Download presentation
Presentation is loading. Please wait.

1
ARTERIAL DISEASES Objectives:
TO UNDERSTAND THE NATURE OF OCCLUSIVE ARTERIAL DISEASE AND ITS ASSOCIATED SYMPYOMS AND SIGNS TO ABLE TO ASSESS ACUTE AND CHRONIC ARTERIAL INSUFFICIENCY AND KNOW TREATMENT OPTIONS. TO KNOW ABOUT GANGRENE AND ITS MANAGEMENT TO KNOW OTHER ARTERIAL DISEASES LIKE ANEURYSMS, ARTERITIS AND VASOSPASTIC DISEASES & AVFistula

2
Arterial Occlusion

3
Occlusive arterial disease
Types Acute arterial occlusion Chronic arterial occlusion

4
ACUTE ARTERIAL OCCLUSION
CAUSES- EMBOLIC THROMBOTIC Heart diseases-Atrial fibrillation,mural thrombus, Post MI Rheumatic valvular heart diseases Paradoxical embolism- venous thromboembolism due to patent foramen ovale Arterio- arterial embolism- dislodgement of atheromatous plaques Angiographic procedures Accidental- intraarterial injection- Ergot,thiopental Trauma.

5
Embolism Brain-MCA Retina-Amaurosis fugax Mesenteric vessel- Spleen
Kidneys Lungs-pulmonary embolism

6
ACUTE ARTERIAL OCCLUSION-Embolism
C/F FIVE Ps PAIN PARALYSIS PALLOR PULSELESSNESS PARAESTHESIA

7
Relation ship of symptoms to the site of obstruction
Aorto-iliac obstruction Iliac obstruction Femoro-popliteal obstruction Distal obstruction ankle pulses absent Caludication in both buttocks,thighs & calves. Femoral & distal pulses absent in both limbs. Impotence.bruit over aortoiliac region. U/l claudication in thigh & calf buttocks. Bruits over iliac region U/L absence of femoral or distal pulses. U/L claudication in calf. Femoral pulse palpable with absent u/l distal pulses Femoral & Popliteal pulse palpable claudication in calf & foot

8
Arterial Stenosis General- Investigations: CBC,ESR,
PLASMA -fibrinogen, protein, electrophoresis, Glucose- blood n urine. Lipid profile Doppler -USG blood flow detection Duplex imaging. Echocardiography Arteriography DSA ECG

9
Hand held Doppler

10
COLOUR DUPLEX

11
ARTERIOGRAM

12
DSA

13
Angioscope

14
Treatment. Embolic arterial occlusion is an emergency!!!
THROMBOLYSIS – Immediate -Intra Venous Heparin 5000U to prevent distal and proximal extension of thrombus. Contraindications Recent stroke Active peptic ulcer Bleeding disorders Pregnancy Hydration EMBOLECTOMY THROMBECTOMY.

15
Fogarty catheterization- for removing proximal and distal extension of thrombus.
Postoperatively- heparin and oral anticoagulation Intrarterial Thrombolysis Only if ischemia is not so severe that immediate operation is mandatory, it is possible to treat thrombus or embolus by intra arterial thrombolysis Agents-TPA-tissue plasminogen activator** Streptokinase Urokinase Identify and treat the basic cause.

16
SFA thrombolectomy

17
Removed thrombus

18
Arterial Catheters

19
Chronic Arterial Insufficiency
Etiology Atherosclerosis Buerger’s disease Artritis Arterisclerosis Diabetes Risk Factors Hypertension Strong family history Smoking Lipid abnormalities

20
Chronic Limb Ischemia Ischemia of the lower limb may be minimal to critical Also called Chronic arterial insufficiency or Peripheral Vascular disease-PVD. Clinical presentation- Intermittant Claudication-commonest complaint. Fatigue, aching or crampy pain occuring with exertion and relieved by rest, reproducible at the same distance. Claudication distance- distance at which the pain appears Rest pain Critical ischemia- severe ischemia with actual or potential tisssue loss.

21
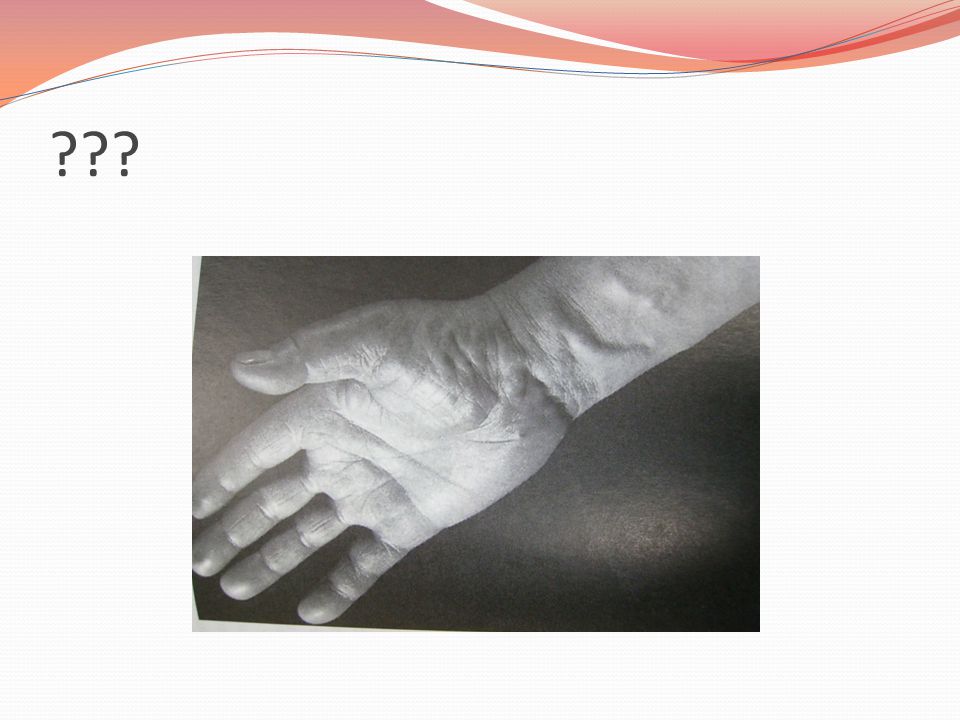
Signs of chronic ishemia
Loss of muscle mass/bulk Loss of subcutaneous fat Skin shiny Loss of hair Brittle nails Gangrene and ulcers of foot.

22
???

23
GANGRENE Def: death, often with putrifaction of macroscopic portion of tissues. VARIETIES ACCORDING TO THE CAUSE- Secondary: Thrombus in atherosclerotic artery. ATRIAL FIBRILLATION-embolus. Arteritis from NEUROPATHY BUERGERS DISEASE RAYNAUDS DISEASE/ERGOTISM- causing arterial shutdown INTRARTERIAL INJECTIONS- thiopentone & cytotoxic materials.

24
GANGRENE Primary: INFECTIVE- boils, carbuncles, gas gangrene, gangrene of scrotum (Fournier’s gangrene) TRAUMATIC- crush, pressure sores & constriction grooves PHYSICAL- burns, scalds,frostbite,chemical irradiation & electricity. VENOUS- C/F Pulseless,painnless,funtionless, with colour change. Lacks capillary refill and venous return. Black,brown, greenish black.

25
GANGRENE CLINICAL TYPES- DRY & MOIST DRY gangrene-
dessicated tissues,part becomes dry and wrinkled. Wrinkled ,discolourd from disintegration of Hb. & greasy to touch. MOISTgangrene: when venous & arterial obstruction is present, when artery is suddenly occluded by a ligature or embolus & in diabetes.. Infection & putrifaction is present. Part is swollen& discoloured. Crepitus may be present.

26
GANGRENE SEPERATION OF GANGRENE- SEPERATION BY DEMARCATION
SEPERATION WITHOUT DEMARCATION. Vague DEMARCATION & skip lesions. TREATMENT OF GANGRENE- GENERAL PRINCIPLES- limb saving attitude. Cardiac failure Atrial fibrillation anaemia. Nutritious diet. Control of diabetes. Analgesics. LOCAL TREATMENT- dry.protection of pressure areas. Cleanniess.

27
VARIETIES OF GANGRENE DIABETIC GANGRENE- three factors-
Trophic changes from peripheral neuritis. Atheroma of artries causing ischemia Excess sugar –decreases resistance to infections esp. fungal infection DIRACT TRAUMATIC GANGRENE BEDSORES-(Decubitus Ulcers) 5 factors Pressure Injury Anemia Malnutrition Moisture
 5 factors. Pressure. Injury. Anemia. Malnutrition. Moisture.")
28
Pressure Sore

29
Gangrene INDIRECT TRAUMATIC GANGRENE-
Interference with blood vessels from pressure by a fractured bones / strangulation Thrombosis of an artery Ligation of an artery poor technique for digital anesthesia ERGOT- claviceps purpurea. Fingers,nose & ears . Seen in migrane suffers.

30
PHYSICAL AND CHEMICAL CAUSE OF GANGRENE
. FROST BITE- cold+wind. Damage to Vessel wall with transudation & edema. Pain initially later painless & gangrene TRENCH FOOT-cold+ moist+ muscular inactivity. Ill fitting boots. I/V INJECTION OF THIOPENTONE DRUG ABUSE CHEMICAL GANGRENE- carbolic acid(phenol).
.")
31
Frost bite

32
ANEURYSMS ANEURYSMS- dilatation of a localised segment of the arterial system. True- all three layers involved. False- single layer of fibrinous tissue as the wall of the sac. According to the shape -fusiform -Saccular -Dissecting Eti0logy-traumatic/atherosclerotic/syphilitic/collagen disease(Marfan,syndrome), mycotic(bacterial)
, mycotic(bacterial)")
34
ANEURYSMS Symptoms- due to expansion, thrombosis, rupture or release of emboli. Symptom relate to the vessel affected, the site supplies or the tissue compressed. Clinical features Intrinsic-expansile pulsation along the course of an artery. proximal compression decreases pulsations Palpation- thrill Auscultation-bruits?? Extrinsic- neighboring or distal structures are affected. Nerve Veins Tubes-trachea ,esophagus

35
D/D Swelling under an artery- cervical rib(subclavian) Swelling over an artery-pancreatic cyst Pulsatile tumors-sarcoma,osteoclastoma & metastsis from hypernephroma. abscess serpentine artery- innominate,carotid.

36
ANEURYSMS Abdominal aortic aneurysm- Commonest large vessel aneurysm
2% population 95% atherosclerotic 95% below the renal arteries Symptomatic/asymptomatic Symptoms-back pain, sudden – mild-sudden severe.

37
ANEURYSMS Ruptured AAA- Anterior Posterior
Free bleeding into the peritoneal cavity(20%) Retroperitoneal hematoma(80%) Profound hypotension Severe pain
 Retroperitoneal hematoma(80%) Profound hypotension. Severe pain.")
38
ANEURYSMS Investigation: USG abdomen CT Chest & abdomen. AORTOGRAM

39
ANEURYSMS Procedure Open surgical procedure
Endoluminal stent graft procedure. Complications: Respiratory H’ge Colonic ischemia Renal failure Infection of the graft. Sexual dysfunction Fistula formation. Spinal cord ischemia.

40
Peripheral aneurysms Popliteal aneurysms- most common Femoral Iliac
Ascending aorta & arch

41
AVF: Communication between an artery & vein. Congenital Acquired-
trauma, penetrating wound or sharp blow, surgical for renal failure. Structural effect arterialized veins. Dilated tortuous veins Physiological effect- Increased VR, Increased VP, Increased HR- Increased CO. PP-HIGH LVF Cardiac failure Cong Fistula- Overgrowth of limb. Persistent ulcer due to distal ischemia.

42
???
43
AVF Clinical signs: Pulsatile swelling Thrill on palpation
Bruits on ausculatation Dilated veins Nicoladoni-Branham’s test- Decreased thrill, reduction in size and bradycardia on pressing the artery proximal to fistula Treatment Embolization Ligation of feeding artery??? Surgery- Separation of artery & vein

44
ARTERITIS Thromboangitis obliterans/ Buerger’s disease
Small & medium sized arteries.Occlusive disease Thrombophebitis of superficial/ deep veins. Raynauds syndrome, male, young patients

45
VASOSPASTIC CONDITIONS:
Reynaud's syndrome: Primary/ idiopathic form. Secondary Pallor- blanching Blue- cyanosis Redness-red engorgement. Accompanied by pain. Treatment - conservative Tab. nicotinamide Secondary Reynaud's syndrome- due to some other problem like-collagen disease, atherosclerosis, thoracic outlet syndrome, carpal tunnel syndrome

Similar presentations

















 Aneurysms Thrombangitis obliterans Inflammatory arteritis Aetiology.>")


 Embolism Trauma Crush injuries.>")