Download presentation
Presentation is loading. Please wait.

1
Bronchopulmonary Dysplasia(BPD) Kumari Weeratunge M.D. PL - 2
 Kumari Weeratunge M.D. PL - 2")
2
Back ground Develops in neonates treated with O2 & PPV. Originally described by Northway in 1967 using clinical, radiographic & histologic criteria. Bancalari refined definition using ventilation criteria, O2 requirement @ 28days to keep PaO2>50mmhg & abnormalities in chest x –ray.

3
Back ground Shennan proposed in 1988 criteria of O2 requirement @ 36 weeks corrected GA. Antenatal steroids, early surfactant Rx & gentle modes of ventilation minimize severity of lung injury.

4
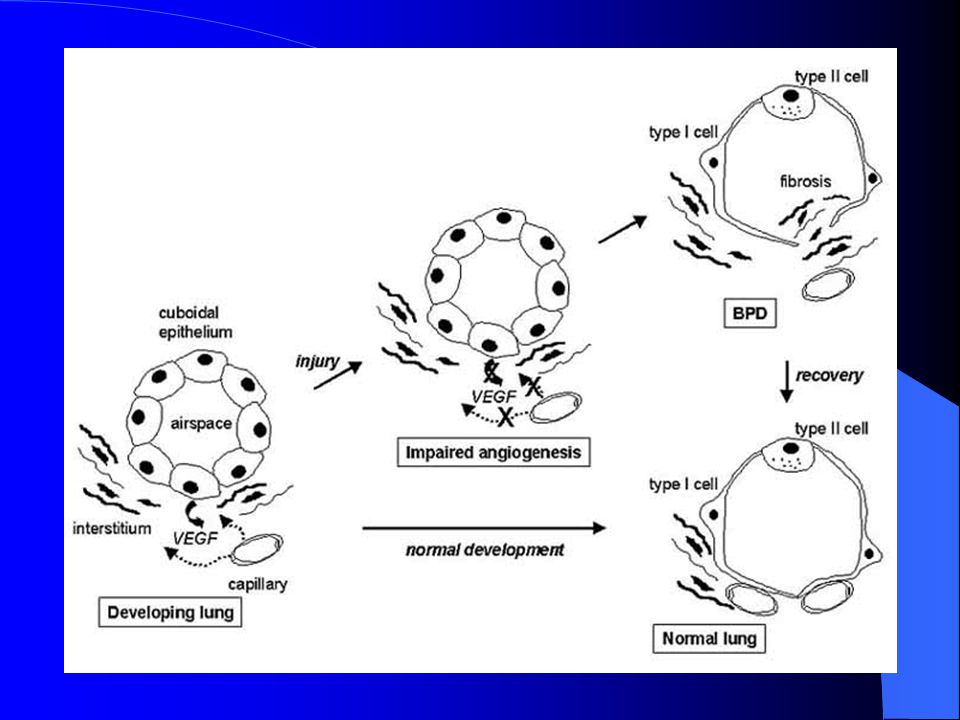
Pathophysiology Multifactorial Major organ systems - lungs & heart Alveolar stage of lung development - 36wks GA to 18 months post conception Mechanical ventilation & O2 interferes with alveolar & pulmonary vascular development in preterm mammals. Severe BPD Pulmonary HT & abnormal pulmonary vascular development.

5
Stages of BPD Defined by Northway in 1967 Stage 1 - similar to uncomplicated RDS Stage 2 - pulmonary parenchymal opacities with bubbly appearance of lungs Stage 3 & 4 – areas of atelectasis, hyperinflation & fibrous sheaths Recently CT & MRI of chest – reveals more details of lung injury

6
Frequency of BPD Dependent on definition used in NICU. Using criteria of O2 requirement @ 28 days frequency range from 17% - 57%. Survival of VLBW infants improved with surfactant Actual prevalence of BPD has increased.

7
Mortality/Morbidity of BPD Infants with severe BPD Increased risk of pulmonary morbidity & mortality within the first 2 years of life.

8
Pulmonary Complications of BPD Increased resistance & airway reactivity evident in early stages of BPD along with increased FRC. Severe BPD Significant airway obstruction with expiratory flow limitations & further increased FRC secondary to air trapping & hyperinflation

9
Volume trauma & Barotrauma Rx of RDS – surfactant replacement, O2, CPAP & mechanical ventilation. Increased PPV required to recruit all alveoli to Px atelectasis in immature lungs Lung injury Inflammatory cascade. Trauma secondary to PPV- Barotrauma Volumetrauma Lung injury secondary to excess TV from increased PPV.

10
Volume trauma & Barotrauma Severity of lung immaturity & effects of surfactant deficiency determines PPV. Severe lung immaturity Alveolar number is reduced increased PP transmitted to distal bronchioles. Surfactant deficiency some alveoli collapse while others hyper inflate.

11
Volume trauma & Barotrauma Increased PPV to recruit all alveoli Compliant alveoli & terminal bronchioles rupture leaks air in to interstium PIE Increase risk of BPD Using SIMV compared to IMV in infants <1000g showed less BPD.

12
O2 & Antioxidants O2 accept electrons in it’s outer ring Form O2 free radicals Cell membrane destruction Antioxidants(AO) Antagonise O2 free radicals Neonates-Relatively AO deficient Major antioxidants – super oxide dismutase, glutathione peroxidase & catalase
 Antagonise O2 free radicals Neonates-Relatively AO deficient Major antioxidants – super oxide dismutase, glutathione peroxidase & catalase")
13
O2 & Antioxidants Antioxidant enzyme level increase during last trimester. Preterm birth Increased risk of exposure to O2 free radicals

14
Inflammation Activation of inflammatory mediators In acute lung injury Activation of leukocytes by O2 free radicals, barotrauma & infection Destruction & abnormal lung repair Acute lung injury BPD Leukocytes & lipid byproducts of cell membrane destruction Activate inflammatory cascade

15
Inflammation Lipoxigenase & cyclooxigenase pathways are involved in the inflammatory cascade Inflammatory mediators are recovered in tracheal aspirate of newly ventilated preterm who later develops BPD Metabolites of mediators vasodilatation increased capillary permeability albumin leakage & inhibition of surfactant function risk of barotrauma

16
Inflammation Neutrophils – release collegenase & elastase destroy lung tissue Hydroxyproline & elastin recovered in urine of preterms who develops BPD Di2ethylhexylphthalate(DEHP) degradation product of used ET tubes lung injury A study in 1996 found that increased interleukin 6 in umbilical cord plasma
 degradation product of used ET tubes lung injury A study in 1996 found that increased interleukin 6 in umbilical cord plasma")
17
Infection Maternal cervical colonization/ preterm neonatal tracheal colonization of U.urealyticum associated with high risk of BPD

18
Nutrition Inadequate nutrition supplementation of preterm compound the damage by barotrauma, inflammatory cascade activation & deficient AO stores Acute stage of CLD increased energy expenditure New born rats nutritionally deprived decreased lung weight

19
Nutrition Cu, Zn, Mn deficiency predispose to lung injury Vit A & E prevent lipid peroxidation & maintain cell integrity Extreme prematurity – large amounts of H2O needed to compensate loss from thin skin

20
Nutrition Increased fluid administration increased risk of development of PDA & pulmonary edema(PE) High vent settings & high O2 needed to Rx PDA & PE Early PDA Rx – improve pulmonary function but no effect on incidence of BPD
 High vent settings & high O2 needed to Rx PDA & PE Early PDA Rx – improve pulmonary function but no effect on incidence of BPD")
21
Genetics Strong family history of asthma & atopy increase risk of development & severity of BPD

22
CVS Changes Endothelial cell proliferation Smooth muscle cell hypertrophy Vascular obliteration Serial EKG – right ventricular hypertrophy Echocardiogram – abnormal right ventricular systolic function & left ventricular hypertrophy

23
CVS Changes Persistent right ventricular hypertrophy/ fixed pulmonary hypertension unresponsive to supplemental O2 leads to poor prognosis

24
Airway Trachea & main stem bronchi - abnormalities depend on duration & frequency of intubation & ventilation Diffuse or focal mucosal edema, necrosis/ulceration occur Earliest changes from light microscopy loss of cilia in columnar epithelium, dysplasia/necrosis of the cells

25
Airway Neutrophils, lymphocyte infiltrate & goblet cell hyperplasia increased mucus production Granulation tissue & upper airway scarring from deep suctioning & repeated ET intubation results in laryngotracheomalacia, subglottic stenosis & vocal cord paralysis

26
Airway Necrotizing bronchiolitis – results from edema, inflammatory exudate & necrosis of epithelial cells. Inflammatory cells, exudates & cellular debris obstruct terminal airways Activation & proliferation of fibroblasts peribronchial fibrosis & obliterative fibroproliferative bronchiolitis

28
Radiologic Findings Decreased lung volumes Areas of atelectasis Hyperinflation Lung haziness PIE

30
Histologic Findings In 1996 Cherukupalli & colleagues described 4 pathologic stages Acute lung injury Exudative bronchiolitis Proliferative bronchiolitis Obliterative fibroproliferative bronchiolitis

33
Medical care in BPD Prevention Mechanical ventilation O2 therapy Nutritional support Medications

34
Mechanical Ventilation O2 & PPV life saving Aggressive weaning to NCPAP eliminate need of PPV Intubation primarily for surfactant therapy & quickly extubation to NCPAP decrease need for prolong PPV If infant needs O2 & PPV gentle modes of ventilation employed to maintain pH 7.28 – 7.40, pCo2 45 – 65, pO2 50- 70

35
Mechanical Ventilation Pulse oximetry & transcutaneous Co2 mesurements – provide information of oxygenation & ventilation with minimal patient discomfort SIMV – provide information on TV & minute volumes which minimize O2 toxicity & barotrauma/volumetrauma SIMV – allow infant to set own IT & rate

36
Mechanical Ventilation When weaning from vent & O2 difficult – when adequate TV & low FiO2 achieved trial of extubation & NCPAP Commonly extubation failure secondary to atrophy & fatigue of respiratory muscles Optimization of nutrition & diuretics – contribute to successful weaning from vent Meticulous nursing care – essential to ensure airway patency & facilitate extubation

37
O2 Therapy Chronic hypoxia & airway remodeling pulmonary HT & cor pulmanale O2 stimulate production of NO smooth muscle relaxation vasodilatation

38
O2 Therapy Repeated desats secondary to hypoxia results from- decreased respiratory drive - altered pulmonary mechanics - excessive stimulation - bronchospasm Hyperoxia worsen BPD as preterms have a relative deficiency of AO

39
O2 Therapy O2 requirement increase during stressful procedures & feedings therefore wean O2 slowly Keep sats 88% - 92% High altitudes may require O2 many months PRBC transfusion increase O2 carrying capacity in anemic(hct<30%) preterms
 preterms")
40
O2 Therapy Study in 1988 found increased O2 content & systemic O2 transport, decreased O2 consumption & requirement after blood Tx Need for multiple Tx & donor exposures decreased by erythropoetin, iron supplements & decreased phlebotomy requirements

41
Nutritional Support Infant with BPD- increased energy requirements Early TPN – compensate for catabolic state of preterm Avoid excessive non N calories increase CO2 & complicate weaning Early insertion of central lines maximize calories in TPN

42
Nutritional Support Rapid & early administration of increased lipids worsen hyperbillirubinemia & BPD through billirubin displacement from albumin & pulmonary vascular lipid deposition respectively. Excessive glucose load increase O2 consumption, respiratory drive & glucoseuria.

43
Nutritional Support Cu, Mn, & Zn essential cofactors in AO defenses Early initiation of small enteral feeds with EBM, slow & steady increase in volume facilitate tolerance of feeds Needs 120 – 150 Kcal/kg/day to gain weight

44
Medical Therapy Diuretics Systemic bronchodilators

45
Diuretics Furesemide (Lasix) Rx of choice Decrease PIE & pulmonary vascular resistance Facilitate weaning from PPV, O2 /both Adverse effects – hyponatremia, hypokalemia, hypercalciuria, cholelithiasis, nephrocalcinosis & ototoxicity
 Rx of choice Decrease PIE & pulmonary vascular resistance Facilitate weaning from PPV, O2 /both Adverse effects – hyponatremia, hypokalemia, hypercalciuria, cholelithiasis, nephrocalcinosis & ototoxicity")
46
Diuretics Careful parenteral & enteral supplements compensate adverse effects Thiazide & spiranolactone for long term Rx

47
Systemic Bronchodilators Methylxanthines – increase respiratory drive, decrease apnea, improve diaphragmatic contractility Smooth muscle relaxation – decrease pulmonary vascular resistance & increase lung compliance Exhibit diuretic effects

48
Systemic Bronchodilators Theophyline – metabolized primarily to caffeine in liver Adverse effects – increase heart rate, GER, agitation & seizures

49
Prognosis Pulmonary function slowly improves secondary to continued lung & airway growth & healing Northway- Airway hyperactivity, abnormal pulmonary functions, hyperinflation in chest x ray persists in to adult hood A study in 1990 found gradual decrease in symptom frequency in children 6 – 9 yrs

Similar presentations


















 Respiratory Distress Syndrome.>")
>")

