Download presentation
Presentation is loading. Please wait.

1
Management Strategies for Stage I germ cell tumours
Professor Gordon J S Rustin Director of Medical Oncology Mount Vernon Hospital Northwood, Middlesex England

2
Testicular Germ Cell Tumours
Approximately 2000 new cases per year in UK (population ) 70% of seminomas and 50% of NSGCTs are diagnosed at stage I
 70% of seminomas and 50% of NSGCTs are diagnosed at stage I.")
3
Considerations in initial management
Is a testicular cancer present? Are there metastatses? Is there carcinoma in situ in contralateral testis? If there are bilateral tumours is partial orchidectomy an option?

4
Initial management Widespread malignancy refer for immediate chemotherapy No evidence of spread inguinal orchidectomy. Biopsy of contralateral testicle should be considered if there is a high risk of carcinoma in situ eg. small testis (<12ml), and in patients < 30 years. SJ Harland. Eur Urol 1993 n= % pts had CIS in contralateral testis. Increased risk of CIS in clinically atrophic testes, but NOT in maldescent. Pts found to have CIS were younger < 30 Complete post – op staging, CT chest/abdo/pelvis Post –op tumour markers if raised pre-op. Should fall according to half life – (4-6 days for AFP, 24 hours for HCG)
, and in patients < 30 years. SJ Harland. Eur Urol 1993 n= % pts had CIS in contralateral testis. Increased risk of CIS in clinically atrophic testes, but NOT in maldescent. Pts found to have CIS were younger < 30. Complete post – op staging, CT chest/abdo/pelvis. Post –op tumour markers if raised pre-op. Should fall according to half life – (4-6 days for AFP, 24 hours for HCG)")
5
Points to consider in managing stage 1 germ cell tumours
Seminomas spread predictably, firstly to the para-aortic lymph nodes and subsequently to the supra-diaphragmatic LNs and on to other metastatic sites. NSGCT spread more randomly with blood borne mets occuring earlier than with seminoma NSGCT produce AFP and/or HCG in 75% of cases Seminomas produce HCG in only 25% of cases LDH is non-specific. In our series of 494 patients who relapsed on surveillance over a 10 year period, the LDH alone did not identify any of these.

6
Management of carcinoma in situ
50% of patients with CIS will develop invasive tumours within 5 years from diagnosis. Low dose XRT (20 Gy in 10#s) to the testis eradicates CIS, relapses with lower doses Leydig cell function increasingly impaired at doses > 17 Gy Long term hormone replacement therapy may be necessary
 to the testis eradicates CIS, relapses with lower doses. Leydig cell function increasingly impaired at doses > 17 Gy. Long term hormone replacement therapy may be necessary.")
7
Possible prognostic factors for stage 1 germ cell tumours
SEMINOMAS Size of tumour (J Clin Onc 2002, Warde et al) Invasion into the rete testis Age Small vessel invasion Histological subtype – classical vs anaplastic DNA ploidy status Mitotic count DNA S-phase % Syncitiotrophoblasts Degree of lymphocytic infiltration of primary tumour Expression of HCG and low MW keratin on immunohistochemistry TERATOMAS Lymphovascular invasion Embryonal ca histology in primary tumour MIB- 1 monoclonal ab – marker of proliferative activity Mitotic count
 Invasion into the rete testis. Age. Small vessel invasion. Histological subtype – classical vs anaplastic. DNA ploidy status. Mitotic count. DNA S-phase % Syncitiotrophoblasts. Degree of lymphocytic infiltration of primary tumour. Expression of HCG and low MW keratin on immunohistochemistry. TERATOMAS. Lymphovascular invasion. Embryonal ca histology in primary tumour. MIB- 1 monoclonal ab – marker of proliferative activity. Mitotic count.")
8
Options for management of stage I Seminomas
Adjuvant radiotherapy Adjuvant chemotherapy Surveillance

9
1980’s Management of stage I seminoma
20% will recur after orchidectomy 90% relapse in para-aortic nodes Traditionally adjuvant treatment with radiotherapy to para-aortic and ipsilateral iliac nodes in a “dog leg” field. (28-30 Gy)
")
10
Late Morbidity from Radiotherapy
Second Cancers Cardiac events Peptic ulceration Infertility

11
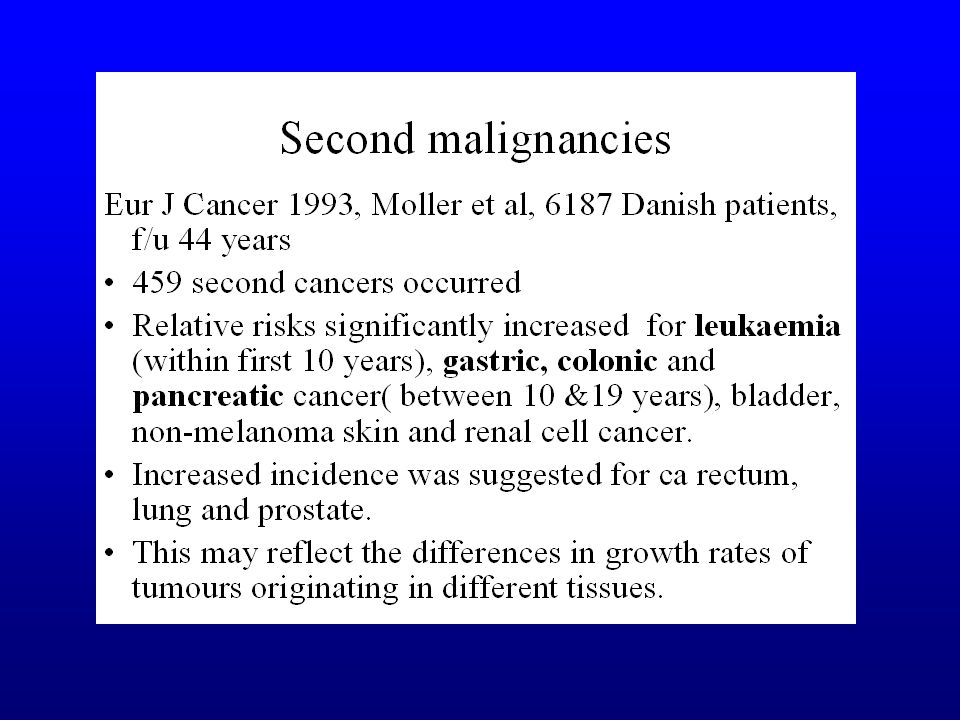
Relative risks for second primary cancers (NB
Relative risks for second primary cancers (NB. RR of contralateral testis ca is 35.7!) 1.7 25 Colon 1.3 16 Rectum 2.2 Kidney 1.8 47 Other skin 5 Melanoma 1.0 42 Lung 1.1 21 Prostate 2.1 37 Bladder 15 Pancreas 1.9 24 Stomach 2.3 13 Leukaemia 1.5 337 All sites RR n
 Colon Rectum Kidney Other skin. 5. Melanoma Lung Prostate Bladder. 15. Pancreas Stomach Leukaemia All sites. RR. n.")
13
Strategies to reduce radiotherapy morbidity
Reduction of radiation field size MRC TE patients randomised to traditional dog-leg or para-aortic radiotherapy Reduction in dose MRC TE patients randomised to 30 Gray in 15 # over 3 weeks or 20 Gray in 10 # over 2 weeks

14
MRC TE10 (Fossa et al 1999) Survival at 3 years, 99% for PA vs 100% for DL RFS 96% PA vs 96.6% DL Acute toxicity ( nausea, vomiting, leukopaenia) was less frequent and less severe in PA group Within the first 18/12 of F/U the sperm counts were significantly higher after PA than after DL radiotherapy. CONCLUSION: Adjuvant radiotherapy confined to the paraaortic LNs is associated with decreased haematologic, GI and gonadal toxicity, but with a higher risk of pelvic recurrence compared with dog-leg radiotherapy.
 was less frequent and less severe in PA group. Within the first 18/12 of F/U the sperm counts were significantly higher after PA than after DL radiotherapy. CONCLUSION: Adjuvant radiotherapy confined to the paraaortic LNs is associated with decreased haematologic, GI and gonadal toxicity, but with a higher risk of pelvic recurrence compared with dog-leg radiotherapy.")
15
MRC TE 18 (Jones et al 2001 & 2005) Therefore:
At median follow-up of 4 years 2 year relapse free survival 97.7% after 30Gy 97% after 20Gy Better Quality of Life scores for acute effects in lower dose arm Therefore: Standard radiotherapy for stage 1 seminoma should be: 20 Gy in 10 # over 2 weeks to para-aortic strip unless previous inguino/pelvic/scrotal surgery when “dog-leg” field.

16
Can chemotherapy replace radiotherapy for stage 1 seminoma
Can chemotherapy replace radiotherapy for stage 1 seminoma ? TE19 / EORTC 30982 Randomised comparison of single agent carboplatin AUC 7 with radiotherapy in adjuvant treatment of stage 1 seminoma following orchidectomy. carboplatin n= Gy/15#s Radiotherapy 20Gy/10#s

17
TE 19 Radiotherapy vs carboplatin : Relapse Free Rate
RFR at 2 years at 3 years R96.7% (95%, 98%)95.9% (94%, 97%) C97.7% (96%, 99%)94.8% (93%, 96%) Absolute difference R - C =-1.0% (-2.5%, 0.5%)1.1% (-1.0%, 3.2%) HR based CI for difference R – C =0.9% (-0.5%, 3.0%)1.1% (-0.6%, 3.7%)
95.9% (94%, 97%) C97.7% (96%, 99%)94.8% (93%, 96%) Absolute difference. R - C =-1.0% (-2.5%, 0.5%)1.1% (-1.0%, 3.2%) HR based CI for difference. R – C =0.9% (-0.5%, 3.0%)1.1% (-0.6%, 3.7%)")
18
Results of TE19 / EORTC 30982

19
Late Morbidity from Chemotherapy
Infertility Second Tumours Cardiovascular damage

20
Prognostic Factors for seminomas on surveillance ( Warde et al 2002)
121 of 638 patients relapsed at a median follow up of 7 years (Relapse free survival 82%) On multivariate analysis: Tumour size <4cm vs >4cm, hazard ratio 2 Invasion of the rete testis, hazard ratio 1.7 5 year recurrence rate Both risk factors 32% Single risk factor 16% No risk factors 12%
 On multivariate analysis: Tumour size <4cm vs >4cm, hazard ratio 2 Invasion of the rete testis, hazard ratio year recurrence rate. Both risk factors 32% Single risk factor 16% No risk factors 12%")
21
Post orchidectomy surveillance vs carboplatin for stage 1 seminoma – Spanish germ cell cancer cooperative group; Ann oncol 2003 N = 203 60 pts with tumour >4cm or lymphovascular invasion given 2 x carboplatin 143 pts with no risk factors put on surveillance 5 yr DFS 83.5% in surveillance pts and 96.6% in carbo grp. All salvaged with 3 or 4 cycles of BEP 5 year OS 96.7%. Cause specific survival 100%

22
Conclusion on management of stage 1 seminomas
Almost 100 % of patients with stage 1 seminoma are cured regardless of approach chosen as post orchidectomy therapy. Adjuvant radiotherapy or chemotherapy are both as effective at reducing relapse rates. However with a relapse rate of 15-20%, and a 5 year survival of 97.7%, surveillance may be considered an alternative “treatment” option. Identification of prognostic factors for relapse on surveillance will allow clinicians to recommend the most appropriate therapy for individual patients. Current recommendations – tumours <4cm and absence of rete testis invasion – RR 12% - surveillance. Tumours >4cm and presence of rete testis invasion – RR 35% offer adjuvant therapy

23
Management Options for Stage 1 Non-seminomatous germ cell tumours
Surveillance RPLND Adjuvant chemotherapy

24
Surveillance for Non-seminomatous germ cell tumours
relapse rate Overall 30% Lymphovascular invasion <40% No risk factors %

25
Surveillance programme MVH - NSGCTs
Month 1 2 3 4 5 6 7 8 9 10 11 12 18 24 36 OPD X CXR Markers xx CT Chest/ abdo/ pelvis Markers currently HCG, AFP and LDH Follow up for 10 years

26
Advantages of Surveillance for Low risk NSGCT
>80% avoid any chemotherapy or RPLND >80% avoid risk of 2nd tumours >80% avoid risk of cardiovascular damage >80% avoid risk of infertility

27
Disadvantages of surveillance for NSGCT
More frequent clinic visits and blood tests Greater diagnostic radiation (10 body CT scans induces 1% 2nd tumours) Anxiety of follow -up Concern about non-attendance
 Anxiety of follow -up. Concern about non-attendance.")
28
MRC TE08 trial of surveillance intensities
Currently a wide variation in the intensity of surveillance programs between hospitals Concern about high levels of radiation produced by CT scans Alternative methods need to be found to determine relapse during surveillance Frequency of CT scans needs to be kept to a minimum

29
Histologically confirmed
Study Design Histologically confirmed Stage I NSGCT Randomise 5 CT scans Chest and abdomen CT at 3 months Chest and abdomen CT at 6 months Chest and abdomen CT at 9 months Chest and abdomen CT at 12 months Chest and abdomen CT at 24 months 2 CT scans 3:2 randomisation in favour of 2 CT arm

30
Lack of value of chest CT scans in surveillance of Stage I NSGCT
168 patients 42 (25%) relapsed 8/42 (19%) intrathoracic relapse All 8 had abnormal CXR at relapse 7/8 also had elevated AFP and or HCG (Harvey et al Annals Oncol 13: , 2002) 1 1
 relapsed. 8/42 (19%) intrathoracic relapse. All 8 had abnormal CXR at relapse. 7/8 also had elevated AFP and or HCG. (Harvey et al Annals Oncol 13: , 2002)")
31
183 stage 1 GCT on surveillance: Initial Presenting Factors among 52 relapses (Francis et al EJC 2000) Symptoms Tumour Markers Radiology (total/no. NSGCT/no. seminoma) 4/3/1 24/21/3 3/2/1 3/3/0 15/8/7 3/3/0 18/12/6
 4/3/1. 24/21/3. 3/2/1. 3/3/0. 15/8/7. 3/3/0. 18/12/6.")
32
Adjuvant BEP chemotherapy for high risk NSGCT (Cullen et al 1996)
2 courses Bleomycin 30,000 units day 2, 8, 15, Etoposide 120 mg/m2 days 1-2, Cisplatin 50 mg/m2 day 1&2 Reduces risk of relapse to <3%

33
MRC Trial TE22: Study of FDG PET in the prediction of relapse in patients with high risk stage 1 NSGCT 108 patients registered by 78/96 (81%) PET scans negative, 77/78 chose surveillance Expected relapse free rate for high risk ~60% at 2 years Anticipated relapse free rate for PET –ve patients ~90% at 2 years (90%CI >80%) Interim analysis 12 month relapse free rate in 77 PET –ve patients 65% (90% CI 53-74%) at 2 years at best 70% Trial closed
 PET scans negative, 77/78 chose surveillance. Expected relapse free rate for high risk ~60% at 2 years. Anticipated relapse free rate for PET –ve patients ~90% at 2 years (90%CI >80%) Interim analysis 12 month relapse free rate in 77 PET –ve patients 65% (90% CI 53-74%) at 2 years at best 70% Trial closed")
34
Comparison of management policies for NSGCT
Surveillance Low risk RPLND Adjuvant BEP Relapse rate <20% % <3% Require chemo <20% % 100% Require RPLND < 5% % <1%

35
Comparison of costs per life saved for managing stage 1 germ cell tumours (Francis et al EJC 2000)
Surveillance RPLND Adjuvant chemotherapy £ £ £5851

36
Management of Stage 1 Testicualr Germ Cell tumours
Many surgeons do orchidectomies, Only a few oncologists should specialise in managing GCT patients Patients should be made aware of the different management options Deciding which option depends upon histology, prognosis, geography, personality, reliability, bias of the doctor, but most importantly the patient

37
Life insurance for patients treated for germ cell tumours
Time without Time to standard Extra/£1000 yr3-4 Extra year 5-6 Seminoma stage1 1 year 4 years £5 Non-seminoma stage 1 6 years £10 Stage 2 A/B 2-3 years 9 years Stage 2 B, stage 3 3 years £15 Stage 4, intermediate and poor risk 3-4 years £20 Temporary loading usually lasts 3-6 years Provided by Graham Jones Underwriting Development Product Management & Development - Protection Direct line: (internal: 5736)
")
38
Factors for Research Prognostic factors to more accurately define those requiring treatment : eg. Compare by comparative genomic hybridization and expression micoarray analysis relapses versus non relapses Reduce diagnostic radiation by comparing MRI with CT scans To better understand factors increasing incidence of germ cell tumours To better understand relationship of 12p isochromosome and Kit with germ cell tumours

39
STROMAL TUMOURS OF THE TESTIS
Leydig, Sertoli cell, Granulosa cell or combined tumours 3% of testis tumours, 10% bilateral Derive from cells making hormones Mean age 36 years 10% metastasise – cannot currently be predicted from histopathology of the primary tumour testosterone, oestradiol and androstenedione are markers (AFP and hCG are not) Resistant to conventional chemotherapy and radiotherapy.
 Resistant to conventional chemotherapy and radiotherapy.")
40
. SURVIVAL FOLLOWING RPLND FOR STROMAL TUMOURS OF THE TESTIS ACCORDING TO PATHOLOGICAL STAGE. 0.00 0.25 0.50 0.75 1.0 0.0 25 50 75 100 Time (months) Survival Stage I Stage II
 Survival. Stage I. Stage II.")
42
Would surveillance alone be an option?

43
Curr opin oncol 2004 n= 394 stage I seminomas, 301 stage I NSGCTs, post orchidectomy % relapse rate – 17% seminomas, 29% NSGCTs. Median time to relapse 13 months for seminomas with 49% relapsing in first year, 5 months for NSGCT, 80% relapsing in first year. 54% of NSGCTs with vascular invasion relapsed and 38% of the seminomas 32% of NSGCTs with embryonal ca relapsed. 90% of relapses detected as routine examination, remaining 10% at patients initiative – treated appropriately with surgery/chemo/radiation 10 deaths in F/u, not related to GCT Os 98.6%, cause specific survival 100%

48
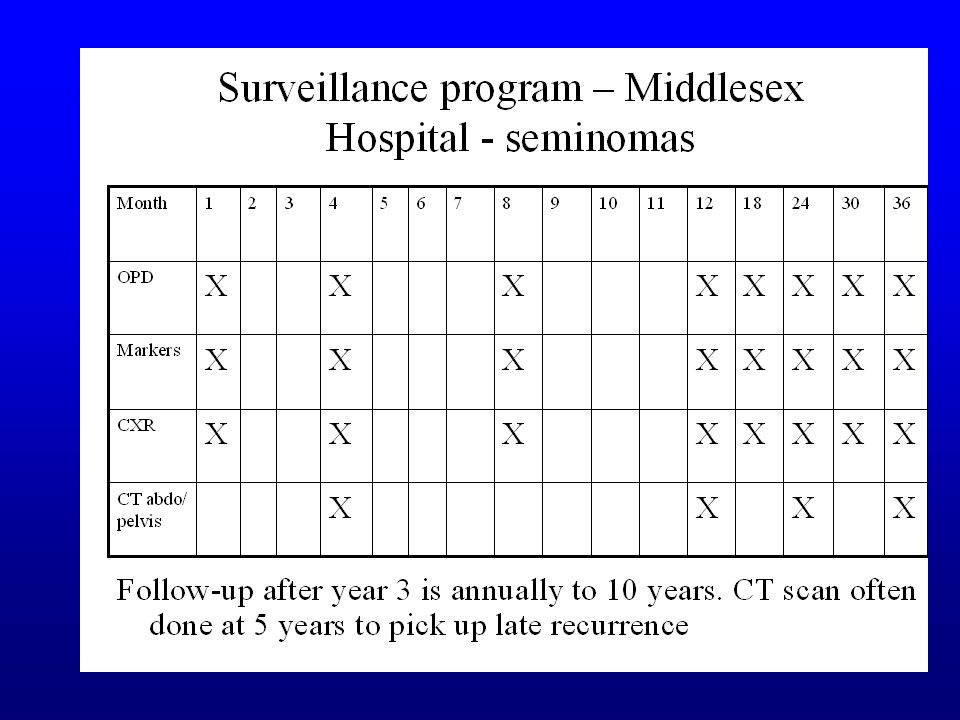
Surveillance programme MVH - seminomas
Month 1 2 3 4 5 6 7 8 9 10 12 18 24 36 OPD X CXR Markers CT abdo/ pelvis CXR & markers performed at each clinic visit. Year 2 OPD every 2/12, Year 3 every 3/12, year 4 every 4/12, years 5 and 6 every 6/12. Yearly thereafter to 10 years. Lifetime follow-up if had XRT.

49
Management of stage I NSGCT
Relapse rate after orchidectomy alone – 25% Vascular or lymphatic invasion relapse rate – 40% Surveillance – low risk patients (85% cure rate surgery alone) 2 x BEP – in high risk patients with vascular or lymphatic invasion reduces relapse rate to 1% Prophylactic RPLND J Urol 2000 – group of high risk stage I teratomas, relapse risk 35-40% - RPLND reduced relapse risk to 23%. Comparable group given BEP x 2 – risk of relapse 3-4%. Good risk patients on surveillance with a 15-20% risk of relapse -RPLND reduces relapse risk to 5%
 2 x BEP – in high risk patients with vascular or lymphatic invasion reduces relapse rate to 1% Prophylactic RPLND. J Urol 2000 – group of high risk stage I teratomas, relapse risk 35-40% - RPLND reduced relapse risk to 23%. Comparable group given BEP x 2 – risk of relapse 3-4%. Good risk patients on surveillance with a 15-20% risk of relapse -RPLND reduces relapse risk to 5%")
51
Management of Stage IIA and B seminoma
Radiotherapy 30Gy in 15 fractions

52
Stage II NSGCT Ongoing debate ?PRLND alone vs neoadjuvant chemo followed by surgery. German trial n=187. No difference in OS but in suregery alone group, significantly higher loss of ejaculation Oldenberg et al n=87, stage II NSGCT undergoing RPLND All patients had masses < 2cm on imaging. Viable tumour found in 33% (26% mature teratoma, 7% malignant tumour), 67% fibrosis/necrosis. No clinical/serological parameters were predictive of histopath findings. CONCLUSION: RPLND recommended for all patients with masses < 2cm because of high rate of viable tumour found
, 67% fibrosis/necrosis. No clinical/serological parameters were predictive of histopath findings. CONCLUSION: RPLND recommended for all patients with masses < 2cm because of high rate of viable tumour found.")
53
Testicular germ cell tumours – Professor Rustin – MVH Cancer Centre

54
Testicular germ cell tumours Professor Rustin – MVH Cancer Centre

57
Testicular Germ Cell tumours
Professor Rustin Mount Vernon Hospital Cancer Centre

59
1-1.5% of male neoplasms Most common tumour in men aged yrs. Incidence has doubled in last 20 years One of the few solid tumours which is completely curable even after it has metastasized with an overall survival of 90% 70% of seminomas and 50% of NSGCTs are diagnosed at stage I

60
Pathological classification of testicular cancers
Seminoma Spermatocytic seminoma Teratoma Non-seminomatous germ cell tumour Teratoma Differentiated (TD) Mature teratoma Malignant teratoma intermediate (MTI) Embryonal carcinoma with teratoma (teratocarcinoma) Malignant teratoma undiffrentiated (MTU) Yolk sac tumour, embryonal carcinoma Malignant teratoma trophoblastic (MTT) Yolk sac tumour; choriocarcinoma
 Mature teratoma. Malignant teratoma intermediate (MTI) Embryonal carcinoma with teratoma (teratocarcinoma) Malignant teratoma undiffrentiated (MTU) Yolk sac tumour, embryonal carcinoma. Malignant teratoma trophoblastic (MTT) Yolk sac tumour; choriocarcinoma.")
66
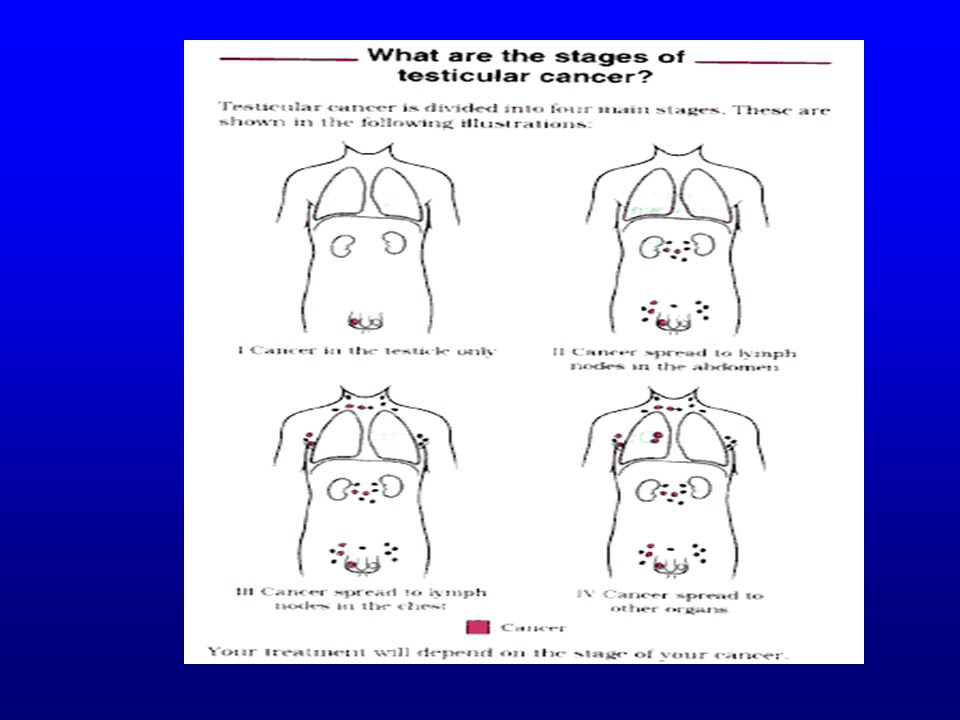
RMH Staging I – No evidence of disease outside the testis
IM – As above but persistently raised tumour markers II – Infradiaphragmatic nodal involvement IIA – max diameter <2cm IIB- max diameter 2-5cm IIC – max diameter 5-10cm IID – max diameter >10cm III – Supra and infradiaphragmatic node involvement Abdominal nodes a,b,c, as above, Mediastinal nodes M+, Neck nodes N+ IV – Extralymphatic metastases. Lungs: L1 - <3 mets, L2- multiple mets < 2 cm, L3 – multiple mets >2cm. Liver involement H+. Other sites specified.

70
Prognostic Factors for seminomas on surveillance

71
tumour size – RFR < 4cm 87%, >4cm 76% (p=0.003)
n=638 (seminomas), F/U 7 years, 121 relapses – 5 year RFR 82% On univariate analysis: tumour size – RFR < 4cm 87%, >4cm 76% (p=0.003) Rete testis invasion – RFR 86% (absent), 77% (present) p=0.003 Presence of small vessel invasion – RFR 86% (absent), 77% (present) p= 0.038
, F/U 7 years, 121 relapses – 5 year RFR 82% On univariate analysis: tumour size – RFR < 4cm 87%, >4cm 76% (p=0.003) Rete testis invasion – RFR 86% (absent), 77% (present) p= Presence of small vessel invasion – RFR 86% (absent), 77% (present) p=")
72
Prognostic factors investigated in seminomas

Similar presentations


























; FRCS (Ireland); MMed (Wits); FCS (SA) Urology 38 th BMA CONGRESS.>")








