Download presentation
Presentation is loading. Please wait.

2
Case scenario: A 36 years old woman with chronic intermittent diarrhea from childhood and weight loss,Abdominal distention and bloating, idiopathic peripheral neuropathy,weakness,fatigue,bone pain and with unexplained iron-deficiency anemia,Folat deficiency, Vitamin D deficiency, abnormal liver function tests that by serologic evaluation and small bowel biopsy and clinical-histologic response to gluten-free diet, established the diognosis of coeliac disease. The patient is worried about risk of malignancy and mortality. Is she in risk of overal mortality compared with the general population?

3
PICO: P:A 36 years old woman known case of coeliac disease.
.I:Coeliac patient .C:Non- coeliac patient .O:Mortality and malignancy

4
all-cause mortality any malignancy and
Meta-analysis: coeliac disease and the risk of all-cause mortality any malignancy and lymphoid malignancy M. Tio, M. R. Cox & G. D. Eslick

5
Celiac Disease Celiac Disease is also called Celiac Sprue and is an auto-immune disease that affects the small intestine. During this presentation, we will discuss this disease and the impacts on health.

6
Celiac disease is common autoimmune disorder and common cause of malabsorption of one or more nutrients.

8
This picture shows the damage that is caused by gluten to the microvilli in someone who suffers from Celiac Disease. As you can see, the image on the left, a healthy intestine, has much greater surface area than the one on the right, damaged by gluten consumption.

10
Celiac disease is considered an "iceberg" disease with a small number of individuals with classical symptoms and manifestations related to nutrient malabsorption

11
The Celiac Iceberg Symptomatic Celiac Disease Manifest mucosal lesion
Silent Celiac Disease Latent Celiac Disease Normal Mucosa Genetic susceptibility: - DQ2, DQ8 Positive serology

12
(1:4500) Classical Celiac Disease Atypical Silent
Latent Detected by screening (1:250)
")
13
:Etiology The etiology of celiac disease is not known, but environmental, immunologic, and genetic factors all appear to contribute to the disease.

14
This depiction is of the 3 components that cause an auto-immune disease: a genetic disposition shown by the pink circle, an environmental trigger, shown in blue and a defected immune system regulation shown here in yellow.

15
Environmental factor is the clear association of the disease with gliadin,a component of gluten that is present in wheat, barley, and rye. In addition to the role of gluten restriction in treatment, the instillation of gluten into both normal-appearing rectum and distal ileum of patients with celiac disease results in morphologic changes within hours.

16
Sources of Gluten OBVIOUS SOURCES Bread Bagels Cakes Cereal Cookies
Pasta / noodles Pastries / pies Rolls

17
Sources of Gluten Candy Communion wafers Cured Pork Products
POTENTIAL SOURCES Candy Communion wafers Cured Pork Products Drink mixes Gravy Imitation meat / seafood Sauce Self-basting turkeys Soy sauce

18
An immunologic component in the pathogenesis of celiac disease is critical Serum antibodies IgA antigliadin, IgA antiendomysial, IgA anti-tTG antibodies—are present. The antiendomysial antibody has 90–95% sensitivity and 90–95% specificity. patients with these antibodies should undergo with .deudenal biopsy

19
Genetic factor(s) are also involved in celiac disease
Genetic factor(s) are also involved in celiac disease. The incidence of symptomatic celiac disease is 10% in first-degree relatives of celiac disease patients. all patients with celiac disease express the HLA-DQ2 or HLA-DQ8 allele, though only a minority of people expressing DQ2/DQ8 have celiac disease. Absence of DQ2/DQ8 excludes the diagnosis of celiac disease.
 are also involved in celiac disease. The incidence of symptomatic celiac disease is 10% in first-degree relatives of celiac disease patients. all patients with celiac disease express the HLA-DQ2 or HLA-DQ8 allele, though only a minority of people expressing DQ2/DQ8 have celiac disease. Absence of DQ2/DQ8 excludes the diagnosis of celiac disease.")
20
{ { Be aware DR3 should now be referred to as DR17 DQ2 DQ8 DR3 DR3/DR3
DQA1*0501 { DQA1*0201 DQA: Any DQ2 DQB1*0201 DQB1*03 CIS CIS Trans APC Gluten

21
Genetics Several genes are involved
The most consistent genetic component depends on the .presence of HLA-DQ (DQ2 and / or DQ8) genes Other genes (not yet identified) account for 60 % of the .inherited component of the disease HLA-DQ2 and / or DQ8 genes are necessary (No DQ2/8, no Celiac Disease!) but not sufficient for the .development of the disease Genes ? ? ? ? HLA + Gluten Celiac Disease
 genes. Other genes (not yet identified) account for 60 % of the .inherited component of the disease. HLA-DQ2 and / or DQ8 genes are necessary (No DQ2/8, no Celiac Disease!) but not sufficient for the .development of the disease. Genes. HLA. + Gluten. Celiac Disease.")
22
:Diagnosis A biopsy should be performed in patients with symptoms and laboratory findings suggestive of nutrient malabsorption and/or deficiency and with a positive endomysial antibody test.

23
The diagnosis of celiac disease requires the presence of characteristic histologic changes on small-intestinal biopsy together with a prompt clinical and histologic response following the institution of a gluten-free diet. If serologic studies have detected the presence of IgA antiendomysial or tTG antibodies, they too should disappear after a gluten-free diet is started.

24
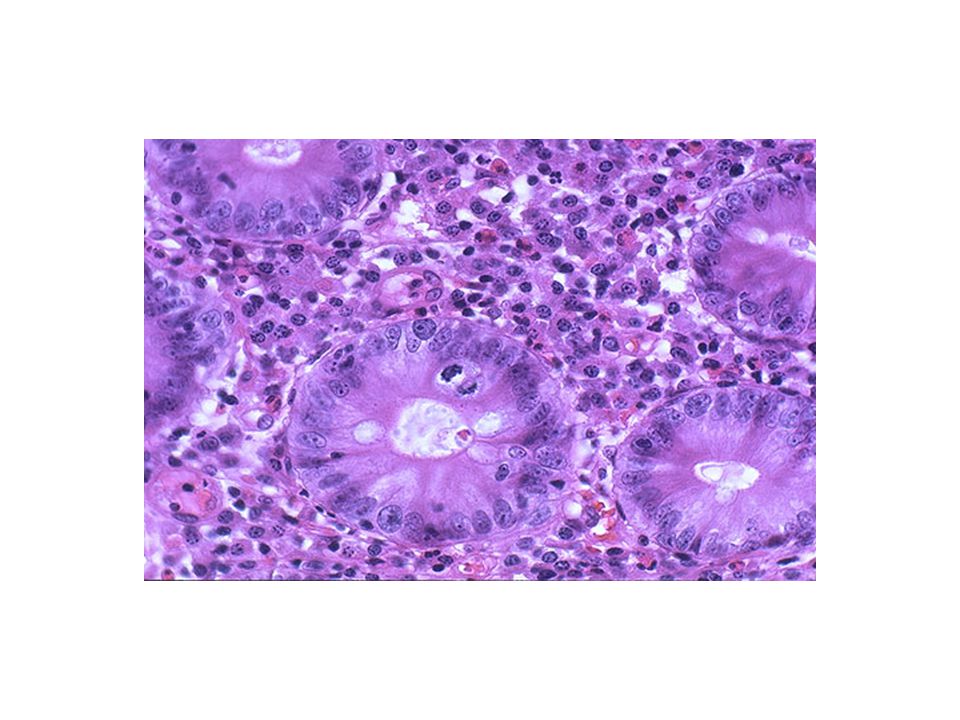
The hallmark of celiac disease is the presence of an abnormal small-intestinal biopsy (Fig ) and the response of the condition—symptoms and the histologic changes on the small-intestinal biopsy—to the elimination of gluten from the diet. The histologic changes have a proximal-to-distal intestinal distribution of severity, which probably reflects the exposure of the intestinal mucosa to varied amounts of dietary gluten.
 and the response of the condition—symptoms and the histologic changes on the small-intestinal biopsy—to the elimination of gluten from the diet. The histologic changes have a proximal-to-distal intestinal distribution of severity, which probably reflects the exposure of the intestinal mucosa to varied amounts of dietary gluten. .")
25
Diagnosis 1st: Physical exam and blood testing 2nd: Duodenal biopsy 3rd: Implement gluten-free diet According to the Celiac Sprue Association, there are three major steps that are taken in order to diagnose a person with Celiac Disease. The first step includes a thorough physical examination to look for any signs of CD (fatigue, weight loss, etc). A blood panel is also conducted, sometimes referred to as a Celiac Blood Panel, to look at other indictors of CD, such as antibodies. Second, a multi-sample biopsy of the duodenal portion of the intestine is done in order to look at possible damage from gluten. The third step includes implementing the gluten-free diet. When the person’s health begins to improve, symptoms start to diminish and the intestinal villi start to repair themselves, Celiac Disease is diagnosed. Please be aware that it is important to keep gluten in the diet for an accurate diagnosis. Removal of gluten too early before seeing a physician can remove signs and symptoms of CD needed for a successful diagnosis. As you can see in this diagram, there are 3 different areas of the intestine. The duodenum is the portion of the intestine that immediately follows the stomach and where biopsy samples are taken to diagnose CD.
. A blood panel is also conducted, sometimes referred to as a Celiac Blood Panel, to look at other indictors of CD, such as antibodies. Second, a multi-sample biopsy of the duodenal portion of the intestine is done in order to look at possible damage from gluten. The third step includes implementing the gluten-free diet. When the person’s health begins to improve, symptoms start to diminish and the intestinal villi start to repair themselves, Celiac Disease is diagnosed. Please be aware that it is important to keep gluten in the diet for an accurate diagnosis. Removal of gluten too early before seeing a physician can remove signs and symptoms of CD needed for a successful diagnosis. As you can see in this diagram, there are 3 different areas of the intestine. The duodenum is the portion of the intestine that immediately follows the stomach and where biopsy samples are taken to diagnose CD.")
26
The classical changes seen on duodenal/jejunal biopsy :are restricted to the mucosa and include 1:an increase in the number of intraepithelial .lymphocytes 2: absence or reduced height of villi, resulting in a flat appearance with increased crypt cell proliferation, resulting in crypt hyperplasia and loss of villous structure, with consequent villous, but not mucosal, .atrophy 3:cuboidal appearance and nuclei that are no longer oriented basally in surface epithelial cells. 4:increased lymphocytes and plasma cells in the lamina propria.

27
Histology of intestinal biopsy in CD Modified Marsh score

28
Normal small intestine Normal villi
Small intestine with villous atrophy Small intestine with scalloping

31
It Takes A Villi Damaged Healthy
The “gold standard” used to diagnose celiac disease is an endoscopy that includes a biopsy of the small intestine. Usually gastroenterologists will only perform an endoscopy with a biopsy of the small bowel after a patient has had several blood tests (usually called a “celiac panel”) that show an increase in one or more antibodies that indicate probable celiac disease. Patients are told to NOT restrict gluten before they are tested because the results of the tests will be skewed. The tests are very sensitive and specific, but can still show a false positive, so that is why it is recommended to wait until a positive biopsy is confirmed before someone is told to follow a gluten free diet for life. The photo on the left shows a blunted villi which has little to no absorptive surfaces as compared to the normal healthy one on the right. Nutrients are absorbed through the villi and with less surface area available for this absorption, fewer nutrients are usually absorbed in the individual with celiac disease.
 that show an increase in one or more antibodies that indicate probable celiac disease. Patients are told to NOT restrict gluten before they are tested because the results of the tests will be skewed. The tests are very sensitive and specific, but can still show a false positive, so that is why it is recommended to wait until a positive biopsy is confirmed before someone is told to follow a gluten free diet for life. The photo on the left shows a blunted villi which has little to no absorptive surfaces as compared to the normal healthy one on the right. Nutrients are absorbed through the villi and with less surface area available for this absorption, fewer nutrients are usually absorbed in the individual with celiac disease.")
32
Duodenum

33
CELIAC DISEASE ENDOSCOPY Normal Scalloped Gluten-free diet HISTOLOGY
Increased IEL Villous atrophy Recovering

34
This is what the small intestine looks like under the microscope when the mucosa is injured like the left photo shows. The villi are essentially flat and numerous lymhocytes are near the surface lining.

35
This endoscopic photo of the small bowel (duodenum) shows the classic fissuring or cobblestoning of the surface as well as "scalloping" of the folds in Celiac disease.
 shows the classic fissuring or cobblestoning of the surface as well as scalloping of the folds in Celiac disease.")
36
This endoscopic photo was taken with special light technique called Narrow Band Imaging (NBI). It brings out some of features of atrophy, fissuring or cobblestone appearance of the mucosa (surface lining) and the "scalloping" of the folds seen in Celiac disease.
 and the scalloping of the folds seen in Celiac disease..")
37
The folds are flattened and the mucosa in this patient with Celiac.

41
Shown here is a pie chart depicting the prevalence of some common symptoms of Celiac Disease. As you see, diarrhea in blue affects about 15% of patients with CD. Infants or children with CD will not develop properly and be classified as failure to thrive (red). Other symptoms that affect CD sufferers include anemia, emotional issues, stomach pain, distended abdomen, vomiting and constipation and a variety of other symptoms.
. Other symptoms that affect CD sufferers include anemia, emotional issues, stomach pain, distended abdomen, vomiting and constipation and a variety of other symptoms..")
42
GI symptoms diarrhea weight loss weakness
pedal edema - protein malabsorption easy bruising - vitamin K malabsorption classic steatorrhea increase in stool mass in most patients

43
Extraintestinal features

44
Hematopoietic anemia - iron or folate deficiency, but also increased blood loss B12 deficiency in severe cases hyposplenism - may resolve with dietary therapy thrombocytosis with Howell-Jolly bodies bleeding diathesis

45
Osteopenic bone disease
decrease Ca absorption decrease in absorption fat-soluble vitamin D binding of Ca and Mg in lumen by unabsorbed dietary fatty acids

46
Osteopenic bone disease
Osteoporosis with bone pain and pathologic fractures paresthesia, muscle cramps and tetany if severe hypocalcemia chronic can result in secondary and even tertiary hyperparthyroidism problems with premenopausal bone mass

47
Neurologic symptoms peripheral neuropathy myopathy cerebellar ataxia
myoclonus cerebral atrophy and dementia cerebral vasculitis brain-stem encephalitis epilepsy and cerebral calcifications

48
Renal and liver disease
Glomerulonephritis IgA nephropathy may respond to gluten-free diet PBC, PSC and chronic active hepatitis elevated transaminases

49
Autoimmune and Connective tissue disease
Vasculitis cryoglobulinemia Sjogren’s syndrome SLE selective IgA deficiency thyroid disease IDDM- and celiac both have HLA-DR3 and DQB1*0201 alleles

50
OB-GYN Impaired fertility in women
high incidence of spontaneous abortion low birth-weight babies reduced breast milk production paripartum exacerbation or first presentation correctable with gluten-free diet

51
Treatment Options Option #1: Remove the genes
Option #2: Remove the grains

52
Treatment Only treatment for celiac disease is a gluten-free diet (GFD) .Strict, lifelong diet Avoid: Wheat Rye Barley

53
:Associated Diseases Celiac disease is associated with dermatitis herpetiformis (DH), Almost all patients with DH have histologic changes in the small intestine consistent with celiac disease, although usually much milder and less diffuse in distribution. Most patients with DH have mild or no gastrointestinal symptoms. Celiac disease is also associated with: Diabetes mellitus type 1 IgA deficiency Down syndrome Turner's syndrome.
, Almost all patients with DH have histologic changes in the small intestine consistent with celiac disease, although usually much milder and less diffuse in distribution. Most patients with DH have mild or no gastrointestinal symptoms. Celiac disease is also associated with: Diabetes mellitus type 1. IgA deficiency. Down syndrome. Turner s syndrome.")
54
Dermatits herpetiformis
Erythematous macule > urticarial papule > tense vesicles Severe pruritus Symmetric distribution 90% no GI symptoms 75% villous atrophy Gluten sensitive

55
Dermatitis Herpetiformis
Skin manifestation of coeliac disease. Raised, red patches, often blistered. Commonly on elbows/knees/buttocks. Symmetrical Skin biopsy, treated with dapsone.

56
The most important complication of celiac disease is the development of cancer.
An increased incidence of both gastrointestinal and nongastrointestinal neoplasms as well as intestinal lymphoma exists in patients with celiac disease. The possibility of lymphoma must be considered whenever a patient with celiac disease previously doing well on a gluten-free diet is no longer responsive to gluten restriction or a patient who presents with clinical and histologic features consistent with celiac disease does not respond to a gluten-free diet.

57
Other complications of celiac disease include the development of intestinal ulceration independent of lymphoma and so-called refractory sprue and collagenous sprue.

58
In the past, patients with celiac disease or DH had been reported to have a 10-fold increased risk for certain gastrointestinal tract malignancies and 40- to 70-fold increased risk for non-Hodgkin's lymphoma (NHL). Recent studies, however, indicate that the increase in risk of malignancy, particularly lymphoma, is much .less than initially believed

59
Small intestinal lymphoma, often multifocal and diffuse, accounts for one half to two thirds of the malignancies complicating celiac disease and typically occurs after 20 to 40 years of disease. Whereas in the general population, most small intestinal lymphomas are of B-cell origin, intestinal lymphoma in celiac disease is typically of T-cell origin. the term EATL (enteropathy-associated T-cell lymphoma) was coined to describe both the intestinal and extraintestinal lymphomas that complicate celiac disease.
 was coined to describe both the intestinal and extraintestinal lymphomas that complicate celiac disease.")
60
EATL commonly is accompanied by mucosal ulceration, as seen in ulcerative jejunoileitis, and these ulcers sometimes are the only endoscopic manifestation of lymphoma. Although some patients with EATL have a partial or temporary response to a strict gluten-free diet, most are eventually unresponsive to gluten withdrawal. In patients whose disease was previously controlled on a gluten-free diet, recurrence of gastrointestinal symptoms (e.g., abdominal pain, weight loss, diarrhea) should raise the clinical suspicion of lymphoma.
 should raise the clinical suspicion of lymphoma.")
61
Other features suggesting lymphoma include: Intestinal obstruction Intestinal bleeding Fever Hypoalbuminemia Lymphadenopathy Erythrophagocytosis evident in bone marrow or the peripheral blood.

62
:Diagnose Small intestinal radiology
enteroscopy with biopsy of the mucosa at multiple levels capsule endoscopy CT or MR scanning. If the index of suspicion is high and studies are not diagnostic, full-thickness biopsy specimens of the small intestine should be obtained at laparoscopy or laparotomy with careful examination of the entire length of the small intestine and examination of mesenteric lymph nodes. Even with such an aggressive approach, EATL can be extremely difficult to diagnose.

63
EATL commonly is fatal: Overall one-year and five-year survival rates of 31% and 11%, respectively, were reported in one small series, with long-term survival almost exclusively confined to those treated with chemotherapy. one third of the remaining malignancies complicating celiac disease. The average patient so affected is older than 50 years. The Swedish study reported elevated risks for small intestinal cancer (standardized incidence ratio,SIR, 10), oropharyngeal cancer (SIR, 2.3), esophageal cancer (SIR, 4.2), and primary liver cancer (SIR, 2.7). Patients with DH also had a slightly increased overall cancer risk (SIR, 1.2) owing to excesses of lymphoma and leukemia, .but they had no increases in gastrointestinal carcinomas
, oropharyngeal cancer (SIR, 2.3), esophageal cancer (SIR, 4.2), and primary liver cancer (SIR, 2.7). Patients with DH also had a slightly increased overall cancer risk (SIR, 1.2) owing to excesses of lymphoma and leukemia, .but they had no increases in gastrointestinal carcinomas .")
64
potential factors : Increased crypt mitotic activity
The mechanisms responsible for the increased prevalence of malignancy in celiac disease are unknown. potential factors : Increased crypt mitotic activity increased turnover of lymphoid cells within the mucosa penetration of the damaged intestinal mucosa by carcinogens infection with oncogenic viruses epithelium underlying abnormalities in the mucosal immune system and surface .

65
the excess risk of malignancies, which was confined to adults, disappeared after a 10-year follow-up. This declining risk of malignancies with increased duration of follow-up, and thus with the length of gluten-free diet, supports the results of a previous study, which indicated that a strict gluten-free diet for five years reduced the risk of all malignancies, not just EATL, to that of the general .population

66
all-cause mortality any malignancy and
Meta-analysis: coeliac disease and the risk of all-cause mortality any malignancy and lymphoid malignancy M. Tio, M. R. Cox & G. D. Eslick

67
:INTRODUCTION Coeliac disease is a common autoimmune disorder, with a prevalence approaching 1% in the United States. Although it is classically associated with malabsorption and the attendant complications that can arise from the malabsorptive state, it has also been associated with an increased risk of lymphoid malignancies. This association is particularly clear in the case of a specific non-Hodgkin lymphoma (NHL) subtype, enteropathy-associated Tcell lymphoma (EATL), which has been long established as a complication of coeliac .disease
 subtype, enteropathy-associated Tcell lymphoma (EATL), which has been long established as a complication of coeliac .disease")
68
The magnitude of the risk of other forms of lymphoid malignancies is much less clear. Data on lymphoid malignancy risk other than NHL are scant, and the risk estimates for the more commonly reported NHL vary significantly. Similarly, whether coeliac disease increases the overall risk of malignancy or not remains unknown, with large discrepancies in reported estimates. Coeliac disease has also been associated with an increased risk of all-cause mortality, although again, the estimates vary widely, ranging from no association to a 3.9-fold increased risk.

69
:METHODS :Search strategy Relevant articles were identified by one reviewer (M.T.) by systematically searching through MEDLINE (from 1950), PubMed (from1946),EMBASE (from 1949) and Current Contents Connect (from 1998) through to 4 January 2012. No language restrictions were used in either the search or study selection. A search for unpublished literature was not performed.
 by systematically searching through MEDLINE (from 1950), PubMed (from1946),EMBASE (from 1949) and Current. Contents Connect (from 1998) through to 4. January No language restrictions were used in either the search or study selection. A search for unpublished literature was not performed.")
70
:Study selection To be included, eligible studies needed to:1-have a study design of either a cohort or case control; 2-report the risk of all-cause mortality, any specific mortality any malignancy or any lymphoid malignancy .in coeliac patients 3-report the risk point estimate as an odds ratio (OR), hazard rate or relative risk. 4-report the 95% confidence interval (CI) for the point estimate. 5-use an internal comparison when calculating the risk estimate.
, hazard rate or relative risk. 4-report the 95% confidence interval (CI) for the point estimate. 5-use an internal comparison when calculating the risk estimate.")
71
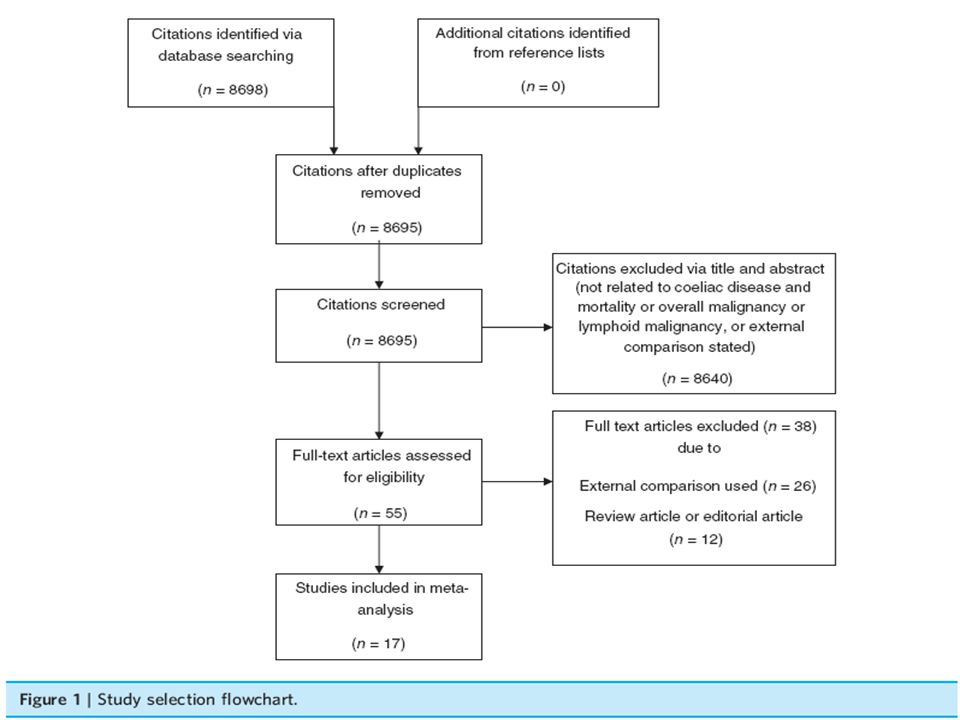
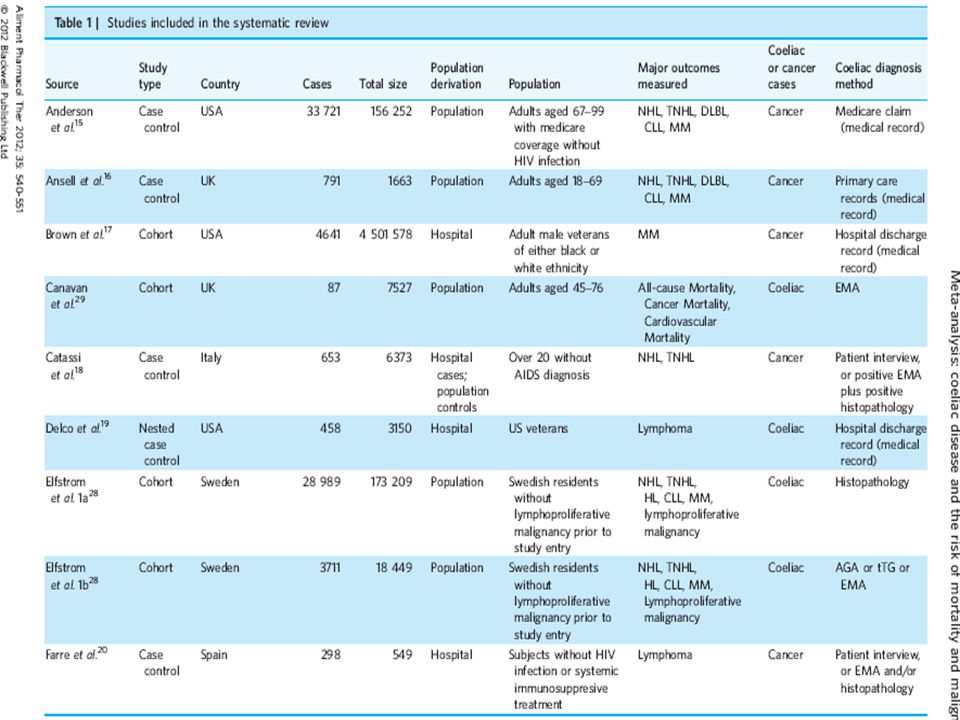
:RESULTS From 8698 citations screened by our search, we identified a total of 17 observational studies that met our inclusion criteria (Figure 1). Table 1 shows selected characteristics of the identified studies.2, 8, 15–29. In terms of study design, nine were case control studies and eight were cohort studies. There was heterogeneity in the method of coeliac disease diagnosis, with six studies using medical records, one study using patient interview, three studies using patient interview or positive serology plus positive histopathology and two studies using positive histopathology. Latent or undiagnosed coeliac disease was used as a coeliac disease subtype diagnosis in seven studies, with two studies using positive eurospital tissue-transglutaminase antibodies (Eu-tTG) plus positive endomysial antibodies (EMA) or positive celikey tissue-transglutaminase antibodies (celikey-tTG), two studies using positive tTG plus positive EMA, two studies using positive tTG or positive EMA or positive antigliadin antibody and two studies using positive EMA alone.
. Table 1 shows selected characteristics of the identified studies.2, 8, 15–29. In terms of study design, nine were case control studies and eight were cohort studies. There was heterogeneity in the method of coeliac disease diagnosis, with six studies using medical records, one study using patient interview, three studies using patient interview or positive serology plus positive histopathology and two studies using positive histopathology. Latent or undiagnosed coeliac disease was used as a coeliac disease subtype diagnosis in seven studies, with two studies using positive eurospital tissue-transglutaminase antibodies (Eu-tTG) plus positive endomysial antibodies (EMA) or positive celikey tissue-transglutaminase antibodies (celikey-tTG), two studies using positive tTG plus positive EMA, two studies using positive tTG or positive EMA or positive antigliadin antibody and two studies using positive EMA alone.")
76
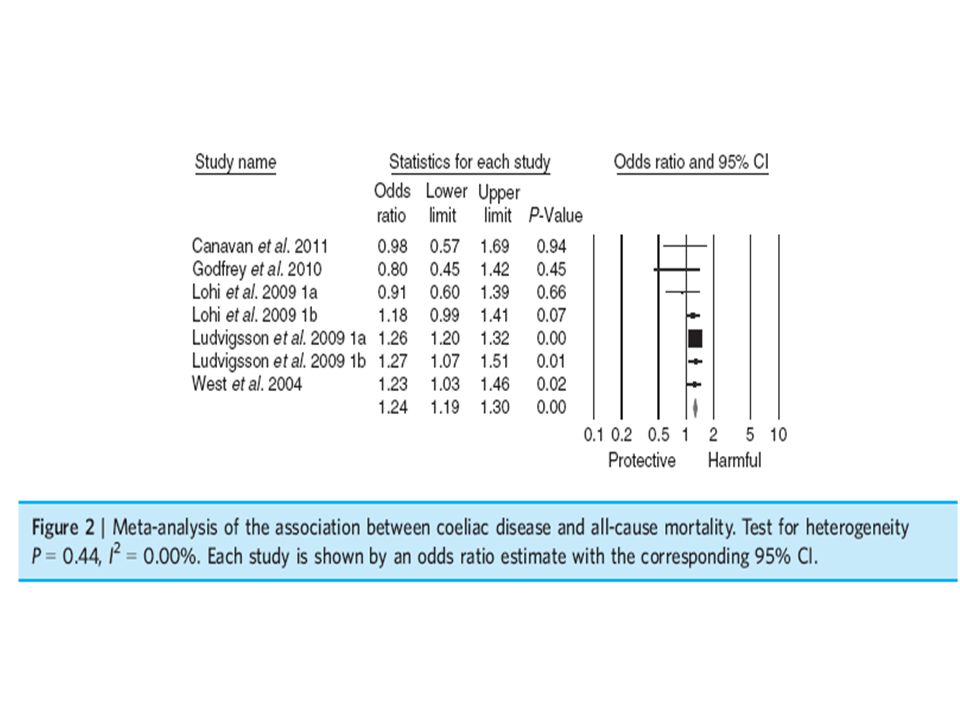
All-cause mortality: the all-cause mortality meta-analysis of five prospective studies[8, 22, 24, 26, 29] comprising of coeliac cases with a total of individuals, indicating that coeliac patients are at an increased risk of all-cause mortality with a pooled OR of 1.24 (95% CI 1.19–1.30). There was .no significant heterogeneity
. There was .no significant heterogeneity.")
78
:Non-Hodgkin lymphoma
Eight studies[15, 16, 18, 21, 23, 25, 27, 28] (six case control studies and two cohort studies) comprising of cancer or coeliac cases with a total of individuals were identified for the non-Hodgkin lymphoma (NHL) meta-analysis. Coeliac patients were at significantly increased risk of NHL.This resulted in a pooled OR of 2.61 (95% CI 2.04–3.33), .with no significant heterogeneity
 comprising of cancer or coeliac cases with a total of individuals were identified for the non-Hodgkin lymphoma (NHL) meta-analysis. Coeliac patients were at significantly increased risk of NHL.This resulted in a pooled OR of 2.61 (95% CI 2.04–3.33), .with no significant heterogeneity.")
80
:T-cell non-Hodgkin lymphoma
Five studies[15, 16, 18, 25, 28] (four case–control studies, one cohort study) comprising of cancer cases with a total of individuals were identified for the TNHL meta-analysis. The risk of TNHL was significantly elevated, with a pooled OR of (95% CI 7.85–31.94) (Figure 4). There was no significant heterogeneity (I2 = 55.6%, P = 0.06).
 comprising of cancer cases with a total of individuals were identified for the TNHL meta-analysis. The risk of TNHL was significantly elevated, with a pooled OR of (95% CI 7.85–31.94) (Figure 4). There was no significant heterogeneity (I2 = 55.6%, P = 0.06).")
82
:Any malignancy Three prospective studies[8, 23, 26] (two cohort studies, one nested case–control study) comprising of 5134 cancer or coeliac cases with a total of individuals were identified for the any malignancy meta-analysis. There was no association between coeliac disease and the risk of any malignancy, with a pooled OR of 1.07 (CI 0.89–1.29) (Figure 5). There was no significant heterogeneity (I2 = 0%, P = 0.58).
 comprising of 5134 cancer or coeliac cases with a total of individuals were identified for the any malignancy meta-analysis. There was no association between coeliac disease and the risk of any malignancy, with a pooled OR of 1.07 (CI 0.89–1.29) (Figure 5). There was no significant heterogeneity (I2 = 0%, P = 0.58).")
84
Cause specific mortality and other :lymphoid malignancies
As shown in Table 2, we found that coeliac patients had an increased risk of cardiovascular mortality 1.19 (95% CI 1.12–1.27), lymphoproliferative disease/malignancy 2.53 (95% CI 1.59–4.04), Hodgkin lymphoma 2.01 (95% CI 1.01–4.01) and diffuse large cell B-lymphoma 2.25 (95% CI 1.32–3.85). There was no increased risk of any malignancy mortality 1.24 (95% CI 0.96–1.60), lymphoma 1.99 (95% CI 0.29–13.58), chronic lymphocytic leukaemia 0.80 (95% CI 0.46–1.38) or multiple myeloma 1.26 (95% CI 0.83–1.90). However, all of these results are based on pooling .together only two or three studies
, lymphoproliferative disease/malignancy 2.53 (95% CI 1.59–4.04), Hodgkin lymphoma 2.01 (95% CI 1.01–4.01) and diffuse large cell B-lymphoma 2.25 (95% CI 1.32–3.85). There was no increased risk of any malignancy mortality 1.24 (95% CI 0.96–1.60), lymphoma 1.99 (95% CI 0.29–13.58), chronic lymphocytic leukaemia 0.80 (95% CI 0.46–1.38) or multiple myeloma 1.26 (95% CI 0.83–1.90). However, all of these results are based on pooling .together only two or three studies")
86
:Discussion Our systematic review and meta-analysis shows that coeliac patients are at an increased risk of mortality, and are at a substantially increased risk of NHL and TNHL. Serologically defined coeliac patients are at a similarly increased risk of both NHL and mortality. However, coeliac patients do not have an increased .risk of any malignancy overall

87
The all-cause mortality results:
This raises the possibility that as the current pooled mortality risk estimate is based on an average of 13.4 years of follow up, this may in fact be an underestimate of the true risk. Further prospective studies with a longer follow-up are needed to determine if the mortality risk is higher than the current estimate. However, our estimate still needs to be interpreted with caution, as it is limited by the availability of only six studies to analyse, combined with the heterogeneity in coeliac disease diagnosis method between studies. Nonetheless, it is likely that our pooled result is the most .reliable estimate currently available

88
This increased risk of all-cause mortality in coeliac patients may be partly explained by our findings that coeliac patients have an increased risk of cardiovascular mortality. our cardiovascular mortality result is based on only three studies, more studies using internal comparisons are required to determine this association. Further studies examining specific mortality risks among coeliac patients may help guide future studies on whether any preventative measures beyond the gluten free diet .could be taken to minimise mortality

89
:Any malignancy and coeliac disease
No association between the risk of any malignancy and .coeliac disease was found in our pooled risk estimate It is not clear how an increased risk of any malignancy overall is not found when there is a clear increased risk of NHL, although one study[36] found a decreased risk of breast cancer in coeliac disease. If coeliac disease decreases the risk of certain non-lymphoid malignancies, it may explain why there is no increased risk of any malignancy overall. Further study into the possibility of decreased cancer risks other than NHL may be warranted. However, it is possible that the lack of increased risk is due to a lack of statistical power, given .low absolute risk of NHL

90
The serology subgroup analysis found that serologically diagnosed coeliac patients had an increased risk of mortality and NHL compared with non-coeliac patients. These results suggest that serologically defined coeliac patients may be subject to a similar level of risk as coeliac patients diagnosed by other means. However, given that these results are only marginally significant, further research into clarifying any association between positive coeliac serology and NHL .is warranted and mortality

91
We were not able to determine from our systematic review and meta-analysis if compliance with a gluten-free diet had any effect on the risk of mortality and NHL in coeliac patients. There is evidence suggesting that the gluten-free diet decreases the risk of mortality and malignancy; however, some studies have not found this association. Future studies should include measurement of .compliance with the gluten-free diet

92
Our systematic review and meta-analysis shows that coeliac patients are at an increased risk of mortality and non-Hodgkin lymphoma, but do not have an increased risk of any malignancy overall. Serologically defined coeliac patients also have an elevated risk of mortality and non-Hodgkin lymphoma. Our results are limited by the small number of studies available for analysis, and by heterogeneity in diagnostic methods. More studies using internal comparators are needed, particularly to more accurately determine the risk of NHL and mortality in both serologically defined .and histologically defined coeliac patients :Conclusion

93
THANKS FOR YOUR ATTENTION

Similar presentations














 the immune system reacts abnormally.>")

















