Download presentation
Presentation is loading. Please wait.

1
Presbyopia Abolfazl Kashfi MD Isfahan Medical University

2
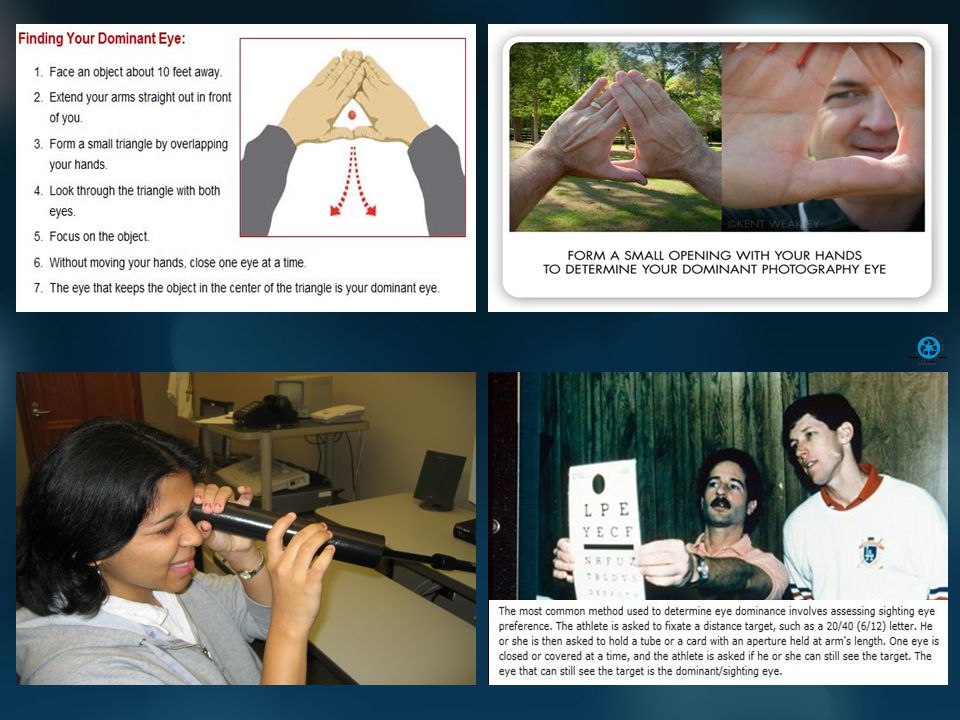
Monovision Definition :One eye for far full correction, one eye for near (33 cm) or intermediate (50 cm) correction Patient selection : Patient’s needs: Suitable for those need far and near vision intermittently. Dominant eye: Dominant eye for far Tolerance: Contact lens trial, strong sighting preference, history of monovision Sex: Females less likely to reject monovision

3
Monovision Methods: contact lens (since 1958,Westsmith) corneal surgery IOL surgery Usually 1.25-2.00 D at most 3.00 D
 corneal surgery IOL surgery Usually D at most 3.00 D")
4
Monovision AdvantagesLimitations Spectacle free High level of satisfaction Acceptable stereopsis Stable VF Physician friendly Less susceptible to decentration Less halo or glare VS multifocal IOLs Easy glasses correction Decreased contrast sensitivity Blurred vision while night driving Blurred intermediate VF defect(?) Challenging preop in cataract
 Challenging preop in cataract")
5
Monovision LASIK Garcia-Gonzalez et al 2010 Reinstein DZ et al 2010 Reinstein DZ et al 2009 Levinger E et al 2006 Reilly CD et al 2006 Miranda D, Krueger RR 2004 Goldberg DB 2003 0.97 D difference monovision LASIK correction is a valid and good method The non-linear aspheric myopic micro-monovision protocol (Carl Zeiss Meditec CRS-Master software and MEL 80 excimer) is well-tolerated, stable, and effective (presbyopia in moderate to high myopic astigmatism) (1-1.5 D difference) Hyperopic micro-monovision protocol (micro-monovision with the Carl Zeiss Meditec MEL80 platform) was a well-tolerated and effective procedure for treating patients with presbyopia in moderate to high hyperopia (1-1.5 D difference) Monovision LASIK is valuable but be cautious for patients in whom night driving and/or reading are an essential part of their life patient satisfaction is good after monovision LASIK but a contact lens trial is advisable monovision is a valuable option for pre-presbyopic and presbyopic patients considering refractive surgery Hyperopic monovision was a viable but more problematic solution to correcting presbyopia than myopic monovision
 is well-tolerated, stable, and effective (presbyopia in moderate to high myopic astigmatism) (1-1.5 D difference) Hyperopic micro-monovision protocol (micro-monovision with the Carl Zeiss Meditec MEL80 platform) was a well-tolerated and effective procedure for treating patients with presbyopia in moderate to high hyperopia (1-1.5 D difference) Monovision LASIK is valuable but be cautious for patients in whom night driving and/or reading are an essential part of their life patient satisfaction is good after monovision LASIK but a contact lens trial is advisable monovision is a valuable option for pre-presbyopic and presbyopic patients considering refractive surgery Hyperopic monovision was a viable but more problematic solution to correcting presbyopia than myopic monovision")
6
Monovision IOL Hayashi et al 2010 Stanojcic et al 2010 Ito M, Shimizu K 2009 Ito M et al 2009 Finkelman YM et al 2009 Marques FF et al 2009 Evans BJ 2007 Greenbaum S 2002 1.5 D difference has a 20/20 far and acceptable near and stereo acuity VF defects are of interest in far-dominant eye (UK driving license criteria) The monovision method group had better reading ability than MF IOL group Pseudophakic monovision is effective after cataract surgery in patients older than 60 years (2.27 D mean difference) Monovision with modest refractive targets achieved good visual function and patient satisfaction (1-1.5 D difference) A viable technique for correction of near, intermediate and distant vision on cataract surgery with high rate of satisfaction (2 D difference) The main limitations are problems with suppressing the blurred image when driving at night and the need for a third focal length, for example with computer screens at intermediate distances. Stereopsis is impaired in monovision, but most patients do not seem to notice this (literature review) Pseudophakic monovision provided a high level of satisfaction
 Pseudophakic monovision provided a high level of satisfaction.")
8
PresbyLasik Definition: Making cornea multifocal using excimer laser Normal human cornea is aspheric instead of multifocal Three approaches : 1 Multifocal transitional 2 Peripheral PresbyLasik (Center for distance and midperipheral for near) 3Central PresbyLasik (Hyperpositive center for near and leaving periphery for far)
 3Central PresbyLasik (Hyperpositive center for near and leaving periphery for far)")
9
PresbyLasik Multifocal transitional An intentionally decentered Hyperopic ablation to produce a transitional vertical multifocality,inducing a significant vertical coma An old technic / Very few publications / Not generally accepted and now abandoned because of doubtful quality of vision

10
PresbyLasik peripheral presbyLasik Center left for distance and the periphary ablate in a manner which produces a negative aspherisity and a 3 diopter pseudoaccommodation in 4mm pupil VISX, Zeiss, Nidek, Wave light-Allegrato A good DOF but There is an interaction with myopic correction Most studies done in hyperopes 8/10 to 10/10 far vision and J2 for near 6 month neuroadaptation required

11
PresbyLasik Central presbyLasik A central hyperpositive area for near and periphery left for far Much prolate cornea much depth of field (KC) Can perform in myopes, hyperopes or emmetropes,even previous LASIK Minimal tissue ablation 8/10 to 10/10 far vision and J2 for near Pupil dependent Centration is very important,it is up to induce coma aberration
 Can perform in myopes, hyperopes or emmetropes,even previous LASIK Minimal tissue ablation 8/10 to 10/10 far vision and J2 for near Pupil dependent Centration is very important,it is up to induce coma aberration")
13
Femtosecond assisted Intracor First introduced by Ruiz et al in 2009 (83 eyes) followed by Holzer et al in 2009 (25 non dominant eyes) They used TECHNOLAS femtosecond platform to make a series of concentric intrastromal cuts for presbyopic emetrrops/hyperops. They made some intrastromal radial cuts to treat distance vision of presbyopic myops. The produced Hyperprolate cornea will give a better near vision while distance vision is preserved.(negative shift of primery spherical aberrations and positive shift of secondary aberrations)
.")
14
Video from www.technolaspv.com The strongest lamellae of cornea are in the anterior one third of cornea ;during INTRACOR anterior cornea remains intact to avoid uncontrolled ecstasia INTRACOR1.avi

15
Femtosecond assisted Intracor Advantages Painless,high level of satisfaction Minimally invasive (Epithelium, Bowman, descemet and endothelium are intact)/ minimal risk of infection Short treatment time Significant and rapid near vision improvement Improves depth of focus Minimal changes of CDVA Minimal myopic shift (0.3 D) Minimal endothelial change Stable corneal thickness stable contrast sensitivity Stable total and higher order aberrations
/ minimal risk of infection Short treatment time Significant and rapid near vision improvement Improves depth of focus Minimal changes of CDVA Minimal myopic shift (0.3 D) Minimal endothelial change Stable corneal thickness stable contrast sensitivity Stable total and higher order aberrations")
16
Femtosecond assisted Intracor Disadvantages: Few patients loss 1 to 2 lines of CDVA Symptomatic halo (30% day one, 3% after one year) Not suitable for scotopic pupil > 6.5 mm Many unknowns ? Centering ? Retreatment

18
Corneal inlays Flexivue microlens A 3mm hydrophilic lens with 15 microns thickness under a Femtosecond made corneal pocket to correct 2.5 D to 3.5 D presbyopia of non dominant eyes Reported by Pallikaris 2010 One year follow up 100% improvement 92% Nea spectacle free Mean UCNVA after 3 month 20/25 Mean UCDVA after 6 month 20/30 It has CE but not FDA approval

19
Corneal inlays KAMRA inlay A 3.8 mm 10 microns thickness implant with a 1.6 mm central hole under a femtosecond made corneal flap to correct vision via pinhole effect Polyvinylidine flouride polymer with 1600 nutritional holes Formerly AcuFocus Reported by Durrie 2010 36 months follow up Mean distance vision 20/20 Mean near vision J1 It has CE but not FDA approval (there is an ongoing 504 patients study in US)
")
20
Corneal inlays KAMRA inlay

21
Thanks

Similar presentations







 Seyed Javad Hashemian MD Eye Research Center Rassoul Akram Hospital TUMS No financial.>")










 FRCSC 1,2,3,4.>")
, FRCSEd.>")


