Adm. A&E, facial injury no stridor or blood Resp 18 /min, normal air entry Bruising over lower left chest HR 68, CRT 4 sec, BP 120/76 GCS 9 (E2,V2, M5), PERL, Neuro L=R 2 IVI, Maintenance N/Saline only; CT Scan, neurosurgical opinion
, PERL, Neuro L=R 2 IVI, Maintenance N/Saline only; CT Scan, neurosurgical opinion.")
14
Case Illustration B.1 2yr girl, 48hr temp, lethargy, vomited x1 2hr petechial rash Admitted to A&E by GP (gave penicillin) Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7
 Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7")
15
Case Illustration B.1 2yr girl, 48hr temp, lethargy, vomited x1 2hr petechial rash Admitted to A&E by GP (gave penicillin) Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7
 Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7")
16
Case Illustration B.1 2yr girl, 48hr temp, lethargy, vomited x1 2hr petechial rash Admitted to A&E by GP (gave penicillin) Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7 Rx O 2, 2 x 20ml Resuscitation fluid, BM=7 HR 175, CRT 4 sec, BP 70/35, RR 56, Sats 93% Still shocked, developing pulmonary oedema
 Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7 Rx O 2, 2 x 20ml Resuscitation fluid, BM=7 HR 175, CRT 4 sec, BP 70/35, RR 56, Sats 93% Still shocked, developing pulmonary oedema")
17
Case Illustration B.1 2yr girl, 48hr temp, lethargy, vomited x1 2hr petechial rash Admitted to A&E by GP (gave penicillin) Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7 Rx O 2, 2 x 20ml Resuscitation fluid, BM=7 HR 175, CRT 4 sec, BP 70/35, RR 56, Sats 93% Still shocked, developing pulmonary oedema
 Spontaneously breathing, RR50, Sats 98% (air) HR 180, CRT 4 sec, BP 65/30, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7 Rx O 2, 2 x 20ml Resuscitation fluid, BM=7 HR 175, CRT 4 sec, BP 70/35, RR 56, Sats 93% Still shocked, developing pulmonary oedema")
18
Case Illustration B.2 2yr girl, 48hr temp, lethargy, vomited x1 2hr petechial rash Admitted to A&E by GP (gave penicillin) Spontaneously breathing, RR50, Sats 98% (air) HR 110, CRT 4 sec, BP 100/70, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7
 Spontaneously breathing, RR50, Sats 98% (air) HR 110, CRT 4 sec, BP 100/70, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7")
19
Case Illustration B.2 2yr girl, 48hr temp, lethargy, vomited x1 2hr petechial rash Admitted to A&E by GP (gave penicillin) Spontaneously breathing, RR50, Sats 98% (air) HR 110, CRT 4 sec, BP 100/70, Temp 38 6 C Opens eyes to pain, E2 V1 M4 = 7; BM 7.5 2xIVI, N/Saline maintenance only. Sats 98%. Reduced conscious level due to…?

20
Connections Decision to correct fluid deficit is a “gestalt” NOT a “one-test-solves-all” Is the child ill? Potentially ill? Context? Is there a reason for extreme caution? –Cerebral oedema, cardiac, infancy? intravascular hypovolaemia Does the overall story with physical signs indicate intravascular hypovolaemia? dehydration Does the overall story with physical signs indicate dehydration?

21
Capillary Refill Time Uses and abuses Is it: –“reliable” (technique, IUV, environment)? predictor –A predictor of hypovolaemic shock? predictor –A predictor of anything useful? negative predictor –Useful as a negative predictor? Is it used canonically by APLS providers? Is it used canonically by APLS instructors?

22
Some kind of shock A true story 14 yr boy c/o faintness, breathlessness HR 190, BP 80/40, weak pulse, CRT 5sec Rx 20ml/kg. No effect Rx 20ml/kg. C/o chest pain, can’t breathe …..?! ECG, diuretic, adenosine x3, flecainide Home in 24hr

23
Some kind of shock A true story 14 yr boy c/o faintness, breathlessness HR 190, BP 80/40, weak pulse, CRT 5sec Rx 20ml/kg. No effect Rx 20ml/kg. C/o chest pain, can’t breathe …..?! ECG, diuretic, adenosine x3, flecainide Home in 24hr Problem: Misapplication of the APLS Method & CRT Test Root cause:a) Dr believed CRT clinched need for volume Rx b) “APLS emphasises CRT as having supportive value in diagnosis of hypovolaemia” [wrong] What could be done better? Tachycardic patient…..ECG Monitor shows more than a Number!
 Dr believed CRT clinched need for volume Rx b) APLS emphasises CRT as having supportive value in diagnosis of hypovolaemia [wrong] What could be done better. Tachycardic patient…..ECG Monitor shows more than a Number!.")
24
14 yr boy c/o severe chest pain & breathlessness HR 160, BP 80/40, weak pulse, CRT >4sec “Doctor he’s got severe chest pain…” “Sorry nurse, but look, he’s really shocked, he’s got delayed CRT, get that saline running stat…” Rx 1L crystalloid. C/o can’t breathe. CRT >4sec Rx 1L crystalloid, CRT >4sec; 1L colloid………! VF arrest…..!! DCShocks, Intubate+PEEP, diuretic, pacing, aortic counterpulsation cardiac catheterisation ECG Anterolateral MI (anomalous LCA). Cardiogenic shock Another true story
. Cardiogenic shock Another true story.")
25
14 yr boy c/o severe chest pain & breathlessness HR 160, BP 80/40, weak pulse, CRT >4sec “Doctor he’s got severe chest pain…” “Sorry nurse, but look, he’s really shocked, he’s got delayed CRT, get that saline running stat…” Rx 1L crystalloid. C/o can’t breathe. CRT >4sec Rx 1L crystalloid, CRT >4sec; 1L colloid………! VF arrest…..!! DCShock, Intubate+PEEP, diuretic, aortic counterpulsation and cardiac catheterisation ECG Anterolateral MI (anomalous LCA). Cardiogenic shock Another true story Diagnosis: Abuse of the APLS Method Root cause: a) Dr believed CRT clinched hypovolaemic shock b) Dr asserted that ABC precedes “diagnosis” c) Dr unable to listen to an experienced nurse and finally d) Dysfunctional self-critiquing result – denial
. Cardiogenic shock Another true story Diagnosis: Abuse of the APLS Method Root cause: a) Dr believed CRT clinched hypovolaemic shock b) Dr asserted that ABC precedes diagnosis c) Dr unable to listen to an experienced nurse and finally d) Dysfunctional self-critiquing result – denial.")
26
Capillary Refill Time How useful is it really?

27
Capillary refilling time in newborn babies: normal values. Strozik, Pieper, Roller. Arch Dis Child 1997;76:F193-6 Ambient temp 23 ± 1 0 C Ambient temp 23 ± 1 0 C Cot nursed Babies under radiant warmers Babies in incubators 2 populations of babies assessed by 2 independent observers. No inter-user reliability data included. Upper limit of CRT 3.22sec in all 4 sites tested

28
Capillary refill time in the hands and feet of normal newborn infants. Raju NV, Maisels MJ, Kring E, Schwarz-Warner L. Clinical Pediatrics 1999;38:139-44 Healthy 36 – 42 wks gestation, Age 1hr – 120hr Mean CRT (s)SDRange Hand 4.2 sec 1.471.6 – 8.8 sec Foot 4.6 sec 1.412.2 – 9.9 sec
SDRange Hand 4.2 sec – 8.8 sec Foot 4.6 sec – 9.9 sec.")
29
Capillary refill time in term neonates: bedside assessment. Raichur, Aralihond, Patil. Indian Journal of paediatrics 2001;68:613-5 Healthy 37 – 42 wks gestation, Age 1hr – 168hr; Room temp 26 – 30 0 C (mean 28.4) Observer 1 Observer 2 Mean SD Range Mean SD Range p Forehead 2.6 0.8 (1.2 - 3.7) 1.9 0.6 (0.8 – 3.6) <0.001 Chest 2.7 0.4 (1.7 – 4.4) 2.6 0.7 (1.1 – 4.8) NS Forehead 2.6 0.8 (1.2 - 3.7) 1.9 0.6 (0.8 – 3.6) <0.001 Chest 2.7 0.4 (1.7 – 4.4) 2.6 0.7 (1.1 – 4.8) NS Palm 3.0 0.6 (1.5 – 5.3) 2.8 1.1 (1.3 – 6.9) <0.05 Heel 3.1 0.8 (1.8 – 5.6) 4.2 1.8 (1.6 – 10.0) <0.001
 Observer 1 Observer 2 Mean SD Range Mean SD Range p Forehead 2.6 0.8 ( ) 1.9 0.6 (0.8 – 3.6) <0.001 Chest 2.7 0.4 (1.7 – 4.4) 2.6 0.7 (1.1 – 4.8) NS Forehead 2.6 0.8 ( ) 1.9 0.6 (0.8 – 3.6) <0.001 Chest 2.7 0.4 (1.7 – 4.4) 2.6 0.7 (1.1 – 4.8) NS Palm 3.0 0.6 (1.5 – 5.3) 2.8 1.1 (1.3 – 6.9) <0.05 Heel 3.1 0.8 (1.8 – 5.6) 4.2 1.8 (1.6 – 10.0) <")
30
Capillary refill time in term neonates: bedside assessment. Raichur, Aralihond, Patil. Indian Journal of paediatrics 2001;68:613-5 Healthy 37 – 42 wks gestation, Age 1hr – 168hr; Room temp 26 – 30 0 C (mean 28.4) 2 SD upper limit (approx 95%) 2 SD upper limit (approx 95%) Observer 1 Observer 2 4.2 sec 3.1 sec 3.5 sec 4.0 sec Forehead 4.2 sec 3.1 sec Chest 3.5 sec 4.0 sec Comment: longer CRT than one would expect for the ambient temperature? & note the variability between users
 2 SD upper limit (approx 95%) 2 SD upper limit (approx 95%) Observer 1 Observer sec 3.1 sec 3.5 sec 4.0 sec Forehead 4.2 sec 3.1 sec Chest 3.5 sec 4.0 sec Comment: longer CRT than one would expect for the ambient temperature. & note the variability between users.")
31
Capillary refilling time in newborn babies: normal values. Strozik, Pieper, Roller. Arch Dis Child 1997;76:F193-6 Ambient temp 23 ± 1 0 C Cot nursed Babies under radiant warmers Babies in incubators 2 populations of babies assessed by 2 independent observers. No inter-user reliability data included. Upper limit of CRT 3.22sec in all 4 sites tested !!

32
CRT relationship with HR and BP in 42 AGA term neonates 1-4hr old, T ax 36.5 – 37.0 Duration of pressure had substantial and highly significant difference to the result. Moderate direct relationship with systolic, diastolic, and mean BP: r p Sys BP0.35 0.02 Mean BP0.490.001 Dia BP0.430.005 Capillary refill time is an unreliable indicator of cardiovascular status in term neonates. LeFlore JL, Engle WD. Adv Neonatal Care 2005;5:174-54

33
Capillary refill time significantly prolonged by > 1sec at low ambient temp (mean 19.5 C) compared with warmer ambient temp (mean 25.7 C) who had normal CRT of <2sec. Significant inter-user variability even amongst experienced professionals. before and during Q: What ambient temp are your patients subjected to before and during assessment? Effect of ambient temperature on capillary refill in healthy children. Gorelick MH, Shaw KN, Baker MD. Pediatrics 1997 92: 699-702

34
Capillary refill – is it a useful predictor of hypovolemic states? Schriger DL, Baraff LJ. Annals of Emergency Medicine 1991;20:601-5 Mean CRT SDRange Blood Donors (500ml) Before 1.4 0.70.6 – 3.7 After 1.1 0.70.4 – 4.0 Clinically hypovolaemic patients *Orthostatic signs 1.9 0.70.8 – 3.3 Hypotension 2.8 1.21.1 – 5.1 Total 2.8 1.00.8 – 5.1 *Orthostatic signs: CRT sensitivity 47%
 Before – 3.7 After – 4.0 Clinically hypovolaemic patients *Orthostatic signs – 3.3 Hypotension – 5.1 Total – 5.1 *Orthostatic signs: CRT sensitivity 47%.")
35
Prior probabilityAccuracy+Predictive-Predictive of hypovolaemia Value Value 10% 89% 43% 93% 25% 80% 69% 81% 50% 64% 87% 59% 90% 40% 98% 14% Capillary refill – is it a useful predictor of hypovolemic states? Schriger DL, Baraff LJ. Annals of Emergency Medicine 1991;20:601-5

36
In an adult population in which half of the patients have hypovolaemia with hypotension or abnormal postural vital signs, capillary refill time measured by trained observers with stopwatches in a temperature-controlled environment with good lighting will classify subjects correctly only two thirds of the time.

37
Is measurement of capillary refill time useful as part of the initial assessment of children? Leonard PA, Beattie TF. Eur J Emergency Med 2004; 11: 158-63 7 month cohort n=4878 No significant association between CRT and: –Meningococcal disease –Other significant bacterial illness Significant association with: –More urgent triage category –Administration of fluid bolus –Duration of hospital stay

38
Best performance using > 3sec as criterion Pos predictive value Neg predictive value Triage Category 1,2 9% 97% Requiring Fluid Bolus 11% 99% Hospital Admission 55% 65% Stay >2d or Death 22% 91% Is measurement of capillary refill time useful as part of the initial assessment of children? Leonard PA, Beattie TF. Eur J Emergency Med 2004; 11: 158-63

39
Capillary refill time as indicator of shock in PICU Capillary refill time >= 6 sec predicted abnormally low SVI (<30ml/m 2 ) with sensitivity of 57% and specificity of 94%. Likelihood ratio of positive test (CRT>=6) is 9.5 CRT >=3sec LR = 1.6. Unlikely to be helpful at CRT >=2 ! Capillary refill and core-peripheral temperature gap as indicators of haemodynamic status in paediatric intensive care patients. Tibby, SM, Hatherill M, Murdoch IA. Arch Dis Child 1999; 80:163-6
 is 9.5 CRT >=3sec LR = 1.6. Unlikely to be helpful at CRT >=2 . Capillary refill and core-peripheral temperature gap as indicators of haemodynamic status in paediatric intensive care patients. Tibby, SM, Hatherill M, Murdoch IA. Arch Dis Child 1999; 80:")
40
The Child with non-blanching rash: how likely is meningococcal disease? Wells LC, Smith JC, Weston VCD, Collier J, Rutter N. Arch Dis Child 2001;85:218-22 Prospective study 233 non-blanching rash over 1yr Excluded 15 with “clear” alternative diagnoses), leaving n=218 11% of 218 finally shown to have meningococcal disease BP & other variables & signs are presented HR data were not presented
, leaving n=218 11% of 218 finally shown to have meningococcal disease BP & other variables & signs are presented HR data were not presented.")
41
The Child with non-blanching rash: how likely is meningococcal disease? Wells LC, Smith JC, Weston VCD, Collier J, Rutter N. Arch Dis Child. VariableSens% Spec% PPV % NPV% Odds Ratio CRT>2sec 83 85 42 98 (92-100) 29.4 Hypotension 28 97 71 84 12.7 Fever >38 5 58 81 27 94 8.0 Purpura too 83 88 47 98 (92-100) 37.2 Illness (defined) 79 81 35 97 16.7 CRP >6mg/L 100 54 18 100 (92-100) 0 (0-3%) Rash beyond SVC 100 38 17 100 (91-100) 0 (0-4%) Population n=218 with 11% final prevalence of the diseasewho already have a non-blanching rash. Population n=218 with 11% final prevalence of the disease who already have a non-blanching rash.
 29.4 Hypotension Fever > Purpura too (92-100) 37.2 Illness (defined) CRP >6mg/L (92-100) 0 (0-3%) Rash beyond SVC (91-100) 0 (0-4%) Population n=218 with 11% final prevalence of the diseasewho already have a non-blanching rash. Population n=218 with 11% final prevalence of the disease who already have a non-blanching rash..")
42
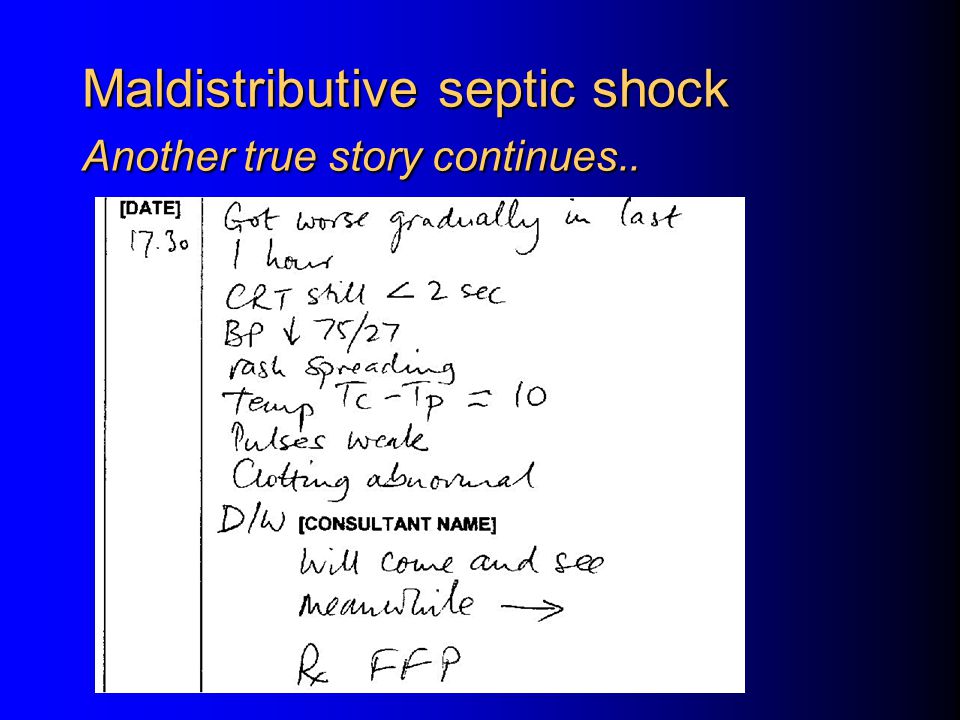
Maldistributive septic shock with non-blanching rash Another true story.. 19mo boy 8hr earlier: vomited x3, not apparently ill 3hr earlier: unwell, 1 blanching spot on chest 1hr earlier: S/B Walk-In Clinic Dr: New petechiae over chest, ill-looking Admitted to hospital urgently

43
Maldistributive septic shock Another true story continues..

46
Invasive Meningococcal Disease Meningitis without shock Rising ICP and aggressive fluid therapy: a deadly combination. Unconscious, petechiae, minimal- or easily- corrected haemodynamic disturbance: THINK BRAIN Early intubation to protect airway and control ventilation Use cerebral protective drugs at intubation Ensure good perfusion, but don’t overdo volume boluses. Think mannitol 0.25 – 0.5 g/kg

47
“Poor capillary refill and differential pulse volumes are neither sensitive nor specific indicators of shock in infants and children, but are useful clinical signs when used in conjunction with the other signs described. They should not be used as the only indicators of shock, nor as quantitative measures of the response to treatment.” Advanced Paediatric Life Support, 3 rd Ed. 2001; p16 Advanced Paediatric Life Support, 4 th Ed. 2005; p62-3

48
“Poor capillary refill and differential pulse volumes are neither sensitive nor specific indicators of shock in infants and children, but are useful clinical signs when used in conjunction with the other signs described. They should not be used as the only indicators of shock, nor as quantitative measures of the response to treatment.” Advanced Paediatric Life Support, 3 rd Ed. 2001; p16 Advanced Paediatric Life Support, 4 th Ed. 2005; p62-3

49
“Poor capillary refill and differential pulse volumes are neither sensitive nor specific indicators of shock in infants and children, but are useful clinical signs when used in conjunction with the other signs described. They should not be used as the only indicators of shock, nor as quantitative measures of the response to treatment.” Advanced Paediatric Life Support, 3 rd Ed. 2001; p16 Advanced Paediatric Life Support, 4 th Ed. 2005; p62-3

50
The validity and clinical reliability of clinical signs in the diagnosis of dehydration in children. Gorelick MH, Shaw KN, Murphy KO. Pediatrics 99(5) 1997 URL e6 Diagnostic performance of 10 individual clinical findings Sensitivity Specificity Kappa w Decreased skin elasticity0.350.97 0.55 Capillary refill >2 sec0.480.96 0.65 * General appearance0.590.91 0.61 * Absent tears0.670.89 0.75 * Abnormal respiration0.430.86 0.40 Dry mucous membranes0.800.78 0.59 * Sunken eyes0.600.84 0.50 Abnormal radial pulse0.430.86 0.59 Tachycardia HR>1500.460.79 - Decreased urine output0.850.53 0.75
 1997 URL e6 Diagnostic performance of 10 individual clinical findings Sensitivity Specificity Kappa w Decreased skin elasticity Capillary refill >2 sec * General appearance * Absent tears * Abnormal respiration Dry mucous membranes * Sunken eyes Abnormal radial pulse Tachycardia HR> Decreased urine output")
51
Is this child dehydrated? Steiner MJ, deWalt DA, Byerley JS. JAMA 2004;291:2746-53 Evidence-based assessment of literature 110 articles, 84 excluded. 3 assigned to Level 3 quality criteria 11 assigned to Level 4 quality criteria NONE at Level 1 or 2 Best individual signs for assessing dehydration are: –prolonged CRT –abnormal skin turgor –abnormal respiratory patterns

52
APLS Message Dehydration APLS uses CRT as an adjunct for determining the presence of shock. APLS makes no mention of CRT in the workshop on fluids in connection with dehydration.

53
APLS Testing (In)Appropriate use of CRT Scenarios and MCQ are not designed with opportunities to test for inappropriate use of the CRT as a guide to fluid therapy: –Trauma +/- exposure to elements –Brought in from the cold –Hypothermic –Non-hypovolaemic shock –Using CRT during cardiac arrest (!!!) –Communicating CRT with priority over HR, BP, & features of underperfusion
Appropriate use of CRT Scenarios and MCQ are not designed with opportunities to test for inappropriate use of the CRT as a guide to fluid therapy: –Trauma +/- exposure to elements –Brought in from the cold –Hypothermic –Non-hypovolaemic shock –Using CRT during cardiac arrest (!!!) –Communicating CRT with priority over HR, BP, & features of underperfusion")
54
CRT: Summary A rapid clinical assessment of…something “Normal” value not especially age-related But: is the clinical assessment tool reliable? Consequences of giving too much fluid? –Special problems Non-hypovolaemic shock Meningitis ARDS Infancy

55
Conclusion ALSG could consider reallocating CRT from Shock to Dehydration assessment ALSG could consider including testing for appropriate use of CRT Fluid deficit correction is a “gestalt” approach NOT a “one-test-solves-all” Is this child ill? Potentially ill? Context? Is there a reason for extreme caution? Does the overall story with findings indicate intravascular hypovolaemia? Does the overall story with findings indicate dehydration?



>")

>")










? 二、 Purposes or goals of child assessment Educational and clinical.>")





