Download presentation
Presentation is loading. Please wait.

1
Peripheral angioplasty Overview, Hardware
Frijo Jose A

2
Vascular Access Relatively disease-free, without signi Ca
Over a bony structure, if possible Angle of entry- 30⁰-45⁰ If access vessel-small/potentially diseased- micropuncture tech preferred

3
Vascular Access sites Retrograde Common Femoral Artery Access Common access site used for peripheral diagnostic angiography and intervention Prevent injury to the less diseased extremity

4
Vascular access sites Contralateral femoral retrograde access :
Internal iliac stenoses are best treated from a contralateral approach SFA,PFA- lesions located within the CFA/involve SFA/PFA ostium - Proximity to arterial puncture site, Bifurcation anatomy of CFA Also allows treatment B/L disease with a single arterial puncture

6
Vascular Access site Required for infrainguinal proced
Antegrade Common Femoral Artery Access: Required for infrainguinal proced Approx 3cm CFA lies betw ligament & FA bifurcation Inorder to access CFA, skin entry- prox to ing ligm Access too close to F bifurc –inadeq working room to selectively cath SFA

7
Vascular access sites Ipsilateral popliteal retrograde access:
Useful in SFA occlusion with failure to cross from contralateral or antegrade Ostial SFA/CFA lesions may also be approached via PA in acute angled terminal ao bifurc CI- aneurysms of PA, pathology of popliteal fossa- Baker’s cyst

8
Brachial Artery Access
Pref access for visc arterial [CA, SMA] interventions PC approach at BA can lead to a ↑compli rate UL arts – smaller, prone to spasm A small hematoma- Could lead to brachial plexopathy Itv req >6F sheaths/smaller pt→open approach preferred Left BA access pref over Rt- can avoid carotid origin A micropuncture tech should be used for all PC BA intervention

9
Wire selection Many-Teflon/silicone :Some- hydrophilic
Hydr-stenosd/torturous+angle tip–Glidewire Can be used for crossing tight lesions and can be advanced independent of a guidewire 014,018,025,035,038-for initial access, 038:18g needle, 018:21g needle

10
Estimated distances from FA access

11
Guidewire-Lesion Interaction
Floppy portion moving in a linear Floppy portion piles up prox to lesion—no chance to cross- backup,redirect,if straight tip→steerable Floppy tip bent with min R—Cautiously adv wire- once crossed, wire should straighten- advancing a “buckledup” wire- force→embolization Floppy tip “buckledup” with R—backup,redirect,adv -dissect,embolz,wire damag

12
Catheter ( diagnostic/ guiding)
Length depends on location for using a) abdominal aorta = 60 to 80 cm length b) BTK,carotid or subclavian areas 100 to 125cm length Polyethylene- ↓coef friction, pliable Polyurethane- softer, even ↑pliable→ tracks wires better Nylon- stiffer, can tolerate ↑flow rate- amenable to angio Teflon- stiffest- used mainly for dilators & sheaths
 abdominal aorta = 60 to 80 cm length. b) BTK,carotid or subclavian areas 100 to 125cm length. Polyethylene- ↓coef friction, pliable. Polyurethane- softer, even ↑pliable→ tracks wires better. Nylon- stiffer, can tolerate ↑flow rate- amenable to angio. Teflon- stiffest- used mainly for dilators & sheaths.")
13
▫ ▫

15
▫ ▫ ▫ ▫ ▫ ▫

18
4F IMPRESS Simmons 1 Catheter 65cm..038
Side Ports:N/A Catheter Shape:SIMMONS 1 French Size:4

19
5F IMPRESS Simmons 2 Catheter 65cm..038
Side Ports:N/A Catheter Shape:SIMMONS 2 French Size: 5

20
SOS Omni selective catheter
Soft, atraumatic, Super-radiopaque tip Reforming in desc thoracic aorta – below great vessels rather than transverse arch –safety The catheter should be pulled from the desc ao into abd ao with a floppy guidewire “leading,” sometimes with a rotating motion The soft, flexible atraumatic tip can be placed deeper into the artery (>1 cm), ↓chance of “catheter kickout.” The shaped tip allows the guidewire to flick into the origin of the RA
, ↓chance of catheter kickout. The shaped tip allows the guidewire to flick into the origin of the RA.")
21
Omni Flush Angiographic Catheter
Designed as a single catheter to perform flush aortography, B/L“run off” studies of lower extremities and to cross ao bifurcation with ease for C/L diagnostics in interventional procedures. Super-Radiopaque tip Reforms and maintains shape—even under injection pressure—with less catheter whipping, resulting in less vessel wall injury Less contrast reflux than other flush catheters, thus resulting in lower total contrast dose

22
Brachiocephalic Artery 1. Head Hunter 1 2. Sidewinder 1 3. Weinberg 4
Brachiocephalic Artery 1. Head Hunter 1 2. Sidewinder 1 3. Weinberg 4. Berenstein L and R External Carotid Artery 3. Hockey Stick 1 4. Weinberg 5. Berenstein 6. Sidewinder 2 L and R Internal Carotid Artery 5. Headhunter 3 L and R Subclavian Artery 1. Berenstein 2.Head Hunter 1 L and R Vertebral Artery 3. Vertebral L and R Common Carotid Artery 1. Head Hunter 1 2. Sidewinder 1 3.Weinberg 4. Berenstein 5. Vertebral 6. Head Hunter 3

23
Descending Aorta 1. Omni Flush 2. Pigtail Flush 3
Descending Aorta 1. Omni Flush 2. Pigtail Flush 3. Straight Flush Ascending Aorta Thoracic Aorta Abdominal Aorta L and R Renal Artery 1. Sos Omni 1 2. Sos Omni 2 3. Cobra 1 4. MPA

24
L and R Common Iliac Artery 1. Sos Omni 1 2. Sos Omni 2 3. Cobra 1 4
L and R Common Iliac Artery 1. Sos Omni 1 2. Sos Omni 2 3. Cobra 1 4. Berenstein L and R Internal Iliac Artery 1. Sos Omni 1 L and R External Iliac Artery 3. Berenstein L and R Common Femoral Artery 5. MPA L and R Deep Femoral Artery 1. Sos Omni 1 2. Sos Omni 2 3. Berenstein L and R Popliteal Artery 1. Berenstein 2. Straight Art L and R Anterior Tibial Artery L and R Posterior Tibial Artery L and R Peroneal Artery

25
Accesses and Selective Guiding Catheters for Some Basic Interventions

26
Carotid Artery Subclavian Artery Celiac or SMA
1.First choice access—either FA 2.Alternative access—left BA 3.Selective catheter— Right carotid: H1,Simmons,Vick; Left carotid : angled glidecath,H1,Simmons Subclavian Artery 1.First choice—either FA 2.Alternative access—ipsilateral BA 3.Selective catheter– angled Glidecath,H1,Simmons,H3 Celiac or SMA 3.Selective catheter—RIM,Chuang-C,Chuang-3

27
Superior Femoral Artery
Renal Artery 1.First choice—contralateral FA 2.Alternative access—left BA 3.Selective catheter—C2,RDC,Sos-omni Infrarenal Aorta 1.First choice —either FA 3.Selective catheter—omni-flush,RIM,C2 Superior Femoral Artery 2.Alternative—ipsi retro FA for run-off; ipsi antegrade for interv 3.Selective catheter—Berenstein,Kumpe,Vertebral Tibial Arteries 3.Selective catheter—Kumpe,Vertebral

28
Kumpe catheter

32
Guiding Catheter vs Sheath
The use of a guide or sheath is determined by operator bias Sheaths are designed with a simple diaphragm or a hemostatic valve, guiding catheters always require hemostatic valves be attached During intervention, the guide catheter or sheath should be placed near the lesion to provide for better visualization and improved support

34
Balloons In selecting a balloon, the following criteria should be considered: a) Guidewire ( 0.014“, 0.018“, 0.035“) b) over the wire (OTW) or monorail system c) shaft length 0.014“ balloon system is usually for carotid, vertebral, renal, infrapopliteal arteries 0.035“ balloon system for subclavian, innominate, aortoiliac, superficial femoral artery 0.018“ balloon system also in SFA, infrapopliteal, depends on what the operator prefers
 over the wire (OTW) or monorail system. c) shaft length balloon system is usually for carotid, vertebral, renal, infrapopliteal arteries balloon system for subclavian, innominate, aortoiliac, superficial femoral artery balloon system also in SFA, infrapopliteal, depends on what the operator prefers.")
35
Law of Laplace Circumfer force/tension (T) exerted on wall of an inflatd balln ~P within balln & R (T=P×R) Balln twice R of a smaller balln- twice wall T for given inflation P→D kept constant, T on wall of balln will ↑linearly with ↑inflatn P Larger ballns -require ↓P than smaller ballns to generate substantial dilating forces Larger vessels (Ao) require ↓P to dilate & rupture
 require ↓P to dilate & rupture.")
36
Balloon cath with a D matchng outflow vessel beyond lesion
Balloon length should be > lesion Balloon centered on lesion & inflated slowly Inflation maintained for 20s- deflated- reinflated 3 inflations of 20s

37
Subintimal angioplasty
Hydrophilic wire not passng Carefully adv into subintimal plane- if not spontaneously, gentle inflation of balloon at edge of the plaque Wire traversed the lesion subintimaliy Hydrophilic catheter or other re-entry device passed OTW to guide it back into lumen Standard angioplasty of subintimal plane performed, with stent placement

38
Femoropopliteal Artery Intervention
Subintimal angioplasty

39
Stents The types of stent used in peripheral interventions:
Balloon-expandable Self-expandable Stent graft

40
Balloon-expandable stents
Require positive pressure for expansion Typically rigid with high radial force Size of the balloon-expandable stent equals to the size of the reference vessel diameter Ideal for immobile parts of the body-ie, subclavian, renal, mesenteric, iliac arteries and at ostial locations

41
Self-expandable Stents
Deployed in vessels that are flexible or twist during movement of neck, shoulder or leg carotid, axillary, superficial femoral artery, popliteal artery Nitinol - best flexibility and memory Stent compressed over a delivery cath & covered with sheath Stent deployment achieved by pulling back the sheath Stent diameter should be 1-2mm > ref vessel D→ adeq stent apposition

42
Self-expandable Stents
Some degree of foreshortening- to be taken into account when choosing More difficult to place with absolute precision Generally comes in longer length than BES Their ability to continually expand after delivery allows them to accommodate adjacent vessels of different size

43
Stents Demonstrating the Nitinol self-expandable stent deployment

44
Stent Grafts Used to exclude aneurysm, treat perforations when prolonged balloon inflation failed Wallgraft and Viabahn are two options

45
Decision between SE or BE stents in Iliac Lesions
Balloon expandable Aortoiliac bifurcation Common iliac Calcified lesions Chronic occlusions (?) Self expanding Vessels flexible/twist during movement Tortuous vessels Distal external iliac artery Contralateral approach Long diffuse lesions Aortoiliac bifurcation (long lesions)
 Self expanding. Vessels flexible/twist during movement. Tortuous vessels. Distal external iliac artery. Contralateral approach. Long diffuse lesions. Aortoiliac bifurcation (long lesions)")
46
Techniques Retrograde Iliac stent placement

47
Techniques Cross-over technique

48
A patient’s complaint of low back pain during balloon inflation may be a warning sign of adventitial stretch, which may occur before aortic rupture

49
Femoropopliteal Artery Intervention
Balloon size & length matched to the size ( ~5-6mm) & lesion length( ~ mm) of SFA ↑ angiographic results may be accomplished with prolonged inflation times ( 3-5 minutes) Dissections are commonly seen after balloon dilation ( due to heavy calcification)
 & lesion length( ~ mm) of SFA. ↑ angiographic results may be accomplished with prolonged inflation times ( 3-5 minutes) Dissections are commonly seen after balloon dilation ( due to heavy calcification)")
50
Femoropopliteal Artery Intervention
Stentimplantion ( always SX-Stents): Sizing the SX- stent ~ 1mm > SFA Postdilation with mm diameter balloon Popliteal artery -> avoid stent = high risk of stent compression or fracture
: Sizing the SX- stent ~ 1mm > SFA. Postdilation with mm diameter balloon. Popliteal artery -> avoid stent = high risk of stent compression or fracture.")
51
Infrapopliteal Interv
Knee-to-foot patency of one of the three branches is usually sufficient to prevent critical lower-limb ischemia Claudication is rarely the result of isolated disease of the infrapopliteal arteries Re-stenosis after intervention in these vessels is typically the highest among the lower limb sites Obstructive disease in these arteries is often occlusive, diffuse and complicated by heavy calcific deposits

52
Infrapopliteal Interv- wire selection
Only atraumatic 0.014“ / 0.018“ guide wires should be used-0.014“ prefered due to vessel diameter Type selection ( floppy, medium,stiff) will be driven by the type of disease
 will be driven by the type of disease.")
53
Infrapopliteal -Balloon Angioplasty
Low profile balloon with high pushability and trackability to easy cross the lesion Flexibility in small collateral branches 0.014”/ 0.018" wire compatibility Diameter 1.5mm-4.0mm Long ( mm) to reduce procedure times and dissection
 to reduce procedure times and dissection.")
54
Infrapopliteal- Balloon Angioplasty
Long balloons (210mm/ tapered) Reduced risk of dissections ( no balloon overlap) Total intervention /revascularization time significantly shorter Reduced X-ray dose for patients, operators as well as for the assistants
 Reduced risk of dissections. ( no balloon overlap) Total intervention /revascularization. time significantly shorter. Reduced X-ray dose for patients, operators. as well as for the assistants.")
55
Renal artery stenosis Usually occurs in the proximal 2 cm
~75% of lesions are caused by atherosclerosis Lesions can be single or multiple, unilateral or bilateral (~25%) Diameter: mm for men mm for women Length 3-7 cm Discuss plaque in aorta – draw
 Diameter: mm for men mm for women. Length 3-7 cm. Discuss plaque in aorta – draw.")
56
Renal artery-Equipment
Diagnostic Wires 0.035” for catheter placement Diagnostic catheter Intervention Wires 0.014” 0.035” for catheter placement Guiding Sheath Guide Catheter Balloons ( 0.014” compatible) Low profile Undersized for pre-dilation BE-Stents
 Low profile. Undersized for pre-dilation. BE-Stents.")
57
Reanal artery stenting
1. Catheter or sheath placement 2. Guide wire (0.014“) insertion. Rosen wire has soft curled end- ideal- prevents perforating small renal branch vessels 3.Stent placement -> as soon as the tip reach the lesion GC is pulled back into the Aorta 4.Stent deployment, proximal struts should protrude 1-2mm into the aorta 5. Flaring the ostium of the stent ( optional), opens the way for re-intervention and covers the plaque in the aorta
 insertion. Rosen wire has soft curled end- ideal- prevents perforating small renal branch vessels 3.Stent placement -> as soon as the tip reach the lesion GC is pulled back into the Aorta 4.Stent deployment, proximal struts should protrude 1-2mm into the aorta 5. Flaring the ostium of the stent ( optional), opens the way for re-intervention and covers the plaque in the aorta")
58
Subclavian PTA Femoral access used except for TO/severely angulated – BA preferred LSCA – FA- direct take-off : RSCA because of its angulated take-off from inno A- ipsi BA Ostial RSCA, FA can protect the right CCA Total occlusions- combined approach Usually pre-dilated with a slightly undersized balloon BES sized 1:1 with ref D Ao-ostial lesions - stent protrude (1–2mm) into Ao BES - Ao-ostial locations SES- long segment/more flexibility needed/lesions beyond IMA→external compression
 into Ao. BES - Ao-ostial locations. SES- long segment/more flexibility needed/lesions beyond IMA→external compression.")
59
COOK

60
Catheters Slip-Cath Beacon Tip Catheters
Beacon Tip Torcon NB Advantage Caths Torcon NB Advantage Catheters CXI Support Catheters Beacon Tip Royal Flush Plus High-Flow Catheters Royal Flush II Nylon Catheters
![]()
61
Slip-Cath Beacon Tip Catheters
Hydrophilic Coating Enhanced radiopaque Beacon tip Sixteen stainless steel wire braid imparts 1:1 torque control to catheter tip & ↑pushability Nylon material resists softening during prolonged catheter manipulation
![]()
62
Slip-Cath Beacon Tip Catheters
![]()
63
Beacon Tip Torcon NB Advantage Caths
Enhanced radiopaque Beacon tip Gradual transition of radiopaque Beacon tip to catheter shaft Sixteen stainless steel wire braid Nylon material
![]()
64
Torcon NB Advantage Catheters
Sixteen stainless steel wire braid Nylon material Short, flexible atraumatic catheter tip

66
Beacon Tip Royal Flush Plus High-Flow Catheters
Royal Flush II Nylon Catheters
![]()
67
CXI Support Catheters For use in small vessel/superselective anatomy for diagn & interv procedures, incl peripheral use Low profile from tip to hub ensures smooth transition through small vessels Shaft's polymer material offers desired flexibility Braided SS entire length -pushability Hydrophilic coating Embedded radiopaque markers -size the vessel segment length

69
ATB ADVANCE PTA Dilatation Catheter
Advance 14LP Advance 18LP Advance 35LP

70
ATB ADVANCE PTA Dilatation Catheter
Designed for iliac, renal, popliteal, infrapopliteal, femoral and iliofemoral Also intended for postdilatation of balloon-expandable peripheral vascular stents 40,80,120

71
Advance 14LP Low Profile Provides the trackability and pushability to reach even the most remote infrapopliteal lesions Hydrophilic coating on balloon and distal shaft, along with a smooth tip transition Maintains super-low profile after inflation 4 Fr sheath compatibility for all sizes 20 to 200 mm in 2, 2.5, 3, 4 mm D 170

72
Advance 18LP Low Profile PTA Balloon Dilatation Catheters
Super-flexible tip Advanced rewrap technology 80,135

73
Advance 35LP first 8 mm x 8 cm 5 Fr sheath
Low-profile design tightly tapers to the wire Double-lumen D-shaped design allows rapid inflate/deflate 80,135

74
Amplatz Stiff Wire Guides
The wire guide has a stiff shaft and a gradual transition to a very flexible distal tip TFE Coated Stainless Steel-035,038: 145,180,260-straight TFE Coated Stainless Steel with Heparin Coating-035: 145,180,260-straight 8cm-flexi tip

75
Amplatz Extra-Stiff Wire Guides
The increased inner diameter of the wire guide coil allows utilization of an extra-stiff mandril while maintaining tip flexibility. TFE Coated Stainless Steel-025,035,038: 80,145,180,260-straight & curved: 300-straight TFE Coated Stainless Steel with Heparin Coating-035: 80,145,180,260-straight & curved

76
Amplatz Ultra-Stiff Wire Guides
The increased inner diameter of the wire guide coil allows utilization of an ultra-stiff mandril while maintaining tip flexibility. TFE Coated Stainless Steel-035,038: 80,145,180-straight TFE Coated Stainless Steel with Heparin Coating-035: 145,180-straight 8cm-flexi tip

77
Roadrunner Extra-Support Wire
Complex diagnostic/interventions where extra support needed for cath exchange/manipulation of devices Heavy-duty nitinol alloy mandril provides support while imparting 1:1 torque response to distal platinum spring coil tip Angled tip facilitates directional control Lubricious TFE coating -low coefficient of friction 014,018 180,270,300

78
Cope Mandril Wire Guides I
Stainless Steel Platinum coil ↑visualization and an angled floppy tip for precise directional control 018 40,60,100,125 Standard taper-7cm coil

79
Cope Mandril Wire Guides II
Nitinol mandril kink resistant and provides 1:1 torque control Platinum coil ↑visualization and an angled floppy tip for precise directional control 018 60,100,125 Standard taper-7cm coil, short taper-7cm coil

80
Rosen Curved Wire Guides
The heavy-duty mandril, 2 cm flexible tip and tightened “J” configuration TFE Coated Stainless Steel-035: 80,145,180,220,260 TFE Coated Stainless Steel with Heparin Coating-035: 145,180,260

81
The Graduate Measuring Wire Guides
Used to determine accurate sizing of vessel lumen prior Gold radiopaque markers delineate 25 cm in length for precise measuring accuracy. Six distal markers are spaced 1 cm apart. Four proximal markers are spaced at 5 cm increments. 035 145,180

83
Reuter Tip Deflecting Wire Guide
Used with Reuter Tip Deflecting Handle for curving or deflecting catheter tips during selective and superselective angiography Facilitates catheter tip movement by controlling the deflection of the wire guide tip within catheter lumen Distal tip of wire guide must never extend beyond tip

85
Double Flexible Tipped Wire Guides
Permits alternative use of both ends of wire guide, depending on procedural needs

86
Zilver 518 Vascular Self-Expanding nitinol Stent- iliac arteries
Recomm 5.0 Fr sheath/7.0 Fr guiding cath Accepts .018 inch wire

87
Zilver 518 RX Vascular Self-Expanding Nitinol Stent – Rapid Exchange-iliac Recommended 5.0 Fr sheath/7.0 Fr guiding catheter Accepts .018 inch diameter wire guide.

88
Zilver 635 Vascular Self-Expanding Nitinol Stent
Recommended 6.0 Fr sheath/8.0 Fr guiding catheter size Accepts .035 inch diameter wire guide

89
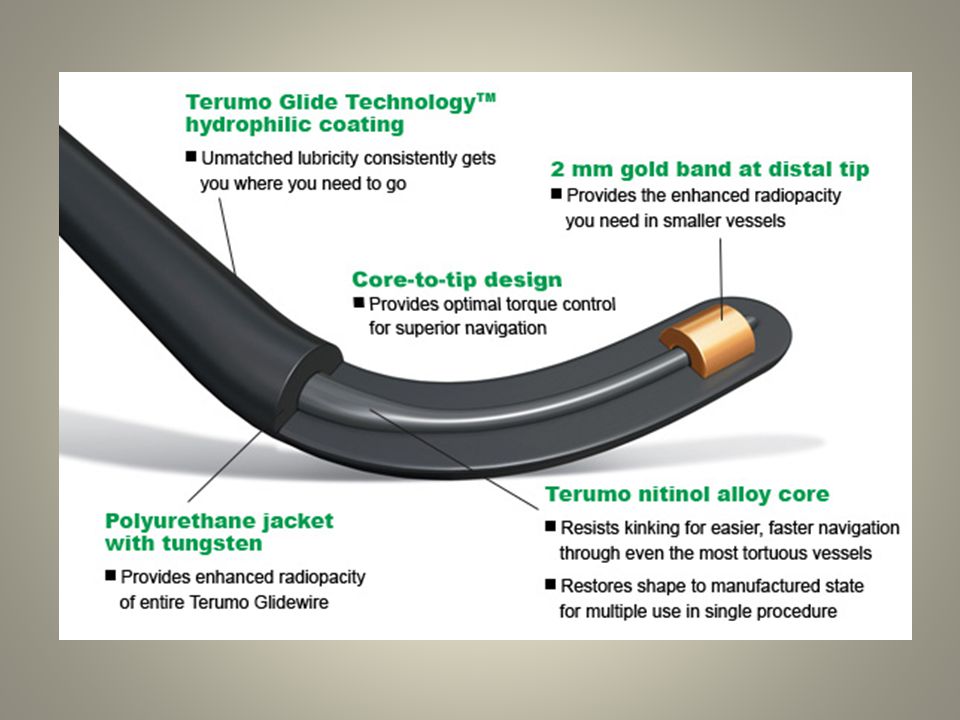
TERUMO

90
Guiding Sheaths (5-8 Fr) Pinnacle Destination
45,65,90 Hydrophilic coating All dilators are 0.038" wire compatible

92
glidewire Peripheral Guidewires (0.032"-0.038")
Standard Glidewire Shapeable Tip Glidewire Long Taper Glidewire Stiff Shaft Glidewire Stiff Shaft Long Taper Glidewire 1 cm Taper Glidewire J-Tip Glidewire Bolia Curve Glidewire Glidewire Advantage™ Small Vessel Guidewires (0.018"-0.025") Glidewire Standard and Shapeable Tip Glidewire GT Super-Selective Glidewire Gold
 Glidewire Standard and Shapeable Tip. Glidewire GT Super-Selective. Glidewire Gold.")
96
Hydrophilic Coated Catheters
Glidecath (4 Fr)-65,100, Glidecath XP (5 Fr)-65, (↑flow rate) Glidecath (5 Fr)-65,
-65,100, Glidecath XP (5 Fr)-65, (↑flow rate) Glidecath (5 Fr)-65,")
98
Microcatheters Progreat™ (2.4 Fr, 2.7 Fr)- 110/130- OD:0.97/0.9=2.9/2.7 -ID:0.57/0.65 Progreat™Ω (2.8 Fr)- 110/130- OD:1/0.93=3/2.8 -ID:0.7
- 110/130- OD:1/0.93=3/2.8 -ID:0.7.")
100
ABBOT

101
Veripath Peripheral Guiding Catheter
Three-Layer Construction 50 cm length 5 catheter shapes 6,7,8 F 014/018

103
Hi-Torque Steelcore Peripheral Guide Wire
Hi-Torque Spartacore Peripheral Guide Wire Hi-Torque Supra Core Peripheral Guide Wire Hi-Torque Versacore Guide Wire System

104
Hi-Torque Steelcore Peripheral Guide Wire

105
Hi-Torque Spartacore Peri Wire
Excellent .014" Support with Superb Steerability and a Soft Shapeable Tip Core-to-tip design High-support.014" stainless steel shaft MICROGLIDE Coating PTFE Coating up to distal 7 cm Available in 5 and 10 cm Intermediate Segment Lengths

107
Hi-Torque Supra Core Peri Wire
One-to-one torque response designed for exceptional steerability MICROGLIDE coating Radiopaque tip designed for visibility during guide wire placement 035" shaft Soft Shapeable tip

108
Hi-Torque Versacore Guide Wire
Torqueable wire for deliverability through tortuous or challenging lesions Soft shapeable tip designed to for lesion access

109
FoxCross .035 PTA Cath D-(3-14 mm), L-( mm), and cath L (50, 80 &135 cm)-OTW 50,80,135 5-7 F Guide wire compatibility: 035 Nylon Polymer JETCOAT coating

110
Fox sv PTA Catheter OTW designed for challenging small vessel procedures Range of BTK and SFA sizes (2-6 mm) 90,150 Sheath Compatibility:4F for all sizes Guide wire compatibility:.014"/.018"

111
Fox Plus PTA Catheter Low Profile
Compatible with a 5 French sheath up to 7mm balloons. Excellent rewrapping Shaft Technology-Adv shaft technology dual lumen - Rapid inflation and deflation JET coated shaft, tip and guidewire lumen. Reduces friction and facilitates access and crossing of target lesions

112
Jostent Peripheral Bare Stent System
SS Bare balloon-expandable stent Rec min sheath size: 1F >balloon Slotted tube with closed cell design Six in one: Every bare stent expandable to 6 different D Post-adjustment of stent size possible Standard version: 4-9 mm Large version: 6-12 mm Length: mm

113
Omnilink Elite Peripheral Stent System
Iliac compatibility with 6F sheaths across all sizes Cobalt Chromium

114
Absolute Pro LL Peripheral Self-Expanding Stent
035 designed to treat longer SFA lesions 120,150

115
Xpert Self-Expanding Stent
4F compatible -speci designed for small vessels Peri vessels from D 2-7 mm 018 Nitinol low strut profile Conformability

116
BOSTON SCIENTIFIC

118
Amplatz Super Stiff Guide Wire
For stiffness, strength and stability during catheter placement and exchange. Diameters: 0.035", 0.038" Lengths: 145cm,180cm, 260cm Tips Styles: Straight, J, Short Core Material: Stainless steel Coating: PTFE

119
Magic Torque Guide Wire
Magic Markers spaced at 1cm increments designed for enhanced visualization and excellent torque control to meet the challenges of difficult anatomy Diameters: 0.035" Lengths:180cm, 260cm Tips Styles: Straight (shapeable) Core Material: Stainless steel Coating: Glidex Hydrophilic Coating (tip)
 Core Material: Stainless steel. Coating: Glidex Hydrophilic Coating (tip)")
120
Meier Guide Wire Stiff shaft engineered for excellent support, while flexible tip is designed to reduce the risk of vessel trauma during diagnostic and interventional procedures including AAA endovascular graft procedures. Diameters: 0.035" Lengths: 185cm, 260cm, 300cm Tips Styles: J, C Core Material: Stainless steel Coating: PTFE

121
Platinum Plus Guide Wire
Designed for negotiation of tortuous anatomy and contralateral approaches. Also available in short taper configuration for access in anatomy with short distal Diameters: 0.014", 0.018", 0.025" Lengths (cm): 60, 145, 180, 260, 300 Tips Styles: Straight – Long or short taper Core Material: Stainless steel Coating: Glidex Hydrophilic
: 60, 145, 180, 260, 300. Tips Styles: Straight – Long or short taper. Core Material: Stainless steel. Coating: Glidex Hydrophilic.")
122
Thruway Guide Wire Designed for excellent performance in acutely angled vessels, such as renals and other peripheral interventions Diameters: 0.014", 0.018" Lengths (cm): 130, 190, 300 Tips Styles: Straight, J Core Material: Stainless steel Coating: Silicone
: 130, 190, 300. Tips Styles: Straight, J. Core Material: Stainless steel. Coating: Silicone.")
123
Sterling ES Balloon Dilatation Cath
0.014" balloon cath Ultra-low profile balloon Both OTW and rapid exchange platforms .017" tip entry profile 140

124
Sterling SL Balloon Dilatation Cath
now in long lengths for below-the-knee - specifically designed to meet the challenges of infrapopliteal procedures 014,018 available in both Over-the-Wire and Monorail platform 90,150

125
Sterling Balloon Dilatation Catheters
Breakthrough 4F Profile Both Over-the-Wire and rapid exchange 40,80,135 Specifically designed for use in renal and lower extremity arteries

126
Sterling Monorail Balloon Dil Cath
Breakthrough 4F Profile. carotid, renal and lower extremity 40,80,135

127
Renegade HI-FLO Microcatheter

128
Express LD Iliac Premounted Stent System
035

129
Express SD Renal Monorail Premounted Stent System
014/018 Low profile; 6F guide catheter-compatible up to 6.0mm

130
WALLSTENT Endoprosthesis
recapturable even when up to 87% deployed

131
CORDIS

133
EMERALD Guidewires Fixed-Core, PTFE Coated Wires 025,035,038 150,180

134
PTA Dilatation Catheters

135
PALMAZ Bal-Exp Stent (unmounted)
Closed cell SS Stent D (Expanded) 4-8mm Stent L (Unexpanded) 10,15,20,29,39mm Sheath Introducer 6F, 7F
 4-8mm. Stent L (Unexpanded) 10,15,20,29,39mm. Sheath Introducer 6F, 7F.")
136
Self-Ex: S.M.A.R.T. CONTROL Iliac
MicroMesh Geometry, Segmented Design Nitinol Stent D 6-10, 12, 14mm (should be 1-2mm >vessel D) 80,120 cm Maximum Guidewire .035" Sheath Compatibility 6F (6-10mm), 7F (12-14mm) Guide Compatibility 8F (6-10mm), 9F (12-14mm)
 80,120 cm. Maximum Guidewire .035 Sheath Compatibility 6F (6-10mm), 7F (12-14mm) Guide Compatibility 8F (6-10mm), 9F (12-14mm)")
137
Self-Ex: PRECISE Carotid Stent System
MicroMesh Geometry, Segmented Design Nitinol Stent D 5-10mm 135cm, Over-the-Wire Maximum Guidewire .018" Sheath Compatibility 5.5F (5-8mm diameters), 6F (9-10mm diameters) Guide Compatibility 7F (5-8mm diameters), 8F (9-10mm diameters)
, 6F (9-10mm diameters) Guide Compatibility 7F (5-8mm diameters), 8F (9-10mm diameters)")
138
Self-Ex: PRECISE PRO RX Carotid Stent
MicroMesh Geometry, Segmented Design Nitinol Stent Diameters 5-10mm 135cm, Rapid Exchange Maximum Guidewire .014" Sheath Compatibility 5F (5-8mm diameters), 6F (9-10mm diameters) Guide Compatibility 7F (5-8mm diameters), 8F (9-10mm diameters
, 6F (9-10mm diameters) Guide Compatibility 7F (5-8mm diameters), 8F (9-10mm diameters.")
139
OUTBACK Re-Entry Catheter
Enables fast, simple true lumen re-entry without need for IVUS Low profile, 6F sheath compatible Highly visible "L" and "T" markers- Orient re-entry cannula towards true lumen easily, eliminating need for IVUS

140
The cannula (large black arrow) is deployed and the 0. 014–in
The cannula (large black arrow) is deployed and the 0.014–in. guidewire (small black arrow) advanced through it. The nose cone (large white arrow) has the radio-opaque ‘‘LT’’ orientation marker. Catheter shaft (small white arrow)
 is deployed and the 0.014–in. guidewire (small black arrow) advanced through it. The nose cone (large white arrow) has the radio-opaque. ‘‘LT’’ orientation marker. Catheter shaft (small white arrow)")
143
BIOTRONIK

144
Cruiser Guide Wire 0.014“ L: 190 cm Tip Shape: Straight and J

145
Cruiser-18 Hi-support Guide Wire 0.018”
Stiff: 195 cm and 300 cm Medium: 195 cm and 300 cm

146
Passeo-18 Balloon Catheter 0.018” / OTW
Hydrophobic patchwork coated balloon ensures a smooth crossing through tortuous vessels and across high grade stenosis whilst minimising the risk of slippage during inflation experienced using hydrophilic coated balloons

147
Passeo-35 Balloon Catheter 0.035” / OTW
Hydrophobic patchwork coated balloon ensures a smooth crossing through tortuous vessels and across high grade stenosis whilst minimising the risk of slippage during inflation experienced using hydrophilic coated balloons

148
Elect Explorer Balloon Catheter 0.014” / Rx
EFT (Enhanced Force Transmission) increases pushability whilst coating improves trackability and crossability Dedicated and unique dimensions for treatment of infrapopliteal disease.
 increases pushability whilst coating improves trackability and crossability. Dedicated and unique dimensions for treatment of infrapopliteal disease.")
149
Dynamic Balloon-Expandable Stainless Steel Stent 0.035” / OTW

150
Dynamic Renal Balloon-Expandable Cobalt Chromium Stent 0.014” / Rx

151
Astron Self-Expanding Nitinol Stent 0.035” / OTW

152
Astron Pulsar Self-Expanding Nitinol Stent OTW
Dedicated and unique dimensions for treatment of diseases of femoral and infrapopliteal arteries.

153
Thank You…

Similar presentations