Download presentation
Presentation is loading. Please wait.

1
ESOFAGO DI BARRETT TERAPIA MEDICA & ENDOSCOPICA Massimo Conio Sanremo Massimo Conio Sanremo

2
Barrett's Esophagus & HGD Strategies Passive:surveillance Active:endotherapy surgery chemoprevention Passive:surveillance Active:endotherapy surgery chemoprevention

3
Barrett's Esophagus & HGD 58 patientsfollow-up: 10 years 26%invasive cancer 27%“regression” 58 patientsfollow-up: 10 years 26%invasive cancer 27%“regression” Gastroenterology 1996

4
ChemopreventionChemoprevention COX-2 inhibition Prostaglandins enhance: Proliferation Angiogenesis Invasiveness Apoptosis inhibition COX-2 inhibition Prostaglandins enhance: Proliferation Angiogenesis Invasiveness Apoptosis inhibition

5
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Years of follow-up Dysplasia rate % El-Serag et al., Am J Gastroenterol 2004 No PPI Therapy PPI Therapy

6
Esophagectomy (40% simultaneous foci of intramucosal cancer) Morbidity48% Mortality2-3% Barrett’s Esophagus with High-Grade Dysplasia
 Morbidity48% Mortality2-3% Barrett’s Esophagus with High-Grade Dysplasia")
7
CP1109264-26 Barrett’s with High-Grade Dysplasia On Biopsy. No Visible Lesion.

8
SCJ Barrett's Esophagus;Histologic Maps of Surgical Resections Barrett's, no dysplasia Low-grade dysplasia High-grade dysplasia Adenocarcinoma CP1109264-27

9
Photodynamic therapy (PDT) sodium porfimer (Photofrin®) 5-aminolevulinic acid Thermal Laser (Nd:YAG, KTP) Argon Plasma Coagulator (APC) MPEC Mechanical Ultrasonic Microwave Cryotherapy Endoscopic Ablative Therapies For Barrett’s Esophagus With HGD
 sodium porfimer (Photofrin®) 5-aminolevulinic acid Thermal Laser (Nd:YAG, KTP) Argon Plasma Coagulator (APC) MPEC Mechanical Ultrasonic Microwave Cryotherapy Endoscopic Ablative Therapies For Barrett’s Esophagus With HGD")
10
Esophagus: Japanese data About 1000 patients “En-bloc” (< 3 cm)CR 100% Piecemeal ( 3 cm)CR 86% (N1: 23%) About 1000 patients “En-bloc” (< 3 cm)CR 100% Piecemeal ( 3 cm)CR 86% (N1: 23%) 5-year survival97.9%(surgery: 98%)
CR 100% Piecemeal ( 3 cm)CR 86% (N1: 23%) About 1000 patients En-bloc (< 3 cm)CR 100% Piecemeal ( 3 cm)CR 86% (N1: 23%) 5-year survival97.9%(surgery: 98%)")
11
Visible nodular abnormalities Comorbidities/Advanced age Efficacy to be determined Endoscopic Mucosal Resection (EMR) Barrett’s Esophagus
 Barrett’s Esophagus")
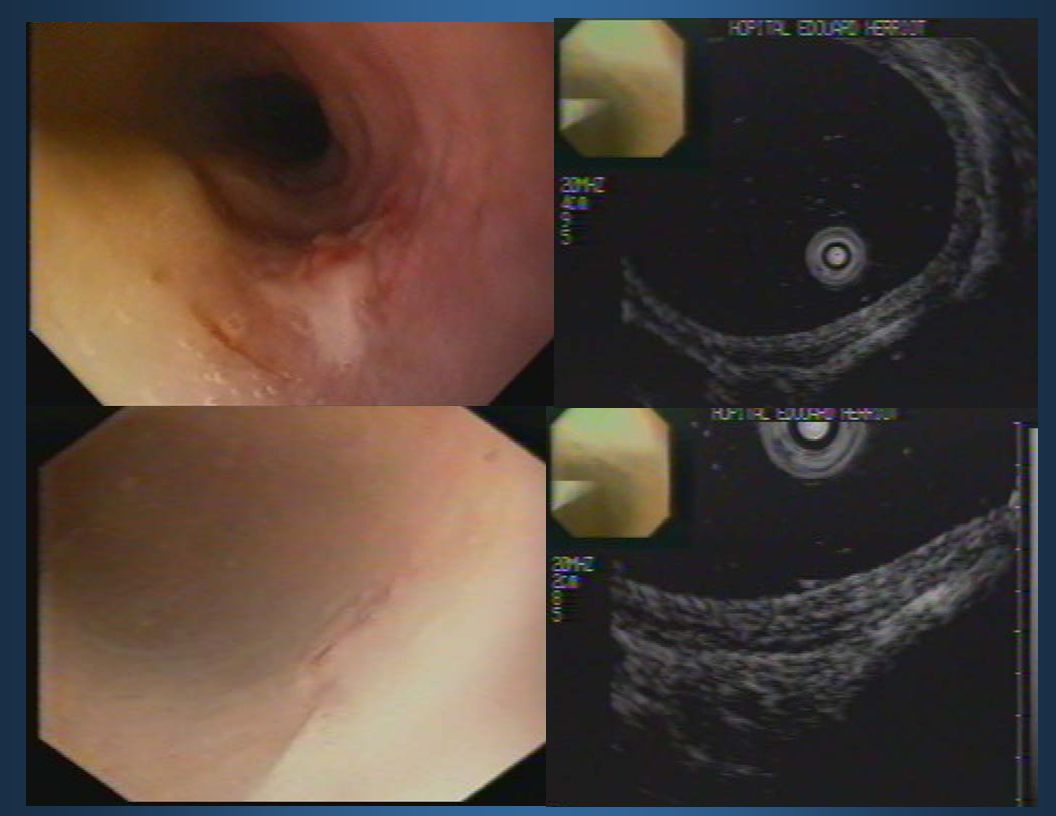
13
When not to do EMR 20 Mhz probe EUS at 7.5 MHz

14
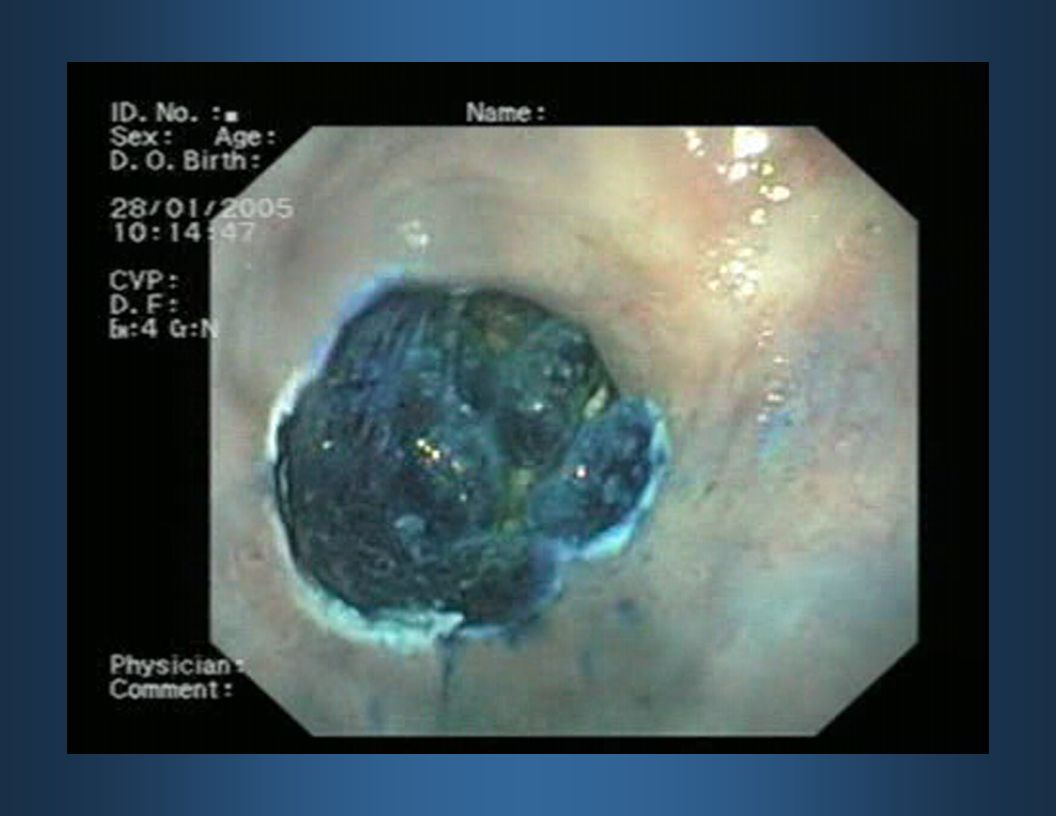
Superficial cancers

16
m sm pm1 pm2

20
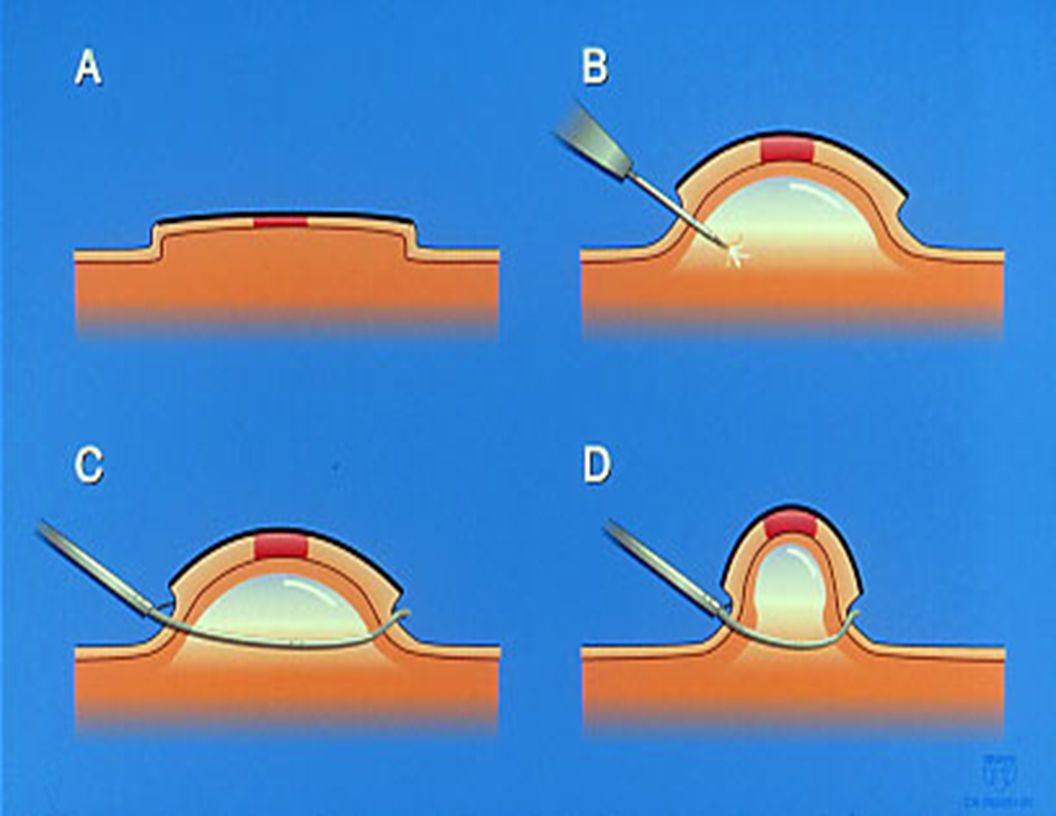
Oblique aspiration mucosectomy device Attached to tip of conventional endoscope. Tanabe et al. Gastrointest Endosc, 2004

22
GROUP A GROUP B N. Sessions (mean)*1.3 0.62.8 2.0 Complete remission* 97%59% Complications1 spurting1 oozing *statistically significant EMR in Barrett’s esophagus with HGD Ell et al., Gastroenterology 2000
*1.3 2.0 Complete remission* 97%59% Complications1 spurting1 oozing *statistically significant EMR in Barrett’s esophagus with HGD Ell et al., Gastroenterology")
23
EMR in Barrett’s esophagus Change in the diagnosis: 44% 32% up-staging Change in the diagnosis: 44% 32% up-staging Nijhawan et al., Gastrointest Endosc 2000

24
May 2000 – December 2003: 39 pts (mean age 62.8±11.4 yrs) Mucosal abnormalities: 36 EUS 20-MHz May 2000 – December 2003: 39 pts (mean age 62.8±11.4 yrs) Mucosal abnormalities: 36 EUS 20-MHz EMR for High-Grade Dysplasia and Intramucosal Cancer Conio, Repici, Cestari, World J Gastroenterol 2005
 Mucosal abnormalities: 36 EUS 20-MHz May 2000 – December 2003: 39 pts (mean age 62.8±11.4 yrs) Mucosal abnormalities: 36 EUS 20-MHz EMR for High-Grade Dysplasia and Intramucosal Cancer Conio, Repici, Cestari, World J Gastroenterol 2005")
25
Histology of lesions HistologyPre-EMRPost-EMR LGD-5 (12.8%) HGD35 (89.7%)27 (69.2%) IM. AC4 (10.3%)2 (5.1%) Invasive AC-5 (12.8%) Change of the original diagnosis 25.6%
2 (5.1%) Invasive AC-5 (12.8%) Change of the original diagnosis 25.6%.")
26
EMR for HGD and/or Intramucosal Cancer AC sm 3 AC >> Surgery (no residual disease) 2 AC >> Follow-up (cancer free) Complications Bleeding4 patients (endoscopic treatment) Follow-up (median 20 months) 1 recurrence (HGD) >> EMR AC sm 3 AC >> Surgery (no residual disease) 2 AC >> Follow-up (cancer free) Complications Bleeding4 patients (endoscopic treatment) Follow-up (median 20 months) 1 recurrence (HGD) >> EMR
 2 AC >> Follow-up (cancer free) Complications Bleeding4 patients (endoscopic treatment) Follow-up (median 20 months) 1 recurrence (HGD) >> EMR AC sm 3 AC >> Surgery (no residual disease) 2 AC >> Follow-up (cancer free) Complications Bleeding4 patients (endoscopic treatment) Follow-up (median 20 months) 1 recurrence (HGD) >> EMR")
29
EMR and PDT in Barrett’s esophagus Downstaging: 8 (47%) Follow-up 13 months:CR 16 (94%) Complications:stricture 30% bleeding 6% Downstaging: 8 (47%) Follow-up 13 months:CR 16 (94%) Complications:stricture 30% bleeding 6% Buttar, Gastrointest Endosc 2001 17 patients (EMR 1 cm) (PDT 200J/cm 2 )
 Follow-up 13 months:CR 16 (94%) Complications:stricture 30% bleeding 6% Downstaging: 8 (47%) Follow-up 13 months:CR 16 (94%) Complications:stricture 30% bleeding 6% Buttar, Gastrointest Endosc patients (EMR 1 cm) (PDT 200J/cm 2 )")
30
Circumferential EMR Multifocal HGD & IM cancer 5 “visible” and 7 “no visible” lesions Circumferential BE: median length 5 cm Complications: 4/31 EMR sessions (bleeding) Follow-up: no recurrences (median 9 mo) Multifocal HGD & IM cancer 5 “visible” and 7 “no visible” lesions Circumferential BE: median length 5 cm Complications: 4/31 EMR sessions (bleeding) Follow-up: no recurrences (median 9 mo) Seewald et al., Gastrointest Endosc 2003
 Follow-up: no recurrences (median 9 mo) Multifocal HGD & IM cancer 5 visible and 7 no visible lesions Circumferential BE: median length 5 cm Complications: 4/31 EMR sessions (bleeding) Follow-up: no recurrences (median 9 mo) Seewald et al., Gastrointest Endosc 2003")
31
Circumferential EMR in Barrett’s Esophagus 21 pts (19 T1N0; 2 T0N0) EUS 20-MHz Polypectomy snare & saline Circumferential BE: median length 5 cm Complications: 4/21 (bleeding) Follow-up: 2/21 (mean 18 months) 21 pts (19 T1N0; 2 T0N0) EUS 20-MHz Polypectomy snare & saline Circumferential BE: median length 5 cm Complications: 4/21 (bleeding) Follow-up: 2/21 (mean 18 months) Giovannini et al., Endoscopy 2004
 EUS 20-MHz Polypectomy snare & saline Circumferential BE: median length 5 cm Complications: 4/21 (bleeding) Follow-up: 2/21 (mean 18 months) 21 pts (19 T1N0; 2 T0N0) EUS 20-MHz Polypectomy snare & saline Circumferential BE: median length 5 cm Complications: 4/21 (bleeding) Follow-up: 2/21 (mean 18 months) Giovannini et al., Endoscopy 2004")
35
1 st endoscope: lifting 2 nd endoscope:cutting Kuwano et al., Ann Surg 2004 Double Endoscopic Intraluminal Operation (DEILO)
")
38
CP1109264-1 Adenocarcinoma of Cardia with Short Barrett’s

39
Summary Surveillance finds dysplasia or early cancer New endoscopic diagnostic method EMR: long term results awaited EMR for non-dysplastic Barrett’s Surveillance finds dysplasia or early cancer New endoscopic diagnostic method EMR: long term results awaited EMR for non-dysplastic Barrett’s

Similar presentations