Download presentation
Presentation is loading. Please wait.

1
What's the Best Brew for Grandma? 2012 Beers List Update Hospitalist Best Practice J Rush Pierce Jr, MD, MPH June 20, 2012

2
Disclosures I am member and serve on Emergency Preparedness Special Interest Group for the American Geriatrics Society, who played a major role in the 2012 Beers update 5% of my salary supported by Donald W Reynolds Foundation for education of hospital care of the elderly

3
Agenda Background of Beers list (rationale, history, methodology of update) Focused review of update Usefulness and limitations Relevance to hospital medicine/resources
 Focused review of update Usefulness and limitations Relevance to hospital medicine/resources")
4
What the Beers list is not

5
Beers list - background 1991 – for use in NH’s 1997 – update for elderly in all settings 1999 – adopted by CMS for NH regulation 2003 – update; adopted by Medicare D, HEDIS, NCQA 2012 – evidence-based update

6
Case Q1 82 y/o white man admitted with CAP, now ready to go home after completion of CAP rx. PMHx: diabetes, HTN, painful diabetic neuropathy Home meds : glyburide, lovastatin, clonidine, ASA, amitriptyline, pantoprazole Q1 How many of these meds are on the Beers list? Q2 What will you send the patient home on?

7
Case Q2 77 y/o woman with dementia has recurrent UTI’s and nausea. Urology suggests long-term suppressive therapy. Recent organisms have been sensitive to nitrofurantoin and Bactrim. Q1 What is best choice for urinary suppression? Q2 What drug is best choice for nausea?

8
Criticisms of previous Beers list iterations Not evidence-based Many drugs on list were infrequently used Unstructured Uncertain relevance to clinical practice – Many studies settings show that 20 – 30% of patients on Beers list meds – Inconsistent assoc with ADE in epidemiologic studies

9
NEISS-CADES Setting: 53 US hospitals Patients: 5077 pts > 64 years adm to hospital for ADE Findings: – Half of hospitalizations were for pts >79 yrs old – Two-thirds due to warfarin (33.3%), insulins (13.9%), oral antiplatelet agents (13.3%), and oral hypoglycemic agents (10.7%). – Beers medications were implicated in 6.6% of hospitalizations for ADE, half of these digoxin Source: NEJM 2011;365:2002

10
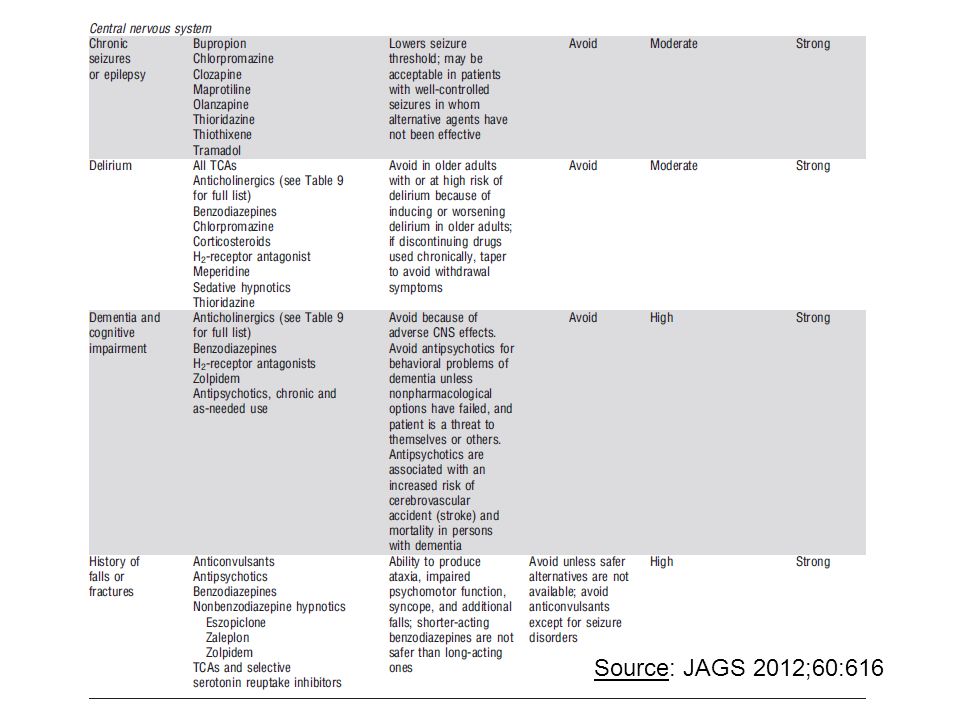
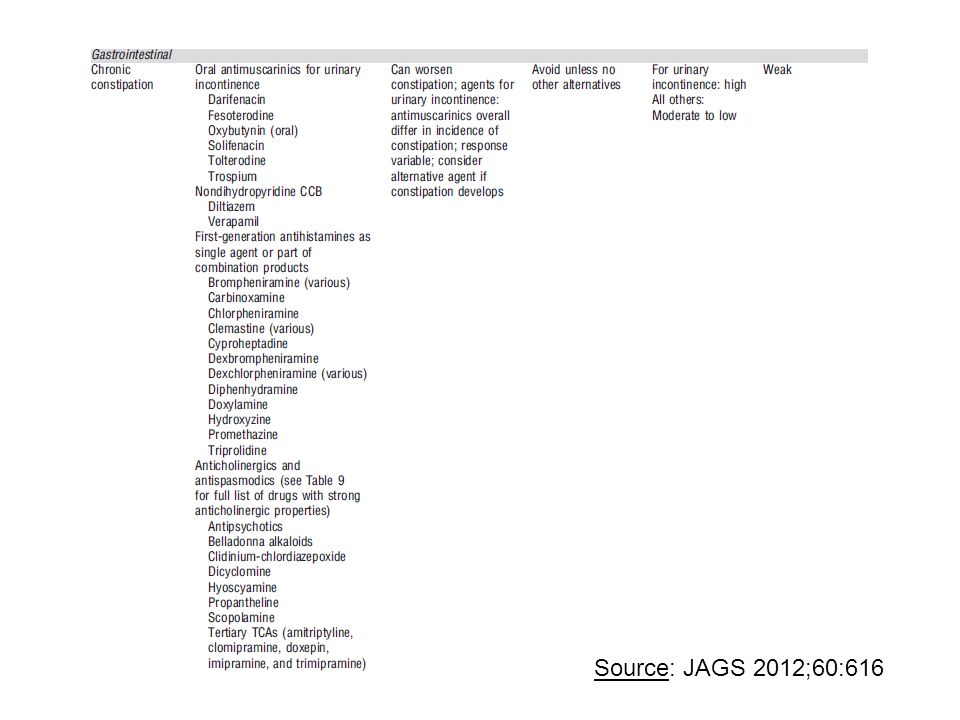
2012 Beers Update Evidence-based approach by American Geriatric Society Incorporate exceptions Divide into three categories (Drugs to avoid, Drug-disease/syndrome interactions, Drugs to use with caution) Publish grade of evidence and strength of recommendation
 Publish grade of evidence and strength of recommendation")
11
Evidence grade and strength of recommendations Grade of evidence – High (>1 RCT or multiple consistent high quality observational studies) – Moderate (1 RCT, or multiple consistent lower quality observational studies) – Low (important study design flaws, inconsistent findings among studies) Strength of recommendations – Strong (risk/burden clearly > benefit) – Weak (benefits finely balanced with risk/burden) – Insufficient (insufficient evidence to determine)
 – Moderate (1 RCT, or multiple consistent lower quality observational studies) – Low (important study design flaws, inconsistent findings among studies) Strength of recommendations – Strong (risk/burden clearly > benefit) – Weak (benefits finely balanced with risk/burden) – Insufficient (insufficient evidence to determine)")
12
Anticholinergics Source: JAGS 2012;60:616

13
Antibiotics Source: JAGS 2012;60:616

14
Cardiovascular drugs Source: JAGS 2012;60:616

15
Cardiovasc drugs (contd) Source: JAGS 2012;60:616
 Source: JAGS 2012;60:616")
16
Psych drugs Source: JAGS 2012;60:616

17
Psych drugs (contd) Source: JAGS 2012;60:616
 Source: JAGS 2012;60:616")
18
Endocrine drugs Source: JAGS 2012;60:616

19
Pain Source: JAGS 2012;60:616

20
Drug – disease/synd interactions Source: JAGS 2012;60:616

24
Drugs to use with caution Source: JAGS 2012;60:616

25
Beers criteria and outpt studies Chang et al (Pharmacotherpy 2005;25:831) – Setting: Taiwan – Patients: 550 older pts seen in outpt clinic – Findings: ADE OR = 15 Budnitz et al (Ann Intern Med 2007;147:755) – Setting: Brazil – Patients: 186 older outpts – Findings: ADE OR = 2.3
 – Setting: Taiwan – Patients: 550 older pts seen in outpt clinic – Findings: ADE OR = 15 Budnitz et al (Ann Intern Med 2007;147:755) – Setting: Brazil – Patients: 186 older outpts – Findings: ADE OR = 2.3")
26
Beers criteria and hosp studies Onder et al (Eur J Clin Pharmacol 2005;61:453) – Setting: Italy – Patients: 5,152 older pts adm to hosp – Findings: No assoc Beers list and ADE, LOS or mortality LaRoche et al (Brit J Clin Pharm 2007;63:177) – Setting: France – Patients: 2,018 pts > 70 adm to hosp – Findings: more ADR in pts on Beers list meds, but no diff in ADR attributable to Beers meds
 – Setting: Italy – Patients: 5,152 older pts adm to hosp – Findings: No assoc Beers list and ADE, LOS or mortality LaRoche et al (Brit J Clin Pharm 2007;63:177) – Setting: France – Patients: 2,018 pts > 70 adm to hosp – Findings: more ADR in pts on Beers list meds, but no diff in ADR attributable to Beers meds")
27
Beers and hospital studies Franceschi M, et al (Drug Safety 2008;31:545) – Setting: Italy – Patients: 1,756 older pts adm to hospital – Findings: 4.4% of hospitalizations related to ADE that was definitely or possibly avoidable 1/5 of these (<1% or adms) had received an inappropriate med Budnitz et al (Ann Intern Med 2007;147:755) – Setting: US – Patients: 177,504 older pts seen in ED – Findings: No association between Beers meds and ADE
 – Setting: Italy – Patients: 1,756 older pts adm to hospital – Findings: 4.4% of hospitalizations related to ADE that was definitely or possibly avoidable 1/5 of these (<1% or adms) had received an inappropriate med Budnitz et al (Ann Intern Med 2007;147:755) – Setting: US – Patients: 177,504 older pts seen in ED – Findings: No association between Beers meds and ADE")
28
BEERS vs STOPP (Hamilton. Arch Intern Med 2011; 171:1013) STOPP = Screening Tool of Older Persons’ potentially inappropriate Prescriptions Setting: Ireland Patients: 600 pts > 64 years adm to hosp Findings: – ADE 26% – 2/3 ADE causal or contributory to adm – OR ADE 1.84 (95% CI = 1.51 – 2.26) with STOPP, 1.27 (95% CI = 0.94 – 1.72) with Beers
 STOPP = Screening Tool of Older Persons’ potentially inappropriate Prescriptions Setting: Ireland Patients: 600 pts > 64 years adm to hosp Findings: – ADE 26% – 2/3 ADE causal or contributory to adm – OR ADE 1.84 (95% CI = 1.51 – 2.26) with STOPP, 1.27 (95% CI = 0.94 – 1.72) with Beers.")
29
Source: Arch Intern Med 2011;171:1013

33
Source:http://www.bgs.org.uk/powerpoint/aut10/Mahony_inappropriate_prescribing.pdf

36
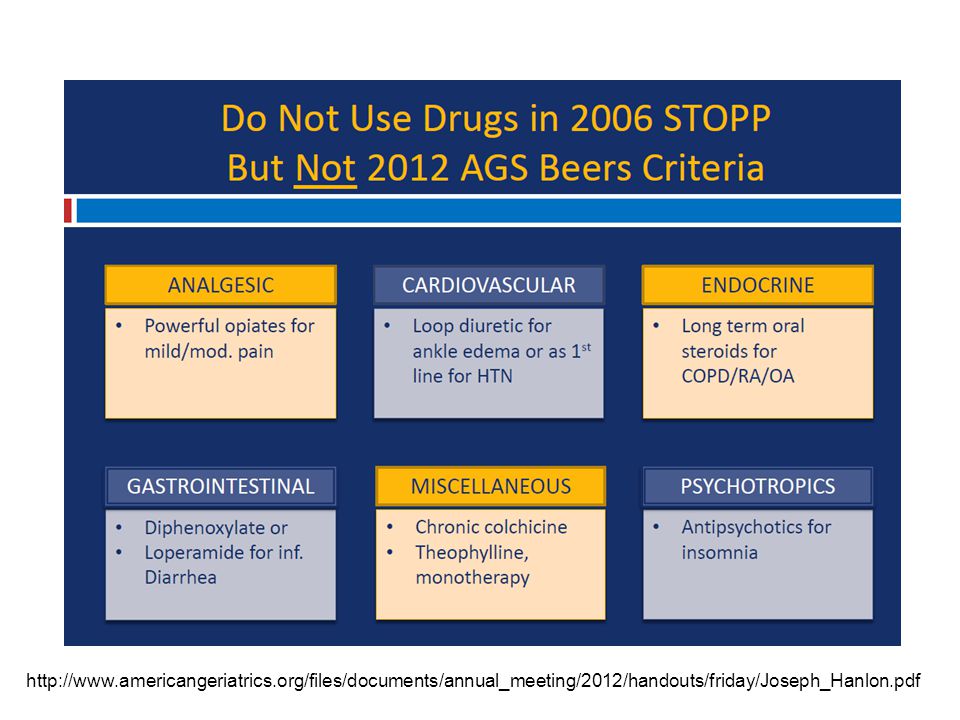
http://www.americangeriatrics.org/files/documents/annual_meeting/2012/handouts/friday/Joseph_Hanlon.pdf
37
Case Q1 82 y/o white man admitted with CAP, now ready to go home after completion of CAP rx. PMHx: diabetes, HTN, painful diabetic neuropathy Home meds : glyburide, lovastatin, clonidine, ASA, amitriptyline, pantoprazole Q1 How many of these meds are on the Beers list? Q2 What will you send the patient home on?

38
Case Q2 77 y/o woman with dementia has recurrent UTI’s and nausea. Urology suggests long-term suppressive therapy. Recent organisms have been sensitive to nitrofurantoin and Bactrim. Q1 What is best choice for urinary suppression? Q2 What drug is best choice for nausea?

39
Beers and Relevance to Hospital Medicine Education/resources (google AGS) Avoid starting Beers/STOPP meds in hospital – Phenergan, benzos If Beers/STOPP meds started in hospital, consider stopping before go home – Antipsychotics, opiates, zolpidem, ?loop diuretics for edema not due to CHF or cirrhosis For patients on Beers/STOPP meds on admission, consider communicating with PCP Redo admission order set; clinical decision support
 Avoid starting Beers/STOPP meds in hospital – Phenergan, benzos If Beers/STOPP meds started in hospital, consider stopping before go home – Antipsychotics, opiates, zolpidem, loop diuretics for edema not due to CHF or cirrhosis For patients on Beers/STOPP meds on admission, consider communicating with PCP Redo admission order set; clinical decision support")
Similar presentations