Download presentation
Presentation is loading. Please wait.

1
Assist prof. of Medical Physiology

3
Thyroid gland activity is regulated by: 1. Plasma level of TSH 2. Thyroid stimulating immunoglobulin (TSI) 3. Stress conditions: ↑thyroid activity 4. Age: ↓ activity of thyroid gland. 5. Pregnancy : ↑thyroid activity 6. Antithyroid agents (Goitrogens) 7. Blood iodine level
 3. Stress conditions: ↑thyroid activity 4. Age: ↓ activity of thyroid gland. 5. Pregnancy : ↑thyroid activity 6. Antithyroid agents (Goitrogens) 7. Blood iodine level.")
4
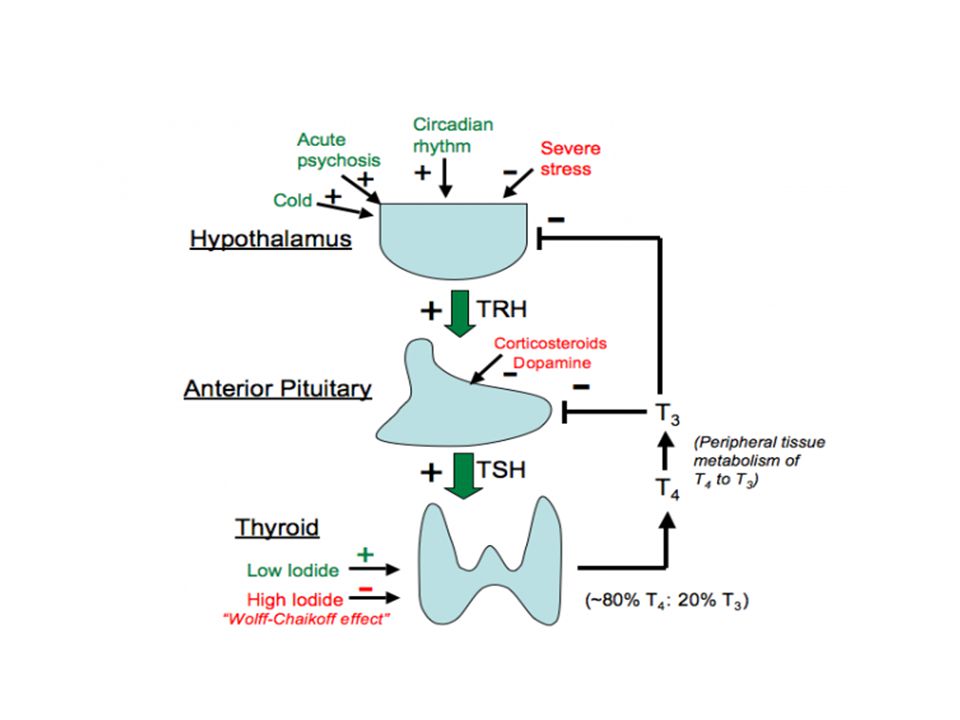
+ Hypothalamus Ant Pituitary Thyroid gland Short loop -ve feed back _ TRH + TSH T3 and T4 _ long loop -ve feed back

5
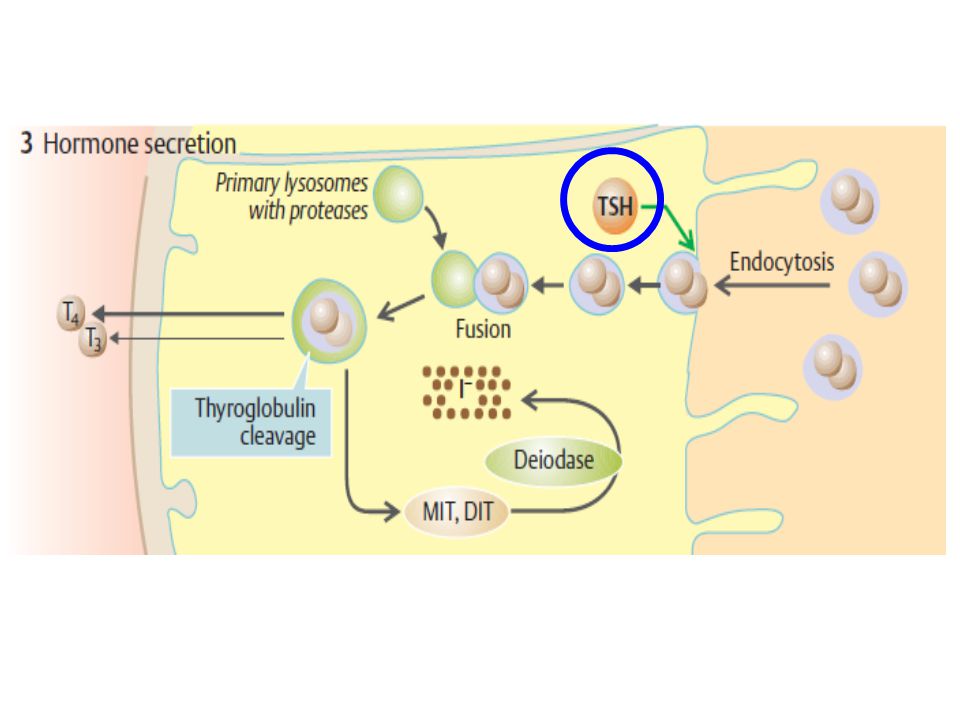
TSH has the following effects on the thyroid gland: a.Promote hyperplasia of the follicular cells. b.Increase iodide uptake of from the blood. c.Stimulates synthesis & release of T3 & T4.

8
Negative feedback between T3 and T4 and TSH secretion. Excess T3 and/or T4 suppresses the release of TSH by acting on the thyrotrop cells, more than on the anterior hypothalamus (site of release of TRH). The feedback mechanism controlling thyroid gland activity act mainly on the ant pituitary.
. The feedback mechanism controlling thyroid gland activity act mainly on the ant pituitary..")
9
Hypothalamic control of thyroid gland.

10
–known as ‘long acting thyroid stimulator’ (LATS). produced by lymphocytes in all cases of Grave’s disease (autoimmune disorder leads to hyperthyroidism). –TSI acts on the thyroid similar to TSH –but –Has is no –ve feed back to increased T3 and T4.
. –TSI acts on the thyroid similar to TSH –but –Has is no –ve feed back to increased T3 and T4..")
12
They enhance thyroid activity: e.g. –Exposure to cold –Increase the thyroid activity: that increase BMR and heat production –to –counteract the effects of low temperature.

14
This effect is small Activity of thyroid gland tends to decrease with increasing age.

15
Thyroid activity increases during pregnancy. The placenta secretes a hormone called ‘human chorionic gonadotropin’ or hCG which is structurally similar to TSH.

16
–Primary Goitrogens include thiocyanates : found in cabbage that inhibit I- uptake. Interfere with T3 and T4 synthesis. – T4 & T3 level leads to TSH level which results in enlargement of the thyroid gland ( goiter ).
..")
17
–a) Iodine deficiency: decreased T3 & T4 formation TSH goiter. –b) Excess iodine (Wolff– Chaikoff) results in: 1- Decrease in organic binding of iodine in the gland. 2- Inhibition of TSH effect on the gland by ↓ cAMP response to it. 3- Decreased proteolysis of thyroglobulin.
 Excess iodine (Wolff– Chaikoff) results in: 1- Decrease in organic binding of iodine in the gland. 2- Inhibition of TSH effect on the gland by ↓ cAMP response to it. 3- Decreased proteolysis of thyroglobulin..")
21
Excess Thyroid Secretion Decreased Secretion (Hypothyroidism) Hyperthyroidism or thyrotoxicosis In children Cretinism In adults Myxoedema
 Hyperthyroidism or thyrotoxicosis In children Cretinism In adults Myxoedema")
22
Cause: may be 1.Primary (thyroid defect) or 2.Secondary (defect in the pituitary gland). Manifestations vary according to the age : 1.Cretinism : Hypothyroidism in infants. 2.Myxoedema : Hypothyroidism of adults.

23
Def Hypothyroidism in infants. May not recognized until 5-6 months after birth (Some thyroid hormones reach the infant through milk from his mother). Clinical features a)Growth Retardation: physical, mental & sexual. The cretin is dwarf. b) Low BMR (Cold intolerance) and O2 consumption.
. Clinical features a)Growth Retardation: physical, mental & sexual. The cretin is dwarf. b) Low BMR (Cold intolerance) and O2 consumption..")
25
c) The skin is: –Yellowish, scaly –Scanty coarse hair, due to failure of formation of vitamin A in the liver from carotins. –The resulting carotinaemia gives the yellowish skin.

26
d) Facial features: –Dull, uninterested expression and puffy eye lids. –Thick protruded tongue ( macroglossia ).
..")
27
e) Abdomen is protuberant (potbelly) and umbilical hernia.
 Abdomen is protuberant (potbelly) and umbilical hernia.")
28
Cretinism: puffy eyelids, depressed nose, disproportionate dwarfism

29
Treatment: Should be started as early as possible –by giving thyroid hormones, –because mental retardation, once developed, is irreversible.

30
Def. Hypothyroidism in adults Manifestations: Characterized by: a) Retardation of all mental functions e.g. lack of concentration, slow thinking, long reflex time and sleepiness. b) Low BMR & O2 consumption leads to: Weight gain. Increased sensitivity to cold weather (cold intolerance) c) Bradycardia & hypotension.
 Retardation of all mental functions e.g. lack of concentration, slow thinking, long reflex time and sleepiness. b) Low BMR & O2 consumption leads to: Weight gain. Increased sensitivity to cold weather (cold intolerance) c) Bradycardia & hypotension..")
31
Myxoedema: puffy face, generalized fatigued appearance

33
d) Skin changes: –Thick doughy Skin: due to deposition of myxoedematus tissue in SC. –Pale Skin due to: iron deficiency anaemia and compression of cutaneous BV by the deposited SC myxoedematus tissue. –Yellowish due to carotinaemia. –Cold due to decreased BMR. –Dry scaly & brittle hair (vitamin A deficiency).
..")
34
f) Failure of sexual functions e.g. –Impotence in the male and –Menstrual disturbances in the female, mainly oligomenorrhea. e) Increased level of cholesterol & triglycerides Treatment by giving thyroid hormones.
 Increased level of cholesterol & triglycerides Treatment by giving thyroid hormones..")
36
Def., Hyperthyroidism or thyrotoxicosis Causes: Due to 1.Thyroid tumour or 2.Over stimulation of the thyroid by TSH or TSI.

37
Clinical features: a) Excessive nervousness and irritability with insomnia and tremors of hands. b) Loss of weight inspite of Increased appetite. –Increased catabolism of tissue proteins and oxidation of the stored fat c) Warm moist skin, and Fine silky hair.
 Loss of weight inspite of Increased appetite. –Increased catabolism of tissue proteins and oxidation of the stored fat c) Warm moist skin, and Fine silky hair..")
38
Clinical features d) Low serum cholesterol level. e) Increased BMR and O2 consumption –Body temp is not raised as the extra heat is lost by excess sweating. –Hot intolerance and prefer cold weather.
 Increased BMR and O2 consumption –Body temp is not raised as the extra heat is lost by excess sweating. –Hot intolerance and prefer cold weather..")
39
f) Ocular signs: include Sympathetic overstimulation causes 1.Stare look. 2.Infrequent blinking. 3.Lid lag phenomenon. 4.Failure of convergence. 5) Exophthalmos (protrusion of eye balls): due to; a.Exophthalmos producing factor (a degradation product of TSH) b.Accumulation of fat, water and inflammatory cells in the retro- orbital tissue and extra ocular ms.
 Exophthalmos (protrusion of eye balls): due to; a.Exophthalmos producing factor (a degradation product of TSH) b.Accumulation of fat, water and inflammatory cells in the retro- orbital tissue and extra ocular ms..")
40
Ocular signs 1-Characteristic stare due to upward retraction of upper eye lid.

41
2-Lid lag phenomenon i.e a delay in the downward movement of the upper eye lid on following a falling object. 3-Failure of convergence. Ocular signs

42
4- Infrequent blinking. 5- Exophthalmos Ocular signs

44
g) Tachycardia, atrial arrhythmias (as AF) –High systolic pressure. –Diastolic pressure is not raised due to peripheral VD. –So There is high pulse pressure.

45
h) Rapid ms fatigue due to reduced ATP synthesis. i) Sexual disturbances –Impotence in males and –Menstrual disturbances in the female. polymenorrhea menorrhagia
 Sexual disturbances –Impotence in males and –Menstrual disturbances in the female. polymenorrhea menorrhagia.")
47
Goiter

49
Def., It is enlargement of the thyroid gland. It is accompanied by either hypo, or hyperfunction. Causes 1. Goitrogens: –Substances that block synthesis of thyroid hormones, –e.g. thiocyanates and thiocarbamides. –They lead to T3 & T4 TSH gland size. 2. Iodine deficiency – T3 & T4 TSH goiter. –Called colloid goiter, the acini distended with colloid.

50
3. Grave’s disease: – due to TSI which binds to TSH receptors on thyroid cells diffuse goiter. 4. Nodular goiter: –Irregular enlargement of the thyroid with varying numbers of discrete nodules, –due to exposure to stresses. 5. Physiological goiter –Sometimes noticed in adolescence and during pregnancy.

51
Goiter: (enlargement of the thyroid gland)
")
Similar presentations
















 Hypothalamic control hGH releasing hormone hGH.>")


 Triiodothyronine (T3) T4 and T3 regulate body metabolism.>")
 Triiodothyronine (T3) Calcitonin Energy & Growth Control.>")











