Download presentation
Presentation is loading. Please wait.

1
Endocrinology and Metabolism in Intensive care 馬偕醫院內分泌暨新陳代謝科 陳偉哲

2
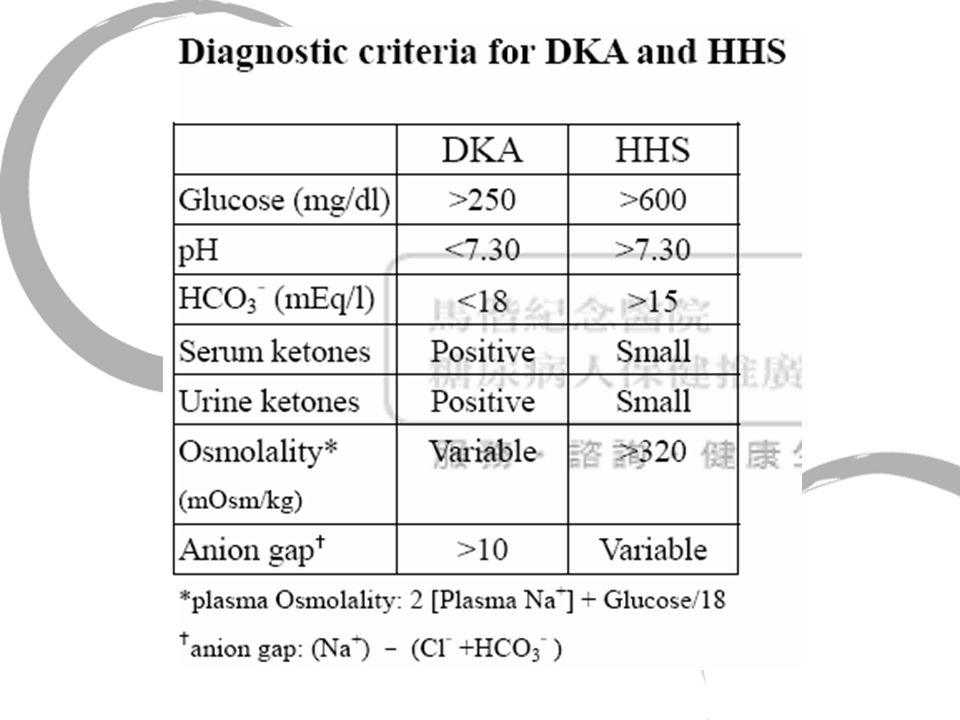
Hyperglycemia crisis

4
Hyperglycemia Crisis Management Hydration Insulin administration Monitor and keep electrolyte balance Correct metabolic acidosis?

5
Hyperglycemia crisis Do you run as fast as possible?

9
Hyperglycemia crisis Do you touch down?

11
Hyperglycemia Crisis Etiology DM control at usual Underlying disease and previous medication Predisposing factors

12
Intractable hyperglycemia in Intensive care Stress-related hormone act as insulin antagonistic hormones: cortisol, epinephrine, nor-epinephrine, glucagon. Hepatic glucose production is enhanced by an upregulation of both gluconeogenesis and glycogenolysis Insulin-stimulated glucose uptake by glucose transporter-4 (GLUT-4) is compromised Current Opinion in Critical Care 2005, 11:304—311
 is compromised Current Opinion in Critical Care 2005, 11:304—311.")
13
DM diagnosis Plasma glucose of 126mg/dl or greater Symptoms of diabetes and a random plasma glucose of 200mg/dl or greater Oral glucose tolerance test(OGTT)
")
14
DM diagnosis Diabetes mellitusDiabetes mellitus Hyperglycemia related to stressHyperglycemia related to stress Pre-diabetes: IGT(impaired glucose tolerance) and IFG (impaired fasting glucose)Pre-diabetes: IGT(impaired glucose tolerance) and IFG (impaired fasting glucose)
 and IFG (impaired fasting glucose)Pre-diabetes: IGT(impaired glucose tolerance) and IFG (impaired fasting glucose)")
15
What should you survey for an inpatient with DM Vital signs BH and BW Hemogram GluAC/PC, HbA1c Liver function: GOT/GPT, Bil.T/D Renal function: BUN/Cre Total cholesterol, triglyceride, LDL, HDL Urinalysis CxR EKG Skin and sensory

16
Continuous HRI IV infusion Critical condition Intractable hyperglycemia 以時間換取空間

17
Continuous HRI IV infusion Actrapid 100U in NS 100ml ivdrip by surestep(capillary blood sugarmonitering ) q4h - 啟始 run 2ml/hr, 而後劑量隨 surestep 增減 - surestep <70 ng/ml, 1) insulin ivdrip -0.5ml/hr, 2) D50W 2Amp iv stat and 3) 兩小時後補驗 surestep stat. 一次 - surestep 70~100 ng/ml, insulin ivdrip -0.5ml/hr - surestep 101~200, insulin ivdrip 不變 - surestep 201~300 ng/ml, insulin ivdrip +0.5ml/hr - surestep 301~400 ng/ml, insulin ivdrip +1ml/hr - surestep >= 401, insulin ivdrip +1ml/hour and insulin iv bolus 4U stat.

18
Euglycemia in ICU care A meta-analysis of myocardial infarction revealed an association between stress hyperglycemia and increased risk of in- hospital mortality and congestive heart failure or cardiogenic Lancet 2000; 355:773—778. Similarly, hyperglycemia predicted a higher risk of death after stroke and a poor functional recovery in patients who survived Stroke 2001; 32:2426—2432.

19
Euglycemia in ICU care Elevated glucose levels also predicted increased mortality and length of ICU and hospital stay of trauma patients and were associated with infectious morbidity Conclusions J Trauma 2003; 55:33—38. 2004; 56:1058—1062. Retrospective analysis of a heterogeneous population of critically ill patients showed that even a modest degree of hyperglycemia was associated with substantially increased hospital mortality contribute to these clinical benefits. In the past few years Mayo Clin Proc 2003; 78:1471—1478.

20
Mechanisms explaining the improved outcome with intensive insulin therapy Both glucose control and insulin dose contributed to the reduced inflammation, albeit with a superior effect of lowering glucose levels.

22
Definition of hypoglycemia Sometimes define as plasma glucose level <2.8 to 3.9mmol/L (<50 to 70mg/dl) Whipple triad: (1) symptoms of hypoglycemia (2) low plasma concentration (3) relief of symptoms after the plasma glucose raised From Willians 10 th
 Whipple triad: (1) symptoms of hypoglycemia (2) low plasma concentration (3) relief of symptoms after the plasma glucose raised From Willians 10 th")
23
Common Cause of hypoglycemia in ICU Drugs: Especially insulin, sulfonylureas, ethanol Sometimes pentamidine, quinine Rarely salicylates, sulfonamides, and others Critical illnesses Hepatic, renal, or cardiac failure Sepsis Starvation and inanition Postprandial Reactive (after gastric surgery) Ethanol-induced Autonomic symptoms without true hypoglycemia Factitious Insulin, sulfonylureas
 Ethanol-induced Autonomic symptoms without true hypoglycemia Factitious Insulin, sulfonylureas")
24
Hypoglycemia in Diabetes Insulin excess => Inadequate physiologic and counterregulatory and behavioral responses : hypoglycemia-associated autonomic failure (1) absolute insulin excess and absent glucagon response (2)reduce autonomic response (adrenomedullary epinephrine) (3) reduce symptom and hypoglycemia unawareness From Willians 10th
 absolute insulin excess and absent glucagon response (2)reduce autonomic response (adrenomedullary epinephrine) (3) reduce symptom and hypoglycemia unawareness From Willians 10th")
25
Thyrotoxic storm Thyrotoxic storm def : exaggeration of the clinical manifestation of thyrotoxicosis if left untreated, mortality range from 20% to 30 %

28
Predisposing factor

29
Clinical manefestation Fever Sinus tachycardia CNS symptomatology: agitation, restless, emotional lability to confusion GI disturbance: vomiting, diarrhea, intestinal obstruction, acute abdomen

30
Lab finding Serum total T4 and free T4 increase Mild hypercalcemia Hyperglycemia in some pts Hepatic dysfunction Leukocytosis with left shift

31
Treatment Reduction of the production/ secretion of thyroid hormone by the thyroid gland: 1. PTU 200~250mg q6h (addition block peripheral conversion of T4) or methimazole 20mg q4h 2. lugol’s solution (30 drops daily in 3 or 4 divided doses) or SSKI(8 drops every q6h) to decrease T4 synthesis 3. sodium ipodate or iopanoic acid- additional block /T4 to /T3 4. lithium carbonate 300mg po q6h to keep serum Li around 1mg/dl for allergy to thionamide or iodine
 or methimazole 20mg q4h 2. lugol’s solution (30 drops daily in 3 or 4 divided doses) or SSKI(8 drops every q6h) to decrease T4 synthesis 3. sodium ipodate or iopanoic acid- additional block /T4 to /T3 4. lithium carbonate 300mg po q6h to keep serum Li around 1mg/dl for allergy to thionamide or iodine.")
32
Treatment Inhibition of thyroid hormone peripheral action-administration of anti-adrenergic drug delpete catecholamine stores such as guanethidine or reserpine or block b- adrenergic receptor inderal 80~120mg q6h or 0.5~1mg iv bolus followed 1~3mg iv every several hrs administration of high doses cholecystyramine

33
Treatment Reverse of systemic disturbance: acetaminophen rather than aspirin ( inhibit thyroid hormone binding to globulin) ice pack fluid replacement
 ice pack fluid replacement")
34
Treatment Measure to remove or abrogate the effect of the precipitating factor treatment underly dx

35
Sick euthyroidism syndrome

37
Adrenal insufficiency Crisis Primary adrenal insufficiency? Secondary adrenal insufficiency? Acute? Chronic?

38
Adrenal insufficiency Crisis Hypotension Hypoglycemia Hypothermia Nausea, vomiting Epigastragia Hyponatremia

39
Adrenal insufficiency Crisis Check ACTH/Cortisol immediately Then given Dexamethsone 4mg q6h(Decardone 1AMp iv q6h) or Solucortef 1amp iv q12h to q6h
 or Solucortef 1amp iv q12h to q6h")
40
Thanks for your attention

Similar presentations









 Sepehr Khashaei, MD Assistant professor Department of Internal Medicine.>")







. 2 Hyperglycaemia Learning objectives >Can state what hyperglycaemia is >Is aware of the short term and.>")







 state>")
 Placebo group (n=2634)HR (95% CI)p Composite primary.>")
