Download presentation
Presentation is loading. Please wait.

1
Introducing Liver Surgery to the MID NORTH COAST NSW Dr George Petrou FRACS 69Lake Rd, Port Macquarie NSW www.portlapsurgery.com.au Hepatobiliary Surgery, Laparoscopic Surgery, Obesity Surgery, Hernia surgery, Endosurgery

2
Indications for liver surgery Colorectal metastases Hepatocellular carcinoma Cholangiocarcinoma Neuroendocrine tumours Hepatic sarcomas Some benign lesions Select metastases- breast, gastric, pancreatic, melanoma

3
Colorectal Cancer 2 nd most common cancer in Australia 2 nd cancer killer 50% patients with colorectal cancer have or will develop liver metastases 15% patients have liver metastases at time of diagnoses of primary 120 colorectal cancer resections performed in Port Macquarie per year

4
Selecting patients for liver surgery Fit for major abdominal surgery. 30% normal functioning liver remnant. Size and number of tumours in the liver does not determine operability. Site of the tumour is more relevant. Patients eligible for surgery – 40-50%

5
Patient work up to determine operability Routine blood tests. Triple phase CT abdomen and CT chest. Liver directed MRI. CT PET used in selective cases (suspected extrahepatic disease or recurrent colorectal cancer). Multidisciplinary team discussion. Anaesthetic work up.
. Multidisciplinary team discussion. Anaesthetic work up..")
6
New Chemotherapy FOLFOX- median survival 24 months New agents are pushing this 2 year hurdle successfully FOLFIRI, FOLFOXFIRI +/- VEG inhibitors Now chemo alone med survival > 2 years 5 year hurdle is only a matter of time

7
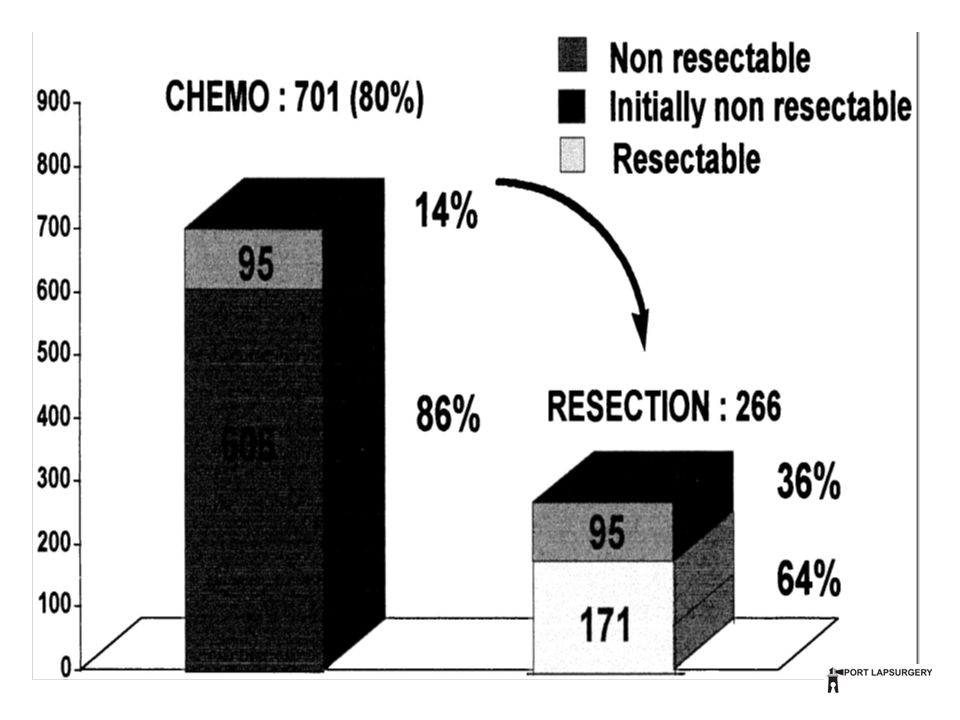
Neoadjuvant Chemotherapy Preoperative chemotherapy before liver surgery. Improves survival & increases operability.

9
Inoperable

10
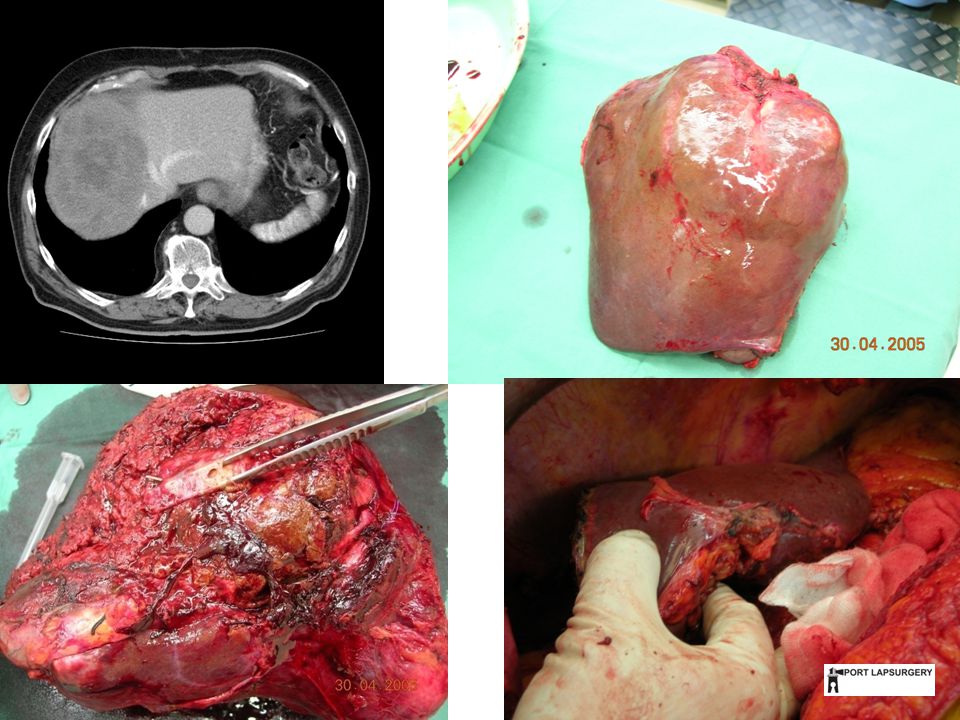
After Neoadjuvant chemotherapy this is now operable

11
RESECTION

12
Margins A clear margin is necessary to prevent local recurrence in the liver

14
Survival: marginal status Transection with CUSA (destroys 1cm) Inspect margin macroscopically R0 microscopically clear (>1mm) R1microscopically involved (<1mm) R2macroscopically involved (edge ablation)
 Inspect margin macroscopically R0 microscopically clear (>1mm) R1microscopically involved (<1mm) R2macroscopically involved (edge ablation)")
15
Survival: marginal status

16
Extrahepatic Disease Rule: excise when minimal

17
Pre-operative PET scan

18
Survival: Extrahepatic Disease

19
Synchronous Resection with bowel Rule: safe if minor liver resection is planned (2 or less liver segments to be removed)
")
20
Survival: Synchronous vs Metachronous

21
Number of lesions Rule: Doesn’t matter provided a clear margin and adequate remnant liver volume can be achieved.

22
Survival: No. of lesions

23
Portal Vein Embolisation Increases operability and safety with extended resection.

24
Small L Lateral Inoperable as not enough remnant liver left to make surgery safe

25
Right portal vein is radiologically embolised as a day procedure

26
The remnant liver grows after 4-6 weeks

27
RESECTION The tumour is now operable as surgery is now safe

28
Is it safe?

29
Literature Morbidity Morbidity 20-30% Bleeding 1-3% Bile leaks 10-30% Infection 10-30% Liver failure < 5% Wound problems 20% PE DVT 1-3%

30
Morbidity and Mortality Australia 30 day mortality 1-5% (3%) AUSTRALIA Only 3 centres have reported data 90% St George Hospital 10% Adelaide and Melbourne ANZHPBA consensus- centre should be doing 10 major resections per year
 AUSTRALIA Only 3 centres have reported data 90% St George Hospital 10% Adelaide and Melbourne ANZHPBA consensus- centre should be doing 10 major resections per year")
31
Local Expertise

32
Mid North Coast NSW Established GIT MDT (Cancer Care Centre) Easily accessible high definition CT and MRI PET- important for recurrent colon cancer Established interventional radiology with experience in percutaneous drain placement Theatre team with experience in major vascular and GIT surgery Anaesthetic and ICU experience in major vascular and GIT surgery Established GIT medical oncology
 Easily accessible high definition CT and MRI PET- important for recurrent colon cancer Established interventional radiology with experience in percutaneous drain placement Theatre team with experience in major vascular and GIT surgery Anaesthetic and ICU experience in major vascular and GIT surgery Established GIT medical oncology")
33
5 year results Port Macquarie NSW Surgeon- George Petrou FRACS

34
Feb 2008-Jan 2013 Total- 55 liver resections Benign 12 (21.8%) Malignant 43 (78.2%) 22 (40%) Major liver resection completed (more than 2 segments removed) 33 (60%) Minor liver resections completed (2 or less liver segments removed) Major liver resection and bile duct resection 2 Combined liver resection with bowel resection 4 Redo liver resection for colorectal cancer recurrence 3 Colorectal cancer metastases 27 Cholangiocarcinoma 4 HCC 4 Gallbladder cancer 1 SI cancer 1 Neuroendocrine tumour 1 30 day mortality 2 (3.6%)
 Malignant 43 (78.2%) 22 (40%) Major liver resection completed (more than 2 segments removed) 33 (60%) Minor liver resections completed (2 or less liver segments removed) Major liver resection and bile duct resection 2 Combined liver resection with bowel resection 4 Redo liver resection for colorectal cancer recurrence 3 Colorectal cancer metastases 27 Cholangiocarcinoma 4 HCC 4 Gallbladder cancer 1 SI cancer 1 Neuroendocrine tumour 1 30 day mortality 2 (3.6%)")
35
morbidity Suppurative infection 5 (9.1%) Wound dehiscence 2(3.6%) Incomplete tumour excision (0%) Pulmonary infection 2(3.6%) Pulmonary embolus 2(3.6%) Bile leak 4(7.3%) Anastomotic leak 1(1.8%) Liver failure 1(1.8%) Overwhelming sepsis 1(1.8%) Reoperation 2(3.6%)
 Wound dehiscence 2(3.6%) Incomplete tumour excision (0%) Pulmonary infection 2(3.6%) Pulmonary embolus 2(3.6%) Bile leak 4(7.3%) Anastomotic leak 1(1.8%) Liver failure 1(1.8%) Overwhelming sepsis 1(1.8%) Reoperation 2(3.6%)")
36
Laparoscopic US George Petrou FRACS The liver tumour is easily seen at operation with US

37
Summary Introducing Liver Surgery to a Regional Hospital Challenging but exciting time Enthusiastic and supportive colleagues Preliminary results encouraging Volume increasing Prometheus stole the secret of fire and gave it to man

Similar presentations










 MDT, University Hospital, Aintree,>")



 is well established Tomoharu T. et.>")


 in Colorectal Cancer Dr Chan Wai Keung Department of Surgery Ruttonjee and Tang Shiu Kin Hospitals.>")

