Download presentation
Presentation is loading. Please wait.

1
WESLEY VALDES D.O. Telemedicine and Remote Monitoring

2
Wesley Valdes D.O. University of Illinois at Chicago Acting Medical Director Office of Telehealth Research and Innovation Assistant Professor of Clinical Surgery Section of Wound Healing and Tissue Repair Clinical Assistant Professor Biomedical and Health Information Sciences

3
Wesley Valdes D.O. Take care of Patients Improve Patient’s Health (when possible) Perform professionally and responsibly
 Perform professionally and responsibly.")
4
Opportunity Health Care Reform in Kuwait By reorganizing the way data is collected and managed, chronic diseases outcomes can be greatly affected Healthier population Reduction in cost of care (i.e. less complications) More efficient care Manage resources more appropriately Increase quality
 More efficient care Manage resources more appropriately Increase quality.")
5
What to remember! Centralization of clinical data in monitored centers can significantly improve patient care Government or non-profit supported data centers can enhance adoption of physician participation Remote patient monitoring is a proven process than can help physicians manage patients, improve quality of care, and significantly reduce cost of care.

6
Fact Advances in information technology have surpassed the current business model of medicine

7
The Business Model of Medicine Ambulatory Patient Care Designed for Acute Care You saw a doctor when you were sick

9
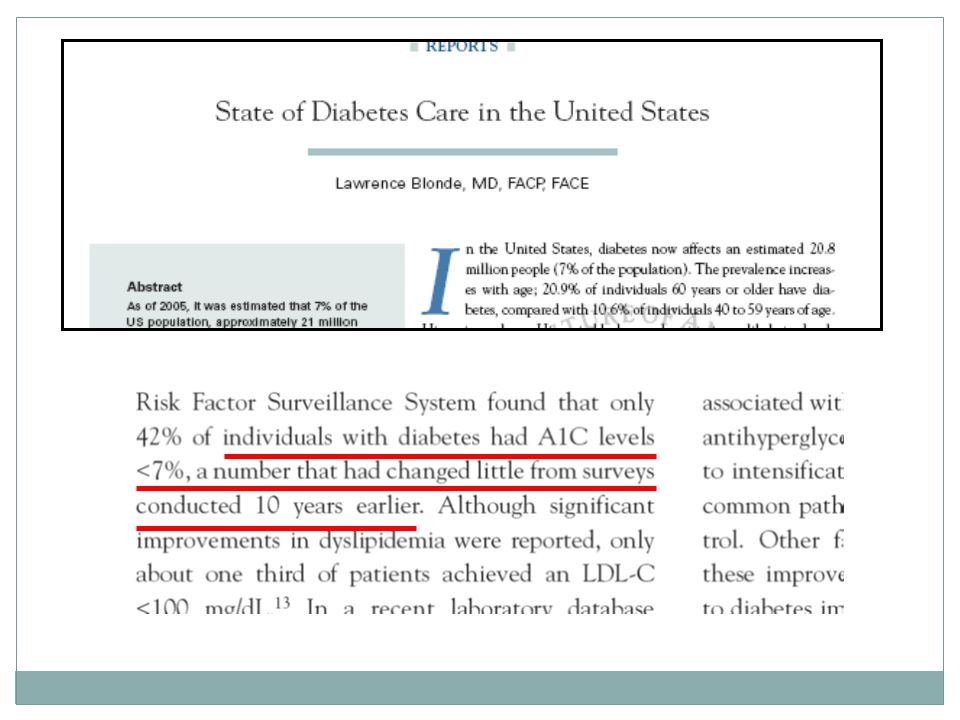
Chronic Disease Diabetes Obesity Hypertension Hyperlipidemia Asthma Coronary Artery Disease

11
Hospital Medicine Chronic Diseases

12
Telemedicine Arizona Telemedicine Program $2,600,000 savings over 6 month study Department of Corrections $1,000,000 annual cost savings

13
Chronic Care

18
Efficiency ≠ Quality Quality + Efficiency = Efficient Quality

19
Care-Giver Focused Department Focused Progression from Back Office to Bedside: Accounting Billing Registration Order Processing Operational Support Clinical Support Laboratory, Radiology, Pharmacy, Etc. Care Plans, Nursing Documentation, Physician Order Entry, Etc.

21
Healthcare and Advances in Technology 1960s Enactment of Medicaid and Medicare Cost-based reimbursement Focus on financial needs 1970s Still focused on financial and accounting systems Technology focused on mainframes 1980s PPS introduces focus on cost containment PCs coming into vogue Ancillary support expanding 1990s More pressures on cost reduction Technology begins to gain focus as a quality improvement vehicle Integration becomes the key, how to service clinicians with disparate systems 2000s Patient safety becomes a focus CPOE becomes huge Mobility and universal connectivity opens new opportunities and challenges

22
PROFESSIONAL ISSUES EMRs don't guarantee quality care, a review of 50,000 patient records shows on 14 of 17 measures, physicians using paper records did equally well as those using EMRs. They even outperformed electronic record users in one area. By Kevin B. O'Reilly, AMNews staff. Aug. 13, 2007.Kevin B. O'Reilly Electronic Health Record Use and the Quality of Ambulatory Care in the United States Jeffrey A. Linder; Jun Ma; David W. Bates; Blackford Middleton; Randall S. Stafford Arch Intern Med. 2007;167:1400-1405. EMRs don't guarantee quality care!

23
Quality indicatorEMRNo EMR Antithrombotic therapy for atrial fibrillation54%60% Aspirin use for coronary artery disease45%40% Beta-blocker use for coronary artery disease40%38% Diuretic and beta-blocker use for hypertension64%60% Statin use*33%47% Inhaled corticosteroid use for asthma44% Treatment of depression82%86% No benzodiazepine use for depression*91%84% Selected antibiotic use for acute otitis media68%67% Smoking cessation counseling30%23% Diet counseling for high-risk adults28%33% Exercise counseling for high-risk adults20%21% Blood pressure check68%71% No routine electrocardiogram97%96% No routine urinalysis*94%91% No routine hemoglobin/hematocrit86% Avoiding potentially inappropriate prescribing in elderly patients93%

24
Quality indicatorEMRNo EMR Antithrombotic therapy for atrial fibrillation54%60% Aspirin use for coronary artery disease45%40% Beta-blocker use for coronary artery disease40%38% Diuretic and beta-blocker use for hypertension64%60% Statin use*33%47% Inhaled corticosteroid use for asthma44% Treatment of depression82%86% No benzodiazepine use for depression*91%84% Selected antibiotic use for acute otitis media68%67% Smoking cessation counseling30%23% Diet counseling for high-risk adults28%33% Exercise counseling for high-risk adults20%21% Blood pressure check68%71% No routine electrocardiogram97%96% No routine urinalysis*94%91% No routine hemoglobin/hematocrit86% Avoiding potentially inappropriate prescribing in elderly patients93%

25
Quality indicatorEMRNo EMR Antithrombotic therapy for atrial fibrillation54%60% Aspirin use for coronary artery disease45%40% Beta-blocker use for coronary artery disease40%38% Diuretic and beta-blocker use for hypertension64%60% Statin use*33%47% Inhaled corticosteroid use for asthma44% Treatment of depression82%86% No benzodiazepine use for depression*91%84% Selected antibiotic use for acute otitis media68%67% Smoking cessation counseling30%23% Diet counseling for high-risk adults28%33% Exercise counseling for high-risk adults20%21% Blood pressure check68%71% No routine electrocardiogram97%96% No routine urinalysis*94%91% No routine hemoglobin/hematocrit86% Avoiding potentially inappropriate prescribing in elderly patients93%

26
Abnormal Finding Action by Healthcare professional TIME

27
Abnormal Finding Action by Healthcare professional TIME

28
Abnormal Finding Action by Healthcare professional TIME Patient follows plan

29
Communication Evidence based decisions Enhanced measurement Compliance Clinical IntegrationChronic Disease Management Members of a health care team working in concert to implement a plan of care. Members of a healthcare team including the patient working in concert to implement a plan of care. Communication Evidence based decisions Enhanced measurement Compliance Behavior Change Management

30
Key Points Technology has made a lot of data almost instantaneously available Traditional physician offices are not set up to manage large amounts of clinical data Clinical outcomes can be significantly improved with better data management Technology is available that can assist and enhance physician performance

31
Physician Enablers Radiological imaging Robotic Surgery Drug Alerts Diagnostic arbiters

32
Telemedicine vs. Telehealth Medical care provided via telecommunications technologies Delivery of health- related services and information via telecommunications technologies

33
TELE - HEALTH TELE - MEDICINE

34
Tele-health Home monitoring – patient safety Gas leaks Alzheimer patient alarms Bed wetting Water overflow (sinks and baths) Fall alarms Telecom activated Key boxes 911 / Healthcare interoperability
 Fall alarms Telecom activated Key boxes 911 / Healthcare interoperability")
35
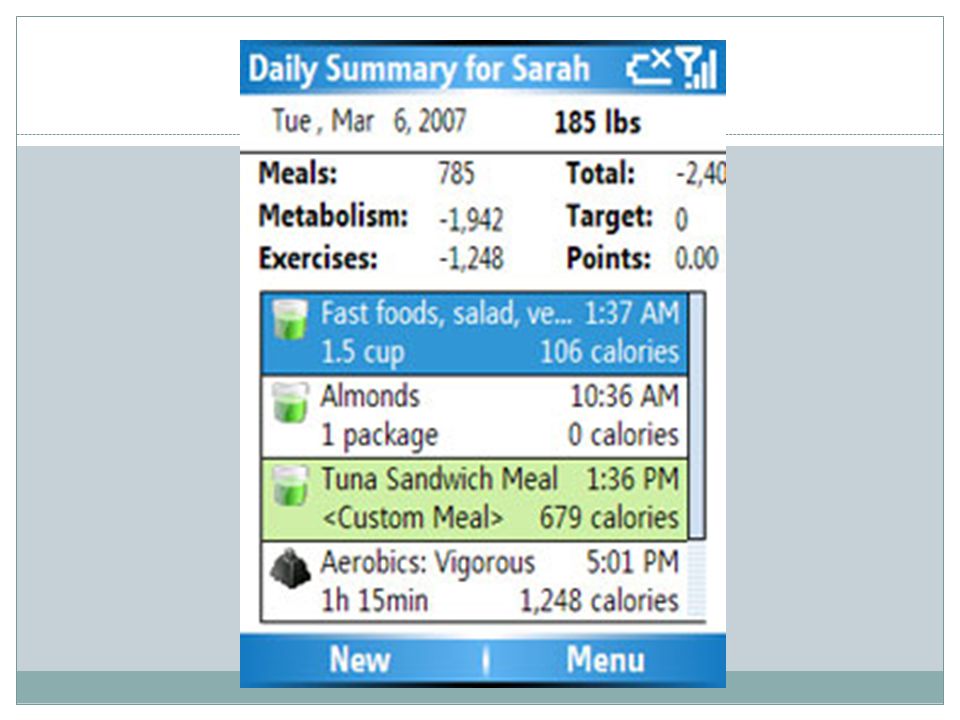
Tele – health / medicine Home patient education Patient data monitors

37
Real Time Technology Utilization of cellular networks

40
Diabetes – helping change Real time availability of data allows – Utilization of resources Early identification of poor control Rapid response to non-compliance Increased compliance Improved communication between patients and providers Better clinical control

41
Shea Study A Novel Solution for Remote Training of Home Telemedicine Patients Albert M. Lai 1, MPhil, Justin Starren 2, MD, PhD, Steven Shea 3, MD, MS 1 Department of Biomedical Informatics, Columbia University College of Physicians and Surgeons, New York, NY; 2Departments of Biomedical Informatics and Radiology, Columbia University College of Physicians and Surgeons, New York, NY; 3Departments of Medicine, Epidemiology, and Biomedical Informatics, Columbia University College of Physicians and Surgeons, New York, NY

42
HOMEHELPFEEDBAC K SUBSCRI P T I O N S ARCHIVESEARCHTABLE OF C O N T E N T S First published October 12, 2005 as JAMIA PrePrint; doi:10.1197/jamia.M1917 J Am Med Inform Assoc. 2006;13:40-51. DOI 10.1197/jamia.M1917. © 2006 American Medical Informatics AssociationAmerican Medical Informatics Association Research Paper A Randomized Trial Comparing Telemedicine Case Management with Usual Care in Older, Ethnically Diverse, Medically Underserved Patients with Diabetes Mellitus Steven Shea, MD, Ruth S. Weinstock, MD, PhD, Justin Starren, MD, PhD, Jeanne Teresi, EdD, PhD, Walter Palmas, MD, Lesley Field, RN, MSN, Philip Morin, MS, Robin Goland, MD, Roberto E. Izquierdo, MD, L. Thomas Wolff, MD, Mohammed Ashraf, BA, Charlyn Hilliman, MPA, Stephanie Silver, MPH, Suzanne Meyer, RN, Douglas Holmes, PhD, Eva Petkova, PhD, Linnea Capps, MD, Rafael A. Lantigua, MD for the IDEATel Consortium This Article Full Text Full Text (PDF) All Versions of this Article: M1917v1 13/1/40 most recent M1917v1 Submit a response Alert me when this article is cited Alert me when eLetters are posted Alert me if a correction is posted Services Similar articles in this journal Similar articles in PubMed Alert me to new issues of the journal Download to citation manager Citing Articles Citing Articles via HighWire Citing Articles via Google Scholar Google Scholar Articles by Shea, S. Search for Related Content PubMed PubMed Citation Articles by Shea, S. J Am Med Inform Assoc. 2006;13:40-51. DOI 10.1197/jamia.M1917 8.35% to 7.42% in the subgroup with baseline HgbA1c 7% (n = 353).
 All Versions of this Article: M1917v1 13/1/40 most recent M1917v1 Submit a response Alert me when this article is cited Alert me when eLetters are posted Alert me if a correction is posted Services Similar articles in this journal Similar articles in PubMed Alert me to new issues of the journal Download to citation manager Citing Articles Citing Articles via HighWire Citing Articles via Google Scholar Google Scholar Articles by Shea, S. Search for Related Content PubMed PubMed Citation Articles by Shea, S. J Am Med Inform Assoc. 2006;13: DOI /jamia.M % to 7.42% in the subgroup with baseline HgbA1c 7% (n = 353)..")
43
Shea study on telemedicine For test patients with HgbA1c above 7% 0.93 reduction in HgbA1c (353 patients) 0.25 for control group (831 patients) Reduction in blood pressure and cholesterol levels seen as well
 0.25 for control group (831 patients) Reduction in blood pressure and cholesterol levels seen as well")
44
Remote Patient Monitoring One component gathering medical data One telecommunication component One evaluation component

45
Remote Patient Monitoring One component gathering medical data One telecommunication component One evaluation component

46
Next Steps

47
Remote Monitoring Clinical Data Center Secure Connection

48
Kuwait Health Reform (at least as far as chronic disease is concerned) 48 Recognize the financial and quality impact of poorly controlled chronic diseases. Collect and manage the data for these diseases. Invest in (or participate in existing) clinical data centers to provide real time management of chronic disease states in affected individuals. Invest in aggressive patient education and community outreach for disease management.
 clinical data centers to provide real time management of chronic disease states in affected individuals. Invest in aggressive patient education and community outreach for disease management..")
49
Repurposing the investment Data-intensive diseases Diabetes Hypertension Congestive Heart Failure Asthma Data-intensive situations Emergency Response Mass Casualty Renal Dialysis Infusion Centers Intensive Care Units Stroke Heart Attack 49

50
Communication Evidence based decisions Enhanced measurement Compliance Clinical Integration Members of a health care team working in concert to implement a plan of care.

51
Care Bundles ICU intensivist staffing is associated with a reduction of 40% in ICU mortality and 30% in overall hospital mortality. Clinical decision support systems reduce adverse drug reactions - 86% reduction in 4 years post-implementation. Use of “bundles” significantly improve clinical outcomes Raising the bar with bundles: Treating patients with an all-or-nothing standard. Joint Commission Perspectives on Patient Safety. 2006 Apr;6(4):5-6.
:5-6..")
54
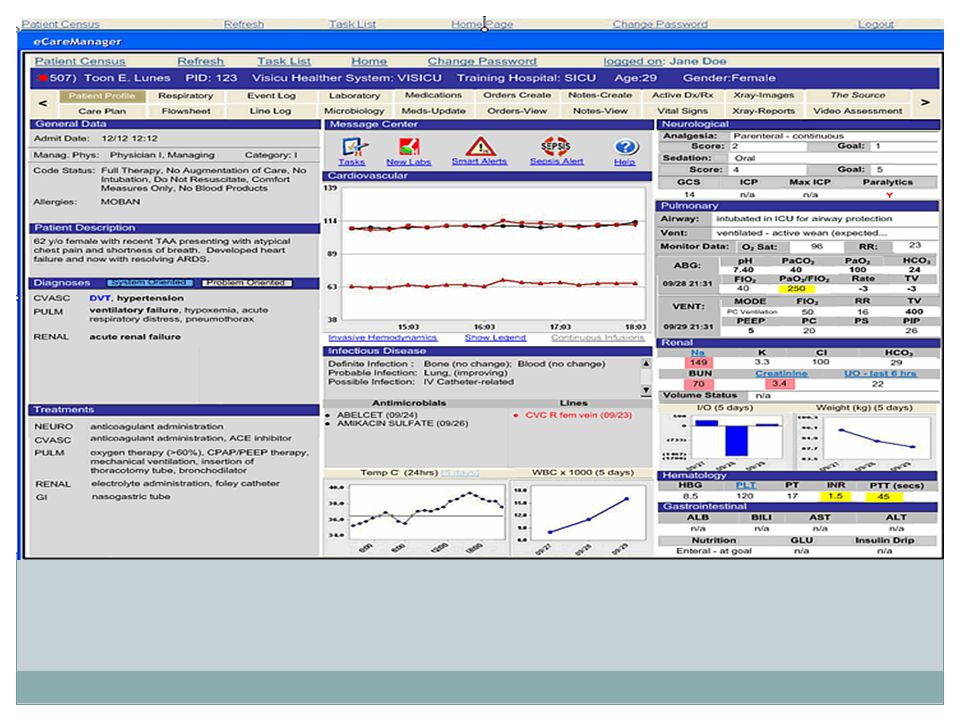
54 eICU Operational Solution

55
eICU ® Video Assessment Hospital Network eCareManager & The Source Real-Time Wave Forms PBX ‘Hot Phone’ Smart Alerts Video Assessment & Video Conference Bedside Monitor Camera Ceiling/Wall Mount Speaker Microphone ICU Patient Room Audio/Video Server

58
Healthcare Data Standards Many Applications with Different Message and Coding Standards Radiology Hospital Pharmacy Knowledge bases Physiologica l Monitors Medical Devices Bedside Computer Laboratorie s Admission Transfer Discharge (ADT) Billing Payers Communit y Pharmacie s Orders & Results Patient Medical Record Information (PMRI) Pharmacy Benefits Managers Clinical Content HL7 DICOM HL7 ASTM HL7 ASTM HL7 & proprietary HL7 & HL7 ASTM HL7 ASTM HL7 ASC X12N NCPDP ASC X12N NCPDP X12N NCPDP Protocols proprietary LOINC
 Billing Payers Communit y Pharmacie s Orders & Results Patient Medical Record Information (PMRI) Pharmacy Benefits Managers Clinical Content HL7 DICOM HL7 ASTM HL7 ASTM HL7 & proprietary HL7 & HL7 ASTM HL7 ASTM HL7 ASC X12N NCPDP ASC X12N NCPDP X12N NCPDP Protocols proprietary LOINC")
59
Where’s the EHR – Challenges with Information Sharing Hospitals Laboratory and Diagnostic Centers Ambulatory Care Clinics Physician OfficesLong Term Care Medical Suppliers Rehabilitation Centers Payer Organizations Pharmacies Home Health Care Electronic Health Record

60
Technical Architecture Data Center eICU ® Clinical Workstation HCA Workstation / eVantage Server Rack eCareManager Smart Alerts Interface Engine HA Database (2) Domain Controllers (2) HIS System ADT System Lab System PACS System MICU (10) GICU (10) Hospital Network Internet The Source ASP Hosted X-ray ScannerX- eCareManagerHIS/PACS CICU (10) SICU (14)
 Domain Controllers (2) HIS System ADT System Lab System PACS System MICU (10) GICU (10) Hospital Network Internet The Source ASP Hosted X-ray ScannerX- eCareManagerHIS/PACS CICU (10) SICU (14)")
61
ICU Bedside Monitor ‘A’ Network Hospital A HIS ‘A’ Interface Engine ‘A’ HL7 Interfaces Digitized Vital Signs ADT (IN) Lab Results (IN) Med Orders (IN) Flowsheet (IN) Notes (OUT) eCareManager Near Real-Time Vital Signs Hot Phone Smart Alerts Video Assessment & Video Conference eICU ® Audio/Video Switch Monitor ‘A’ Network Gateway Audio & Video Nurse Videoconference In-room Video Assessment Hospital B HIS ‘B’ Interface Engine ‘B’ Audio/Video Switch Monitor ‘B’ Network Gateway ICU Bedside Monitor ‘B’ Network HL7 Accelerator SQL Server Windows 2000 Rack Mounted Application & DB Servers ICU-to-eICU Interfaces eCareManager Smart Alerts HA Database Interface Server Near Real-Time Vitals (waveforms)
 Lab Results (IN) Med Orders (IN) Flowsheet (IN) Notes (OUT) eCareManager Near Real-Time Vital Signs Hot Phone Smart Alerts Video Assessment & Video Conference eICU ® Audio/Video Switch Monitor ‘A’ Network Gateway Audio & Video Nurse Videoconference In-room Video Assessment Hospital B HIS ‘B’ Interface Engine ‘B’ Audio/Video Switch Monitor ‘B’ Network Gateway ICU Bedside Monitor ‘B’ Network HL7 Accelerator SQL Server Windows 2000 Rack Mounted Application & DB Servers ICU-to-eICU Interfaces eCareManager Smart Alerts HA Database Interface Server Near Real-Time Vitals (waveforms)")
62
Sentara Healthcare: eICU ® Case Study 1 Critical Care Medicine 32:31-38;2004 (1) Severity Adjusted (27)% (17)% (13)% Baseline eICU
 Severity Adjusted (27)% (17)% (13)% Baseline eICU")
63
95% Goal Ventilator Bundle Compliance

69
Cost Analysis

70
6-Hospital System Outcomes 70 Severity – Adjusted Results N = 3800 patients * * * P< 0.001 P< 0.02 * P<0.001

71
Cost Reduction in U.S. eICUs 71 $100K in Routine Cost/bed/yr/day of stay $170K in Ancillary Cost/bed/yr/day of stay $5K per patient not admitted to ICU 30 Bed eICU with 70% occupancy = $4.5M cost reduction/year net of eICU cost, or $150K /bed/year

Similar presentations

























 is a digital version of a patient’s paper chart. EHRs are real-time, patient-centered.>")








