Download presentation
Presentation is loading. Please wait.

1
Peritrochanteric Space: Disorders and Treatment
AANA Specialty Day Friday, February 19th, 2011 Bryan T. Kelly, MD Co-Director Center for Hip Pain and Preservation

2
Hospital for Special Surgery
Bryan T. Kelly, MD Hospital for Special Surgery Disclosure: I DO NOT have a financial interest in any commercial products or service presented in this lecture AND DO NOT INTEND to discuss off label or investigational use of products or services.

3
Pivot Medical, Inc.: Consultant Smith & Nephew: Educational Consultant
Types of financial relationships and the companies with whom I have relationships are as follows: Pivot Medical, Inc.: Consultant Smith & Nephew: Educational Consultant A2 Surgical: Consultant

4
The Peritrochanteric Space
Greater Trochanter Iliotibial Band Space between the Greater Trochanter and Iliotibial Band Analogous to the subacromial space in the shoulder

6
Peritrochanteric Space Pathology
External Snapping Hip Greater Trochanteric Pain Syndrome Recalcitrant Trochanteric Bursitis Gluteus Medius Tears Gluteus Minimus Tears

7
External Snapping Hip External coxa saltans results from a thickened band of the posterior iliotibial band or anterior gluteus maximus tendon sliding over the greater trochanter. Any irritation or injury to the underlying bursa results in inflammation and the addition of pain with the snapping.

8
External Snapping Hip Although conservative treatment is usually successful, small numbers of patients remain symptomatic. Open treatment Excision of an ellipsoid-shaped portion of the iliotibial band overlying the greater trochanter and removal of the trochanteric bursa. Zoltan et al. Arthroscopic ITB release can be relatively easily accomplished via the lateral compartment.

9
External Snapping Hip The thickened posterior third of the ITB can be palpated with a flexible probe. The band can be released directly across from the area of irritation on the lateral prominence of the greater trochanter.

10
Peritrochanteric Space Pathology
External Snapping Hip Greater Trochanteric Pain Syndrome Recalcitrant Trochanteric Bursitis Gluteus Medius Tears Gluteus Minimus Tears

11
Greater Trochanteric Pain Syndrome (GTPS)
Lateral sided hip pain and tenderness Common clinical syndrome peaking between the 4th and 6th decades of life. 4♀:1♂ Previously known as “Trochanteric Bursitis” Bursal distention is actually uncommon Kingzett-Taylor et al, 1999 Bird et al, 2001 The initial pathology usually occurs in the tendons attached to the greater trochanter. The adjacent bursae are secondarily involved. Gordon EJ, 1961

12
GTPS (cont.) Vast majority respond to conservative mgt.
Recalcitrant cases are often due to gluteus medius or minimus tendon tears. Prospective MRI evaluation of 24 middle aged women with intractable GTPS 45.8% had gluteus medius tendon tears Bird et al, 2001 Prospective US evaluation of 75 pts with GTPS 53/75 had gluteus medius tendinopathy 25 of these 53 had full or partial g. medius tears Connell et al, 2002

13
Rotator Cuff Tears of the Hip
Bunker et al, 1997 22% of patients with femoral neck fractures had gluteus medius tears Kagan A, 1999 Seven pts with recalcitrant GTPS ranging from 2mos – 10yrs Open repair through bone tunnels & or side-to–side after debride F/u at 45 mos, all were free of pain Howell et al, 2001 20% of women undergoing THA for OA had abductor tears

14
Footprint Anatomy Most gluteus medius tears occur anteriorly, at the junction with the minimus. Gluteus Minimus Gluteus Medius

15
4 facets, 3 have distinct insertions
Dwek J. et al MR imaging of the hip abductors: normal anatomy and commonly encountered pathology at the greater trochanter. Magnetic Resonance Imaging Clinics of North America. 13(4): , vii, 2005 Nov Ant- oval, med border is IT line Lat- inverted triangle, caudal portion is palpable part of troch 4 facets, 3 have distinct insertions
: , vii, 2005 Nov. Ant- oval, med border is IT line. Lat- inverted triangle, caudal portion is palpable part of troch. 4 facets, 3 have distinct insertions.")
16
Anterior Facet 2 parts to Gluteus minimus
Ant facet= glut min= best seen on transverse Arrowhead= lat margin jt capsule, arrows= ant facet, curved arrow- glut min 2 parts to Gluteus minimus tendon attachment lateral to joint capsule Muscular attachment to superior joint capsule

17
Lateral Facet Lat facet= lat part glut medius(muscular attachment), located at post ½ of GT on coronals Cuved arrow glut med, straight arrow= ITB, arrow heads =lat facet Middle and Anterior portions of the medius attach to the lateral facet Also continues anteriorly to cover insertion of minimus

18
Superoposterior Facet
Superopost facet= main glut med tendon attachment= best on coronal Curved whitre arrow= tendon. White Arrow=piriformis Curved black=obt ext, black arrow=obt int Main insertion point for the posterior portion of the medius.

19
Posterior Facet No muscle attachments Trochanteric bursa
Post facet= no muscular attachement, instead trochanteric bursa shown here on bursography No muscle attachments Trochanteric bursa

20
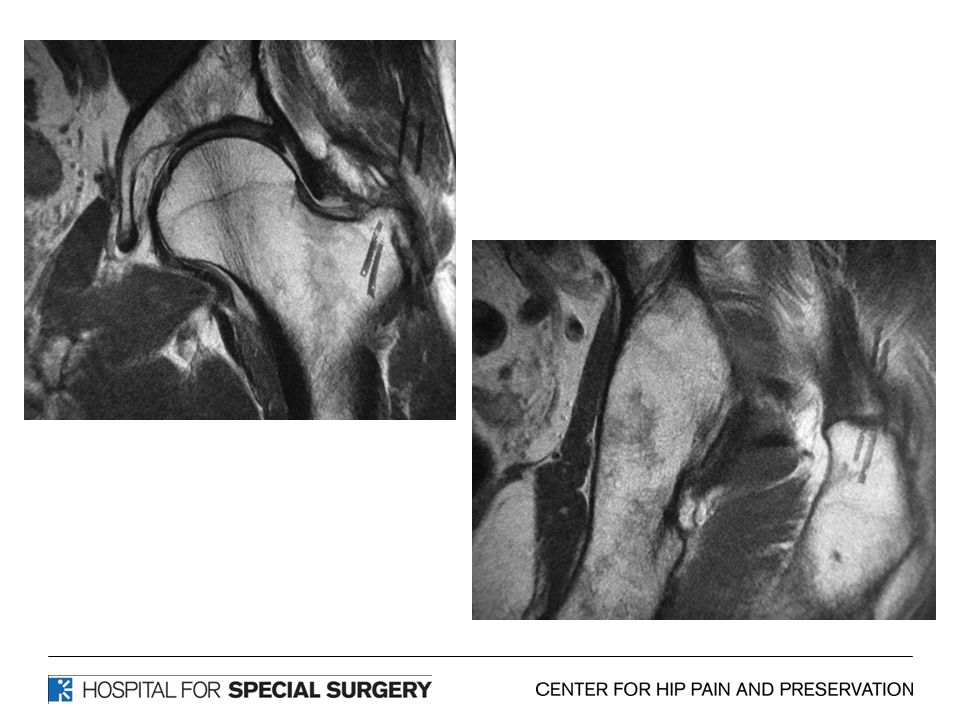
Clinical Presentation: Recalcitrant GTPS – Abductor Tear
Sometimes a history of a “pop” or sudden injury. Age group late 50’s to 60’s Females > Males. Failure of corticosteroid injections. Refractory lateral sided hip pain. Abductor weakness. MRI confirmation. In some (many ?) cases, refractory trochanteric bursitis may be overlooked tears of the gluteus medius and minimus.
 cases, refractory trochanteric bursitis may be overlooked tears of the gluteus medius and minimus.")
21
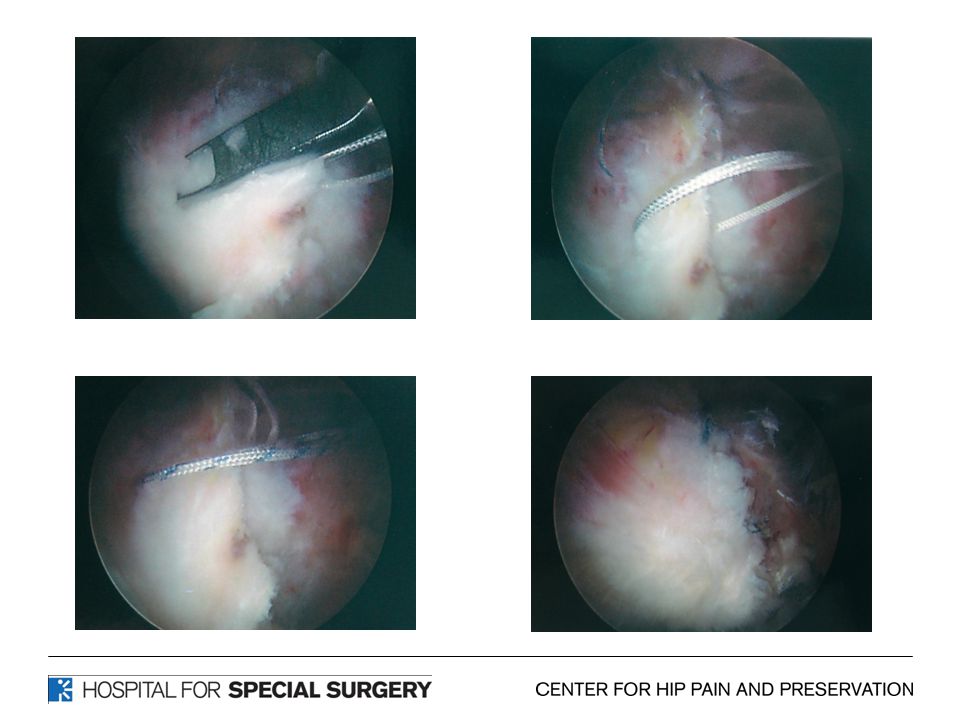
Arthroscopic Management
An arthroscopic approach through the peritrochanteric space is now possible for the repair of focal gluteus medius and minimus tendon tears.

22
Gluteus Medius Tears

23
Repair

25
Abductor Repair - Preparation
In some cases trochanteric spurs may be present that can be burred down to created a better surface area for tendon healing.

26
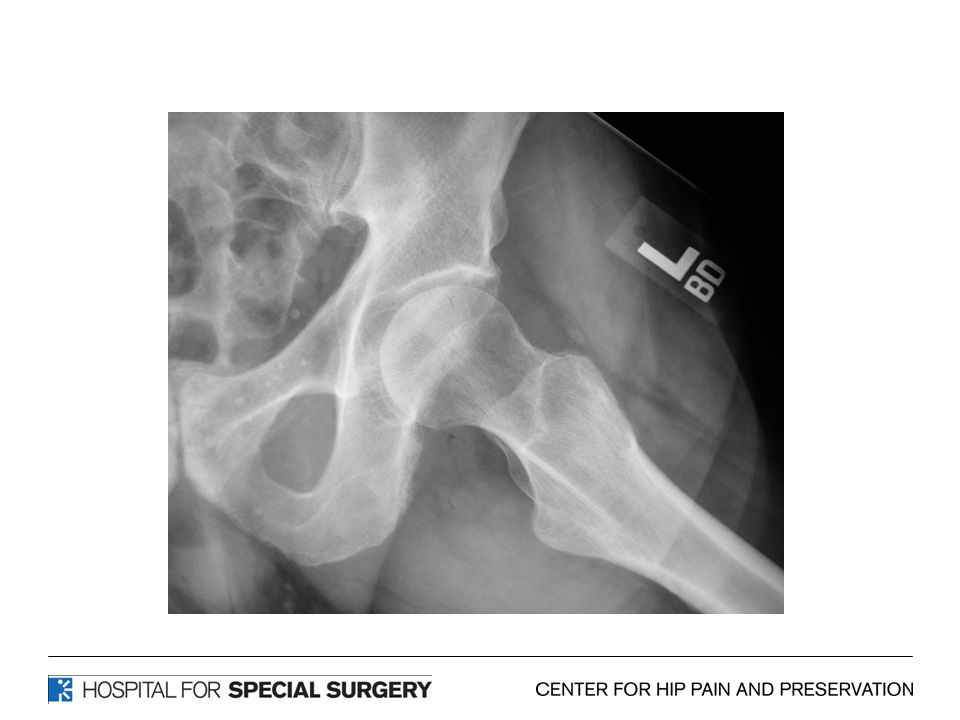
Case TG: Senior Triathlete
65 y/o male Developed left hip pain associated with training Lateral Based No groin pain Treated for trochanteric bursitis with multiple injections / PT with no improvement in symptoms over 6 month period

34
Results Arthroscopic Abductor Repair
Results of 10 patients with minimum of 2 year f/u: All patients had complete resolution of pain in the lateral hip. 9 out of 10 (90%) had 5 out of 5 abductor muscle strength and one patient had 4 out of 5 strength. All patients maintained full hip range of motion.
 had 5 out of 5 abductor muscle strength and one patient had 4 out of 5 strength. All patients maintained full hip range of motion.")
35
Results Arthroscopic Abductor Repair
Modified Harris Hip Scores at one year averaged 92.2 points (range ) and Hip Outcomes Score 93.1 points (range ). 7 out of 10 patients said their hip was normal and 3 said their hip was nearly normal.
 and Hip Outcomes Score 93.1 points (range ). 7 out of 10 patients said their hip was normal and 3 said their hip was nearly normal.")
36
Conclusion Abductor Repair
Endoscopic repair of the gluteus medius tendons to the greater trochanter can be performed in a predictable manner. In the short term, resolution of pain and return to activity is predictable. Long term follow-up and a larger number of patients in prospective trials will provide further insight into the treatment of abductor repairs.

37
Thank You

Similar presentations
























 Muhammad Farrukh Bashir FCPS(ortho)>")