Download presentation
Presentation is loading. Please wait.

1
Saving Lives By Strengthening Our Region’s Trauma Care System December 5, 2013 MICHAEL SLOAN, MD CASE STUDIES IN ABDOMINAL TRAUMA

2
WHEN TRAUMA IS OBVIOUS…

3
NO IMAGING IS NECESSARY

4
WHEN TRAUMA IS UNCERTAIN…

5
TROUBLE LURKS JUST BELOW THE SURFACE

6
TRAUMA Leading cause of death ages 1-44 years in most developed countries Motor vehicle crashes account for the majority of injuries and deaths in 70% of the 39 countries for which data is available 60 million injuries estimated in the US each year, resulting in 36.8 million ER visits

7
TRIMODAL DEATH DISTRIBUTION

8
ABDOMINAL TRAUMA Multiple Mechanisms of Injury 1.Crushing – direct application of blunt force 2.Shearing – sudden deceleration of organs with fixed attachments 3.Bursting – increased intraluminal pressure from abdominal compression 4.Penetrating – knife/gun/stick/bone

9
INJURIES Solid organ Hollow viscus Diaphragm Retroperitoneal Vascular Genitourinary Pelvic

10
YOUR TOOL KIT

11
YOUR DESTINATION

12
CASE #1 History 72 year old male status post auto versus bicycle No LOC (wearing helmet) Complaint of rib pain, hip pain, and lower extremity pain on arrival Level 2 Trauma activation GCS 15, HR 88, BP 138/66, RR 14, O2 sat 98% 2L NC
 Complaint of rib pain, hip pain, and lower extremity pain on arrival Level 2 Trauma activation GCS 15, HR 88, BP 138/66, RR 14, O2 sat 98% 2L NC")
13
INITIAL ASSESSMENT Airway Breathing Circulation Disability Exposure Working Diagnosis Rib fracture Low back pain Hip/Femur fracture

14
INITIAL IMAGING

15
WHILE AWAITING CT… HR 114, BP 114/60, RR 20, O2 sat 98% 2L NC Patient complaint of need to void “I can’t pee!” Nausea => Emesis Foley placed – amber urine (<50 mL) NG placed
 NG placed")
16
TRAUMA SURGERY AND ORTHOPEDICS AT THE BEDSIDE HR 122, BP 96/52, RR 22, O2 sat 97% 2L NC Patient complaint of back pain, need to have a bowel movement, becoming sedate (4 mg IV dilaudid at this point) Hct 32, plts 156, INR 1.4 As he rolls out to CT HR 160…
 Hct 32, plts 156, INR 1.4 As he rolls out to CT HR 160…")
17
WHAT DO YOU DO NEXT? Continue to CT? Return to room? Transfuse? Transfer? OR? FAST? Angio?

18
RETURN TO ROOM 2 nd PIV was placed NS bolus while transfusion initiated Med list confirms ASA and Plavix History of cardiac stent 7 months ago Platelets ordered Draw sheet placed FAST exam (suggests pelvic hematoma)
")
19
PATIENT IMPROVES… Transient or Sustained No angiography available HR 96, BP 122/54, RR 20 O2 95% 4L NC Decision to transfer

20
ON ARRIVAL GCS 14, HR 130, BP 104/50, RR 24 NRB 4L crystalloid, 4u pRBC, platelets in the cooler Repeat FAST – suggests free fluid Taken to OR Ex lap = small amount of free blood, retroperitoneal and pelvic hematoma (tense), temporary closure Binder applied and transfer to Angio suite
, temporary closure Binder applied and transfer to Angio suite")
21
ANGIOGRAPHY 4.5 hours to selectively access and embolize the left internal iliac branches (inferior gluteal/pudendal arteries) 7 u pRBC, 10 u platelets, 5 u FFP Remember to employ massive transfusion protocol Return to OR for 2 nd look laparotomy directly from Angio suite External fixator applied at this time
 7 u pRBC, 10 u platelets, 5 u FFP Remember to employ massive transfusion protocol Return to OR for 2 nd look laparotomy directly from Angio suite External fixator applied at this time")
22
OR – ROUND TWO Retroperitoneal/pelvic hematoma has now begun to bleed from the midline Exploration reveals no obvious bleeding and abdomen is packed and left open with VAC ABThera Two additional trips to the OR for VAC change Definitive abdominal closure on HD#7

23
RECOVERY 13 days ICU 27 days hospital 2 months LTACH 2 months SNF Ongoing outpatient rehab for gait impairment Ventral hernia

24
PELVIC FRACTURES Prior to 1900, pelvic fractures with an associated bleed carried a mortality of 80% Today management revolves around early recognition and minimizing morbidity Associated injuries are common CHI 50% Long Bone Fx 48% Thoracic Injury 21% Liver/Spleen 7% each GI/GU Tract 5% each Trauma 6 th Ed. Feliciano et al. p.781

25
VASCULAR ANATOMY The iliac artery and venous trunks run ventral to the sacroiliac joint bilaterally Lateral compression, anterior compression, or vertical shear result in ligamentous/bony injury which are often visible on plain film Arterial injury often presents with a continued hemodynamic decompensation Venous injury often will tamponade

26
EAST GUIDELINES FOR PELVIC FRACTURE 1. Which patients with hemodynamically unstable pelvic fractures warrant early external mechanical stabilization? 2. Which patients require emergent angiography? 3. What is the best test to exclude extrapelvic bleeding? 4. Are there radiologic findings which predict hemorrhage? 5. What is the role of noninvasive temporary external fixation devices? 6. Which patients warrant preperitoneal packing (PPP)?
 .")
27
1. WHICH PATIENTS WITH HEMODYNAMICALLY UNSTABLE PELVIC FRACTURES WARRANT EARLY EXTERNAL MECHANICAL STABILIZATION? The use of a pelvic orthotic device (POD) does not seem to limit blood loss in patients with pelvic hemorrhage. Level III recommendation The use of a POD effectively reduces fracture displacement and decreases pelvic volume. Level III recommendation Temporary Pelvic Binders (TPB) reduce 24 and 48 hour blood transfusion requirements when compared to early External Pelvic Fixation (EPF)
 does not seem to limit blood loss in patients with pelvic hemorrhage. Level III recommendation The use of a POD effectively reduces fracture displacement and decreases pelvic volume. Level III recommendation Temporary Pelvic Binders (TPB) reduce 24 and 48 hour blood transfusion requirements when compared to early External Pelvic Fixation (EPF).")
28
2. WHICH PATIENTS REQUIRE EMERGENT ANGIOGRAPHY? Patients with pelvic fractures and hemodynamic instability or signs of ongoing bleeding after nonpelvic sources of blood loss have been ruled out should be considered for pelvic angiography/embolization. Level I recommendation Patients with evidence of arterial intravenous contrast extravasation (ICE) in the pelvis by CT may require pelvic angiography and embolization regardless of hemodynamic status. Level I recommendation Patients with pelvic fractures who have undergone pelvic angiography with or without embolization, who have signs of ongoing bleeding after nonpelvic sources of blood loss have been ruled out, should be considered for repeat pelvic angiography and possible embolization. Level II recommendation Patients older than 60 years with major pelvic fracture (open book, butterfly segment, or vertical shear) should be considered for pelvic angiography without regard for hemodynamic status. Level II recommendation Although fracture pattern or type does not predict arterial injury or need for angiography, anterior fractures are more highly associated with anterior vascular injuries, whereas posterior fractures are more highly associated with posterior vascular injuries. Level III recommendation Pelvic angiography with bilateral embolization seems to be safe with few major complications. Gluteal muscle ischemia/necrosis has been reported in patients with hemodynamic instability and prolonged immobilization or primary trauma to the gluteal region as the possible cause, rather than a direct complication of angioembolization. Level III recommendation Sexual function in males does not seem to be impaired after bilateral internal iliac arterial embolization. Level III recommendation
 in the pelvis by CT may require pelvic angiography and embolization regardless of hemodynamic status. Level I recommendation Patients with pelvic fractures who have undergone pelvic angiography with or without embolization, who have signs of ongoing bleeding after nonpelvic sources of blood loss have been ruled out, should be considered for repeat pelvic angiography and possible embolization. Level II recommendation Patients older than 60 years with major pelvic fracture (open book, butterfly segment, or vertical shear) should be considered for pelvic angiography without regard for hemodynamic status. Level II recommendation Although fracture pattern or type does not predict arterial injury or need for angiography, anterior fractures are more highly associated with anterior vascular injuries, whereas posterior fractures are more highly associated with posterior vascular injuries. Level III recommendation Pelvic angiography with bilateral embolization seems to be safe with few major complications. Gluteal muscle ischemia/necrosis has been reported in patients with hemodynamic instability and prolonged immobilization or primary trauma to the gluteal region as the possible cause, rather than a direct complication of angioembolization. Level III recommendation Sexual function in males does not seem to be impaired after bilateral internal iliac arterial embolization. Level III recommendation.")
29
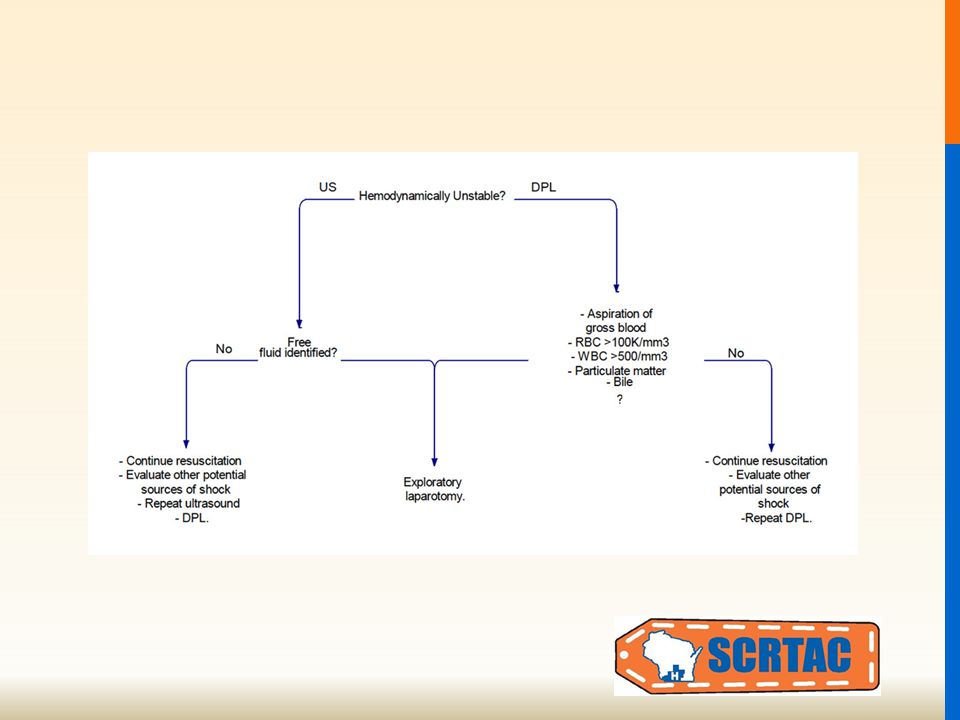
3. WHAT IS THE BEST TEST TO EXCLUDE EXTRAPELVIC BLEEDING? Focused Assessment with Sonography for Trauma (FAST) is not sensitive enough to exclude intraperitoneal bleeding in the presence of pelvic fracture. Level I recommendation FAST has adequate specificity in patients with unstable vital signs and pelvis fracture to recommend laparotomy to control hemorrhage. Level I recommendation Diagnostic peritoneal tap (DP)/Diagnostic peritoneal lavage (DPL) is the best test to exclude intra-abdominal bleeding in the hemodynamically unstable patient. Level II recommendation In the hemodynamically stable patient with a pelvic fracture, CT of the abdomen and pelvis with intravenous contrast is recommended to evaluate for intra-abdominal bleeding regardless of FAST results. Level II recommendation
 is not sensitive enough to exclude intraperitoneal bleeding in the presence of pelvic fracture. Level I recommendation FAST has adequate specificity in patients with unstable vital signs and pelvis fracture to recommend laparotomy to control hemorrhage. Level I recommendation Diagnostic peritoneal tap (DP)/Diagnostic peritoneal lavage (DPL) is the best test to exclude intra-abdominal bleeding in the hemodynamically unstable patient. Level II recommendation In the hemodynamically stable patient with a pelvic fracture, CT of the abdomen and pelvis with intravenous contrast is recommended to evaluate for intra-abdominal bleeding regardless of FAST results. Level II recommendation.")
30
4. ARE THERE RADIOLOGIC FINDINGS WHICH PREDICT HEMORRHAGE? Fracture pattern on pelvic X-ray does not single-handedly predict mortality, hemorrhage, or the need for angiography. Level II recommendation Presence/location of hematoma does not predict or exclude the need for angiography and possible embolization. Level II recommendation CT of the pelvis is an excellent screening tool to exclude pelvic hemorrhage. Level II recommendation Absence of contrast extravasation on CT does not always exclude active hemorrhage. Level II recommendation Pelvic hematoma >500 cm in size has an increased incidence of arterial injury and need for angiography. Level II recommendation Isolated acetabular fractures are as likely to require angiography as pelvic rim fractures. Level III recommendation If a retrograde urethrocystogram is required, it should be performed after CT with intravenous contrast. Level III recommendation

31
5. WHAT IS THE ROLE OF NONINVASIVE TEMPORARY EXTERNAL FIXATION DEVICES? TPBs effectively reduce unstable pelvic fractures as well as definitive stabilization and decrease pelvic volume. Level III recommendation TPBs may limit pelvic hemorrhage but do not seem to affect mortality. Level III recommendation TPBs work as well or better than emergent EPF in controlling hemorrhage. Level III recommendation

32
6. WHICH PATIENTS WARRANT PREPERITONEAL PACKING (PPP)? Retroperitoneal pelvic packing is effective in controlling hemorrhage when used as a salvage technique after angiographic embolization. Level III recommendation Retroperitoneal pelvic packing is effective in controlling hemorrhage when used as part of a multidisciplinary clinical pathway including a POD/C-clamp. Level III recommendation

34
CASE #2 History 49 year old female passenger, restrained, MVC Possible brief LOC Complaint of left chest/breast pain, mild right abdominal pain Level 2 Trauma activation GCS 15, HR 71, BP 154/94, RR 20, O2 sat 100% 6L

35
INITIAL ASSESSMENT Airway Breathing Circulation Disability Exposure Working Diagnosis ?LOC Breast pain Abdominal pain (mild)
")
36
INITIAL IMAGING

37
WHILE IN CT… Increased agitation = CT head negative GCS 14, HR 77, BP 51/35 CT chest/abd/pelvis in progress

39
WHILE IN CT… Scan stopped, IV bolus provided HR 74, BP 102/52 Delayed images show increased free fluid HR 74, BP 88/40 Taken to OR from CT scanner for exploration Shearing injury of abdominal wall Avulsion of 30 cm of distal ileum requiring resection Active bleeding from branch of ileocolic artery

41
BLUNT VISCERAL INJURY Sir McCormack in 1900 was the first to advocate “A man wounded in war in the abdomen dies if he is operated upon and remains alive if he is left in peace” Nonoperative Management has reported success rates of ~90% in properly selected patient populations – regardless of age, grade of injury, multivisceral injury, and mechanism of injury

46
FAST, DPL, DIAGNOSTIC LAPAROSCOPY Overall, FAST has a sensitivity between 73% and 88%, a specificity between 98% and 100% and is 96% to 98% accurate The accuracy of DPL has been reported between 92% and 98% Although there are no randomized, controlled studies comparing Diagnostic Laparoscopy (DL) to more commonly utilized modalities, experience at one institution using minilaparoscopy demonstrated a 25% incidence of positive findings on DL, which were successfully managed nonoperatively and would have resulted in nontherapeutic laparotomies
 to more commonly utilized modalities, experience at one institution using minilaparoscopy demonstrated a 25% incidence of positive findings on DL, which were successfully managed nonoperatively and would have resulted in nontherapeutic laparotomies")
47
OTHER ITEMS OF INTEREST Damage Control Surgery Abdominal Compartment Syndrome

48
DAMAGE CONTROL Traditional thinking = The best operation for a patient is a single, definitive procedure ER => OR => ICU Unfortunately, severely injured patients (ISS>35) are more likely to die from intra- operative metabolic failure, than from failure to complete a definitive procedure
 are more likely to die from intra- operative metabolic failure, than from failure to complete a definitive procedure")
49
DEATH TRIAD Hypothermia AcidosisCoagulopathy

50
OR POSSIBLY A LITTLE MORE COMPLEX

51
DAMAGE CONTROL IN PRACTICE Control hemorrhage Contain/Stop contamination Avoid further injury ER => OR => ICU => OR => ICU

52
GUIDELINES FOR INSTITUTING DAMAGE CONTROL pH < 7.2 Serum bicarbonate < 15 Core temp < 34 C Transfusion > 4 L pRBC Total blood products > 5 L Total fluid > 12 L If all of the above = death If one or more = damage control

53
ABDOMINAL COMPARTMENT SYNDROME https://www.wsacs.org/

56
QUESTIONS

Similar presentations











 advance ET tube B) needle thoracostomy.>")



-Score: Probability of Mass Transfusion as Surrogate for Life Threatening Hemorrhage after Multiple Trauma The.>")







. Straight to theatre? Time to laparotomy Trauma centre127 mins NCEPOD200 mins –NO CT110 mins –CT499 mins NO CT group unstable.>")



