Download presentation
Presentation is loading. Please wait.

1
STROKE John P. Connolly MD Medical Director, Resp Care Lodi Memorial Hospital Assoc Clin Prof Medicine UC Davis

3
STROKE Acute brain disorder of vascular origin accompanied by neurological dysfunction that persists for longer than 24 hours… Stroke 1990 One death every 4 seconds in the US… Circulation 2013

5
TIA Less than 24 hours “clinical reversibility” 1/3 of TIAs are associated with cerebral infarction

6
TIME IS BRAIN TISSUE Each minute of cerebral infarction results in destruction of 1.9 million neurons and 7.5 miles of myelinated nerves… Stroke 2006

8
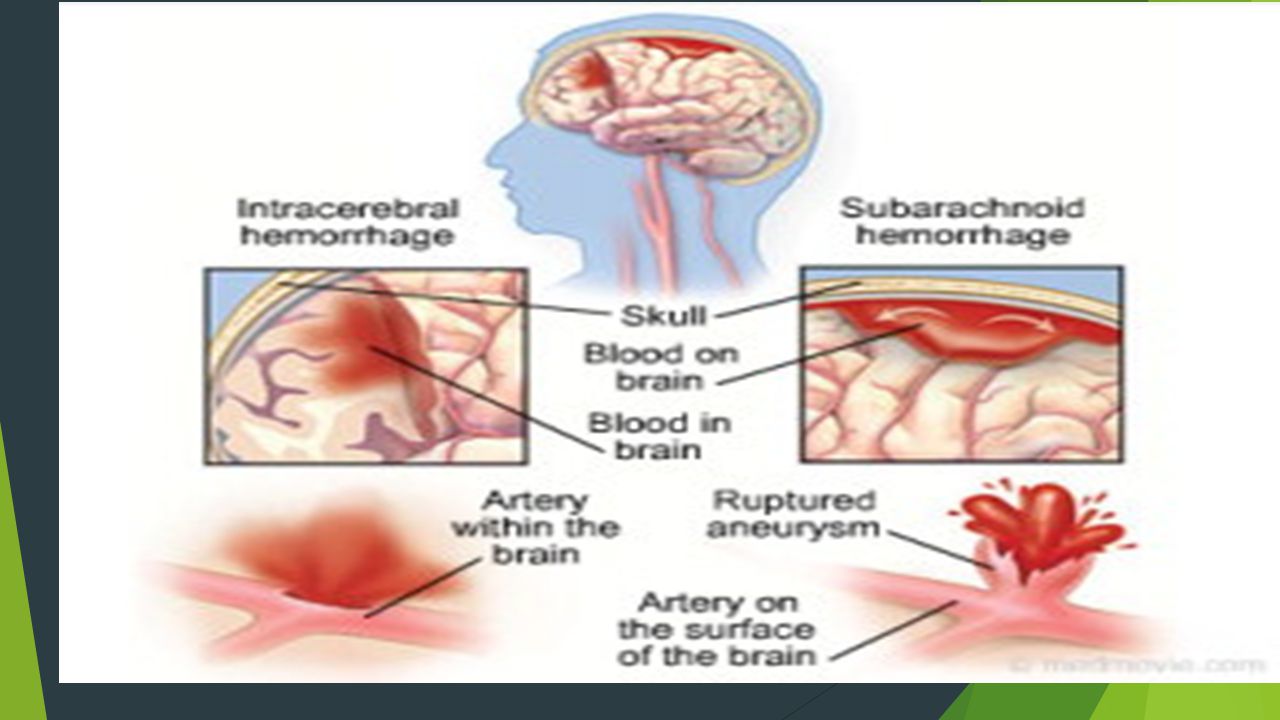
CLASSIFICATION Ischemic Stroke 87% 80% thrombotic 20% embolic Hemorrhagic Stroke 13% 97% intracerebral 3% subdural

24
INITIAL EVALUATION Clinical diagnosis most are unilateral/ no LOC if coma –> hemorrhagic CVA brainstem CVA non-convulsive seizure Left hemispheric damage -> aphasia disturbance in comprehension/formation of language receptive expressive global contralateral weakness – can be due to seizure hemiparesis can result from hepatic encephalopathy or sepsis

25
Suspected CVA 30% will have another condition Seizures Sepsis Metabolic encephalopathies Space occupying lesions …..in that order

26
NIH Stroke Scale…NIHSS 11 different aspects of performance with a number from 0 to 3 or 4 Total score 0 to 41 >22=poor prognosis <10=unlikely to be CVA

27
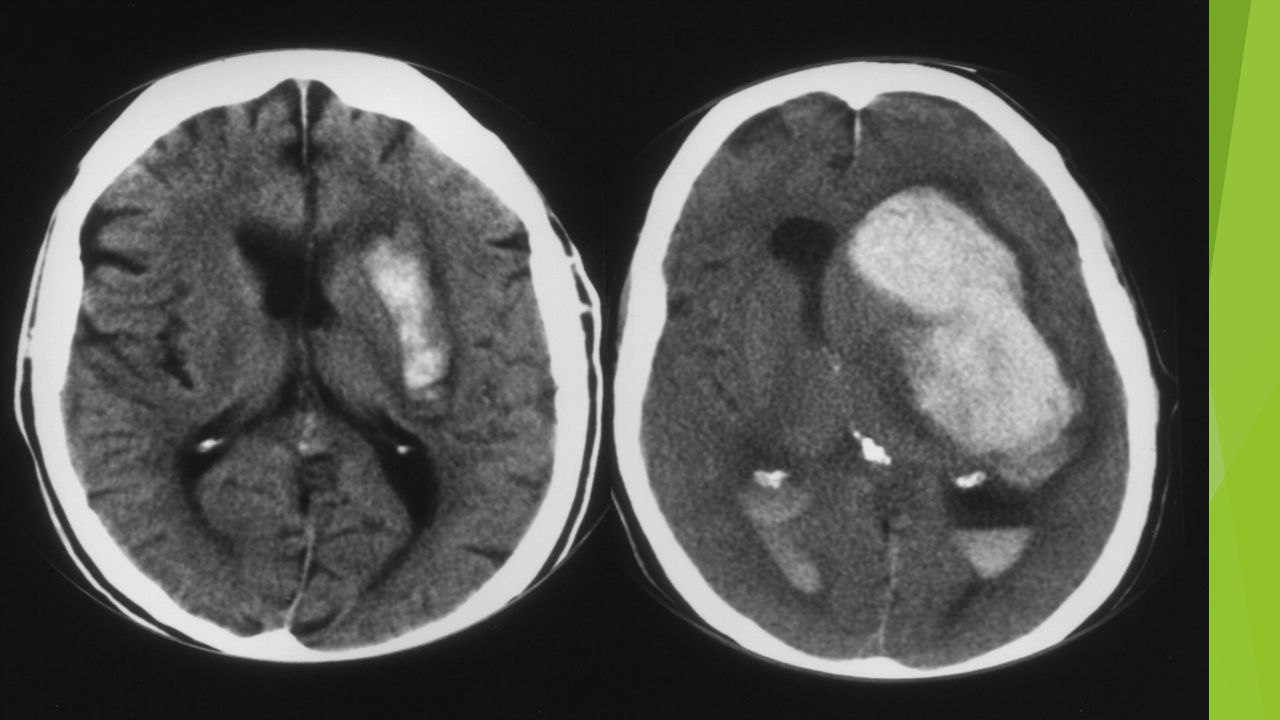
IMAGING CT…reliable for intracranial hemorrhage close to 100% sensitive not sensitive for ischemic CVA…especially early MRI…diffusion weighted hyperdense regions of ischemia can detect ischemia after 5-10 minutes time consuming….cooperation issues ECHO…echocardiography can identify source of cerebral emboli identify patent foramen ovale

28
THROMOLYTIC THERAPY Selection criteria inclusion exclusion relative exclusion Time limit recently expanded to 4-5 hours Balance against 6-7% incidence of cerebral hemorrhage with lytic Rx Time of stroke onset can be difficult to pinpoint HBP as an exclusion…>185S/>110D labetalol, nicardipine, nitroprusside

29
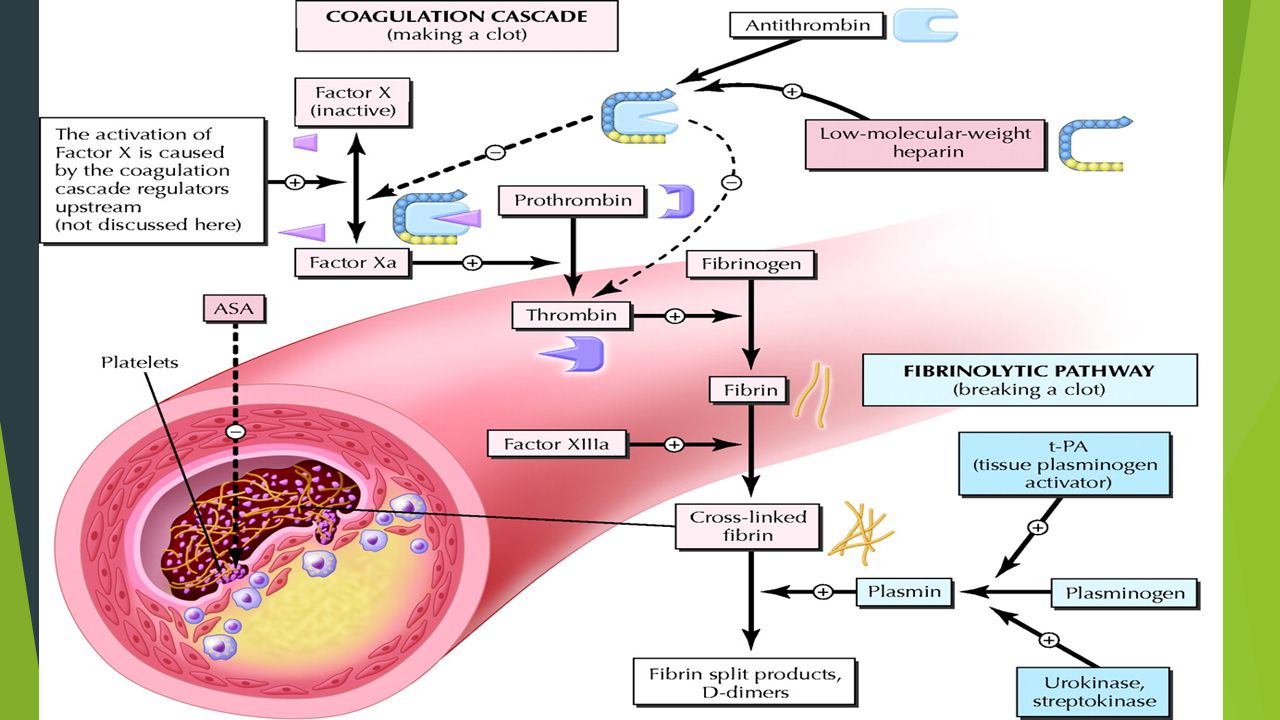
THROMBOLYSIS As early as possible rtPA 0.9 mg/kg up to 90 mg 10% in 1-2 minutes/ remained over 60 minutes No anticoagulant or antiplatelet agent for 24 hours Then only SQ heparin for DVT prophylaxis and ASA 325 given 24-48 hours after CVA then 81 mg a day

31
OTHER THERAPY Oxygen…if O2 is ok then no benefit toxic oxygen metabolites promote cerebral vasoconstriction only if sat < 94% BP Control…HBP in 60-65% of CVAs usually corrects in 48-72 hours correction only id >220S/>120D or acute MI labetalol, nicardipine, nitroprusside(can increase ICP) Fever Control…fever in 30% can be infection or due to tissue necrosis intracranial blood fever harmful to brain tissue
 Fever Control…fever in 30% can be infection or due to tissue necrosis intracranial blood fever harmful to brain tissue")
32
GUIDELINES REVIEWED AHA/ASA Guidelines for the early management of patients with acute ischemic stroke Stroke 2013 44: 870-947 AHA/ASA Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack Stroke 2014 45: 2160-2236 AHA/ASA Palliative and end of life care in stroke Stroke 2014 45: 1887-1916

33
Early Management of CVA “5 suddens”….weakness, speech, visual loss, headache, dizziness “FAST”…face, arm, speech, time

34
http://mmcneuro.files.wordpress.com/2013/01/stroke.gif

35
EMS Prehospital Stroke Screen LA prehospital Stroke Screen Cincinnati Prehospital Stroke Scale Stroke Center Transport Primary Stroke Center Comprehensive Stroke Center/neuro critical care Emergency time…eval and begin fibrinolytic rx <60 min of ED arrival NECT or MRI < 45 minutes assess BG but no delay for ECG, CXR, troponin

36
General Support Correct hypoxemia ?supplemental O2 Supine position Cardiac Monitoring BP control Intubation for unconsciousness or bulbar dysfunction Correct hypovolemia and hypoglycemia 140-180 Temperature < 38 degrees

37
rtPA {Alteplase} With normal or early ischemic change on imaging If frank hypodensity >1/3 MCA no rtPA Unclear use…mild deficits improving CVA symptoms surgery< 3 months recent MI Maybe harmful in pts on dabigatran, apixaban, rivaroxiban Other lytics…not recommended (streptokinase) or investigational
 or investigational")
38
rtPA 0.9 mg/kg up to 90 mg IV within 3 hours Door to needle < 60 minutes Can treat 3-4.5 hours with more exclusions With BP control <185/110 Complications…angioedema, bleeding

39
Management Decisions Endovascular interventions inter-arterial rtPA…no FDA approval mechanical thrombectomy emergency angioplasty and stenting Anticoagulation within 24 hours of rtPA…not recommended ASA 24 hours later ok glycoprotein 2b/3a inhibitors not recommended abciximab,eptifibatide, tirofiban

40
Management Decisions Volume expansion, vasodilators, induced hypertension…no Albumin, hemodilution…no Some use of vasopressors to support BP Neuroprotective agents statins…should be continued, ? Started hypothermia…not proven transcranial infrared laser…no hyperbaric oxygen….only for air embolism drugs…EtOH, Magnesium, Caffeine…not established

41
General Care Specialized Stroke Units Infection therapy/DVT prophylaxis Swallow eval before po intake Early mobilization No benefit to specialized nutritional therapy or prophylactic antibiotics Surgical intervention…emergent CEA not established

42
Treatment of Complications Brain edema/Increased ICP…peaks 3-4 days after CVA restriction free water avoid excess glucose minimize hypoxemia and hypercarbia treat hyperthermia elevate HOB 20-30 degrees avoid antihypertensive agents causing cerebral vasodilation Treatment of increased ICP hyperventilation, hypertonic saline, osmotic diuretics Interventricular CSF drainage Steroids not recommended decompressive surgery…effective…decisions based on volume of tissue infarcted and midline shift

43
Treatment of Complications Hemorrhagic transformation within 24 hours of rtPA most fatal hemorrhages within 12 hours optimal management debated ?cryoprecipitate ? tranexamic acid Seizures….standard anti-epileptic therapy prophylactic anticonvulsants not indicated Acute hydrocephalus placement of ventricular drain Palliative Care

44
Secondary Prevention of CVA Control of Risk Factors Intervention for vascular obstruction Antithrombotic therapy for cardioembolic stroke Antiplatelet therapy for noncardioembolic stroke Special circumstances

46
Risk Factor Control HBP…risk for CVA rises directly with BP>115 syst No benefit to systolic <120 BP Rx if >140/90 several days post CVA lacunar infarct – goal<130 syst Lipids…statin to LDL-C <100 DM…screen all CVA patients with HgbA1C

47
Risk Factor Control Obesity…BMI< 30 usefulness of weight loss uncertain for secondary prevention Risk for CVA rises above BMI 20 Metabolic Syndrome…overweight, trig, low HDL-C, high BP, high BG ….20% of adults over 20 Physical Inactivity … 40 minutes 3-4x a week ….supervision by PT or Rehab after CVA Nutrition…over or under, routine supplements not helpful vitamins not helpful, Mediterranean diet possibly helpful

49
Risk Factor Control OSA…very high incidence…sleep studies Cigarettes…strong risk for 1 st CVA second hand smoke increases risk EtOH…light to moderate decreases 1 st ischemic CVA risk increased risk of hemorrhagic CVA with any EtOH heavy EtOH increases risk for both types

50
Extracranial Carotid / VertebrobasilarDisease CEA for > 70% stenosis Not recommended for < 50% Carotid Angioplasty and stent vs. CEA Older patients…CEA better Younger…equivalent Optimal Medical Therapy Vertebrobasilar…medical therapy, BP lowering, lipid control Stenting vs VB endarterectomy considered

51
Intracranial Disease and Cardioembolic Disease Atherosclerosis…>50% ASA> warfarin BP control and high Intensity statin therapy >70% add clopidogrel for 90 days Cardioembolism…Afib is main risk warfarin, apixaban, dabigatran, for nonvalvular afib rivaroxaban also reasonable anticoagulation and antiplatelet Rx if CAD

52
Cardiac Disease Acute MI/LV Thrombus…VKA for 3 months or apixaban dabigatran rivaroxaban Cardiomyopathy…LVAD…VKA EF< 35% anticoagulation and antiplatelet Valvular Heart Dz…MV Disease plus Afib…VKA MV Disease without Afib…consider VKA CVA/TIA on VKA…add ASA Prosthetic Heart Valves…Mechanical AV/MV….VKA plus ASA 81 Bioprosthetic…ASA if CVA …add VK

53
Non-cardioembolic CVA/ Aortic Arch/ ICH Antiplatelet agents ASA and dipyridamole or clopidogrel ?Add VKA….unclear importance Aortic Arch Atheroma antiplatelet therapy and statin VKA or surgery not recommended Arterial Dissection ??surgery …Antiplatelet therapy or anticoagulation considered ICH…controversy…high risk of bleed…antiplatelet therapy restart anticoagulation > 1 week

54
Other risks PFO Hyperhomocystinemia Thrombophilia Antiphospholipid antibodies HbSS Venous sinus thrombosis Pregnancy risks LMWH or UFH every 12 hours or heparin until the 13 th week followed by VKA

56
Palliative/End of Life Care 2010…130,000 CVA deaths/ >5% of all deaths 50% in hospital 35% SNFs 15% home/other 20% of CVAs to SNF 30% of CVAs permanently disabled

57
Grief/ Pain/ Non-pain Issues Anticipatory and acute grief Complicated grief/depression…1-2 months later more severe if acute loss Pain…central post stroke pain….1-12% hemiplegic shoulder pain post-CVA spasticity Non-pain…fatigue, incontinence, seizures, sexual dysfunction, sleep disordered breathing, depression, anxiety/delirium, emotional lability

59
Palliative Care/ Prognosis & Decision Making “what is a good outcome” Aspects of recovery most important to patient and family Decision making…Surrogate Decision Makers Cultural and Religious preferences Bereavement Services Available Preference Sensitive Decisions…DNR/DNI Swallowing Care Decompressive Craniectomy, etc.

61
Access to Palliative Care Interdisciplinary Collaborative/patient centered communication Services available Peace and dignity Access…any CVA affecting daily functioning or reducing life expectancy Goals of care…communication, best available science, acknowledge uncertainty, changes in preferences over time

62
A final Word…Paul Marino MD (2014) Number of Strokes each year in US 700,000 Number of Ischemic Strokes (88%) 616,000 Number of Stroke Patients receiving lytic therapy 12,320 Number of pts who benefit from lytic Rx (1 in 9) 1,369 Percent of strokes that benefit from lytic RX 0.2%
 Number of Strokes each year in US 700,000 Number of Ischemic Strokes (88%) 616,000 Number of Stroke Patients receiving lytic therapy 12,320 Number of pts who benefit from lytic Rx (1 in 9) 1,369 Percent of strokes that benefit from lytic RX 0.2%")
Similar presentations































>")

 Stroke - Overview Third leading cause of death in industrialized countries. Total cost of strokes in the U.S. is roughly.>")




