Download presentation
Presentation is loading. Please wait.

1
Prescription Overdose Deaths in Rural Virginia Martha J Wunsch MD FAAP FASAM Associate Professor, Virginia College of Osteopathic Medicine “Time to Team Up!” November 16, 2007 Virginia PMP & Virginia Board of Medicine

2
Learning Objectives Discuss the literature addressing rural prescription drug abuse Describe those decedents for whom prescription medications were a direct or contributing cause of death in Southwestern Virginia. Discuss Universal Precautions in the treatment of Pain

3
Literature Rural Rx Drug Abuse 1525 Felony Probationers 2001-2004 1 –Rural probationers were 5X more likely to have abused prescription opioids 233 Treatment Professionals Key Informants (RADARS) 2 –Geographic pockets of abuse of hydrocodone and oxycodone –Predominantly in very small urban, suburban, rural areas. 1 Havens et al. Am J Drug Alcohol Abuse. 2007;33(2):309-17 2 Cicero et al. Pharmacoepidemiol Drug Saf. 2007 Aug;16(8):827-40
: Cicero et al. Pharmacoepidemiol Drug Saf Aug;16(8):")
4
Literature Rural Rx Drug Abuse 233 Probationers and Prisoners SW Va 3 –Modified/Augmented ASI (2002-2004) –40% OxyContin Addiction Younger, less likely to be married More likely to be female More likely to abuse BZD, Methadone, cocaine, heroin. OxyContin Use Abuse and Diversion in SW Va 4 –50 OxyContin Addiction, 50 Prisoners, 34 Pain Patients : ASI, DSM IV, questionnaire –Demographics, Psychiatric Hx, Family not useful –SA history and POMI differentiated. 3. Wunsch et al. Journal of Addictive Disease. 26(4): 15-22. 4. Wunsch et al., under review Journal of Opioid Management.
: Wunsch et al., under review Journal of Opioid Management..")
5
* Opioids as a direct or contributing cause of death YearDrug Deaths Opioid Related Deaths* OxycodoneMethadoneFentanylHydrocodoneMSO4 199767?140612 19986983 6 0127 199984251812 0811 20001013619 22 11017 20011649541 4993413 Medical Examiner Cases SW Va

6
Drug and Rx Opioid Deaths 0 50 100 150 200 250 300 19981999200020012002200320042005 Year Number of Deaths Drug Deaths Opioid Deaths

7
Overall Goal* “The overall goal of this study is to characterize Medical Examiner cases where prescription medications are identified as a direct or contributing case of death in a rural area of Virginia” National Institute of Drug Abuse *National Institute of Drug Abuse RO3 DA019047-01A1

8
Methods: In depth review of Medical Examiner Files 1997-2003 Autopsy Results Death Certificates Death Scene Investigations Police Reports Toxicology Reports Physician Notes Hospital Records ( ER, Inpatient, Psych)
")
9
Data from Western District

10
Prevalence of Drug-related Fatalities Western VAU.S. Male23.3 per 100K12.9 per 100K Female11.8 per 100K7.0 per 100K 893 drug-related deaths (1997-2003) in Western Virginia 686 (76.8%) involved opioids
 in Western Virginia 686 (76.8%) involved opioids.")
11
Demographics of Opioid Deaths N=686 (1997-2003) Gender – 64.9% Male ; 35.1% Female Median Age of sample –39.7 years Males 38.6 years Females 41.4 years Race –95.9% White ; 3.9% African American ; 0.4% Native American; 0.1% Asian
 Gender – 64.9% Male ; 35.1% Female Median Age of sample –39.7 years Males 38.6 years Females 41.4 years Race –95.9% White ; 3.9% African American ; 0.4% Native American; 0.1% Asian")
12
Employment Employment Status –Working 48.1% –Disabled 25.4% –Unemployed 12.9% –Unknown 12.1% –Retired 1.5% Occupation –Homemaker 11.5% –Construction 10.2% –Mining Labor 4.2% –Mfg Labor 7.4% –Other Labor 9.0%

13
Marital Status OverallMaleFemale Ever Married70.6%63.1%83.5% Single25.5%31.9%13.9% p<.01

14
Opioid Deaths Of total 893 deaths, opioids were a direct or contributing cause of death in 686. Prevalent opioids listed as a cause of death: Methadone249 Hydrocodone160 Oxycodone160 Fentanyl45 Heroin19 >1 Opioid (Polydrug) (present on toxicology) 252
 (present on toxicology) 252.")
15
Opioid Mortality: Manner of Death OverallMaleFemale Accident78.9 %84.3%69.2% Suicide18.1%12.8%27.9% Other0.8%0.9%0.8% Unknown2.0% 2.1% p<.001

16
Other Drugs Present (Identified on Toxicology) Tobacco*29.3% Cocaine12.1% Alcohol27.4% Cocaethylene2.0% Methamphetamine0.4% Any Anti-depressant44.6% Any Benzodiazepine45.9% *from History
 Tobacco*29.3% Cocaine12.1% Alcohol27.4% Cocaethylene2.0% Methamphetamine0.4% Any Anti-depressant44.6% Any Benzodiazepine45.9% *from History")
17
Age & Gender Distribution MaleFemale Under 35169 38.0% 52 21.6% 35 or Older276 62.0% 189 78.4% Deaths among older people predominate (consistent with other studies of Rx drug deaths) Most pronounced among women
 Most pronounced among women")
18
Prescription Drug Mortality CDC Injury Study 1990-2001 (11 states) 4 –Poisonings increased average of 145% nationwide. –Highest rates among 35-54 year olds New Dawn 2003 (6 states) 5 –Multiple drugs involved in opioid related deaths –Highest death rates were 35-54 year olds in 5 of 6 states. 4 MMWR Weekly. 2004;53(11):233-238. 4 SAMHSA DAWN Report: Opiate-Related Drug Misuse Death in Six States: 2003 5 Substance Abuse and Mental Health Services Administration. The New DAWN Report: Opiate-Related Drug Misuse Death in Six States: 2003; 2006, Issue 19.
 5 –Multiple drugs involved in opioid related deaths –Highest death rates were year olds in 5 of 6 states. 4 MMWR Weekly. 2004;53(11): SAMHSA DAWN Report: Opiate-Related Drug Misuse Death in Six States: Substance Abuse and Mental Health Services Administration. The New DAWN Report: Opiate-Related Drug Misuse Death in Six States: 2003; 2006, Issue 19..")
19
Opioid Prescriptions and Pain Decedents Holding Opioid Prescription MaleFemale Under 3531.1%34.0% 35 or Older43.5%54.5% Decedents with History of Chronic Pain MaleFemale Under 3524.5%23.4% 35 or Older38.4%49.7%

20
Depression and Anxiety Decedents with History of Depression MaleFemale Under 3526.5%44.7% 35 or Older39.5%52.9% Decedents with History of Anxiety MaleFemale Under 3515.2%10.6% 35 or Older15.6%25.4%

21
Prescriptions for Related Drugs Decedents with Prescription for Anti-depressant MaleFemale Under 3519.2%25.5% 35 or Older26.1%47.6% Decedents with Prescription for Benzodiazepine MaleFemale Under 3525.2%36.2% 35 or Older35.1%50.3%

22
Disturbing Pattern Of female decedents with Rx for Opioid: –68.6% hold Rx for Benzodiazepine –61.2% hold Rx for Anti-depressant Of male decedents with Rx for Opioid: –59.1% hold Rx for Benzodiazepine –39.8% hold Rx for Anti-depressant Female decedents over 35 exhibit particularly high rates of co-morbidity of chronic pain, depression, and anxiety and hold prescriptions for multiple drugs including opioids, benzodiazepines, and anti-depressants

23
What about the cases where Methadone was identified on toxicology? The most commonly identified opioid in our cases

24
Methadone Mortality Demographics Gender – 75.2% Male ; 24.8% Female Race –98% White ; 1.2% African American;.4 % Asian 45 % of decedents were prescribed an opioid –53% of these decedents were prescribed methadone

25
Age Distribution of Cases

26
Co-Morbidity: Methadone Cases Chronic Pain 40% –55 % have an antidepressant on toxicology –55 % have a benzodiazepine on toxicology Anxiety Disorder 19% –50% have an antidepressant on toxicology –46% have a benzodiazepine on toxicology Depression 40% –60% have an antidepressant on toxicology –56% have a benzodiazepine on toxicology

27
Toxicology Results Opioids –68% had only methadone present –24% had methadone AND another opioid present –8% had methadone AND 2 or more opioids present

28
Source of Methadone in 2004 Medical Examiner Drug Deaths Melissa Weimer DO Martha Wunsch MD

29
Goal of the Project Describe methadone deaths in western Virginia from January 1, 2004 to December 31, 2004. Ascertain the probable source of methadone. Compare decedents for which methadone was –Prescribed in an opiate treatment programs –Prescribed for the treatment of pain –Procured illicitly.

30
“Subjects” Retrospective, population-based investigation of all medical examiner cases January 1, 2004- December 31, 2004. Subjects: –Accessed OCME computer database of deaths and autopsies in 2004 where poisoning was the fatal agency. –Identified cases where methadone detected in the serum toxicology. –Selected cases were methadone was noted to be a direct or contributing cause of death.

31
Cases Definition Total Drug Deaths 2004 –204 Identified –68 cases (33.5%) Methadone was identified as a direct or contributing cause of death AND toxicology was positive 7 excluded because they lived outside the PMP Pilot Study area (source unavailable) –61 Cases for study
 Methadone was identified as a direct or contributing cause of death AND toxicology was positive 7 excluded because they lived outside the PMP Pilot Study area (source unavailable) –61 Cases for study")
32
Procedures Review of case files and entry into existing database* –Autopsy Results –Death Certificates –Death Scene Investigations –Police Reports –Toxicology Reports –Physician Notes –Hospital Records ( ER, Inpatient, Psych) National Institute of Drug Abuse *National Institute of Drug Abuse RO3 DA019047-01A1
 National Institute of Drug Abuse *National Institute of Drug Abuse RO3 DA A1")
33
Demographic Characteristics 95% Caucasian 64% male 49% metropolitan residence 44% rural residence Age: Range 19-59; mean 35.8 years old

34
Case Characteristics History of Drug Abuse 54% –Intravenous Drug Use (autopsy) –Evidence death scene (drugs, syringes, straws) –Medical/Psychiatric History Addiction treatment Overdose requiring hospitalization Cocaine, cannabis, opioid abuse Cause of Death –Methadone sole agent 34%; Polydrug abuse 66%
 –Evidence death scene (drugs, syringes, straws) –Medical/Psychiatric History Addiction treatment Overdose requiring hospitalization Cocaine, cannabis, opioid abuse Cause of Death –Methadone sole agent 34%; Polydrug abuse 66%")
35
Procedure Using the Virginia Prescription Monitoring Program identify decedents who were prescribed methadone for the treatment of pain* –Prescription misuse >1 physician Rx obtained simultaneously. >1pharmacies used to fill Rx simultaneously. >1 Rx filled in one month. *Methadone can only be prescribed in a private office for the treatment of pain (Harrison Act, 1914)
.")
36
Procedure Identify decedents ever enrolled in an opioid treatment program –Medical Examiners and Substance Abuse treatment programs may communicate in death investigations without permission of next of kin (42 CFR Part 8) –Contacted program directors to identify cases By exclusion, decedents identified as obtaining methadone illicitly
 –Contacted program directors to identify cases By exclusion, decedents identified as obtaining methadone illicitly")
37
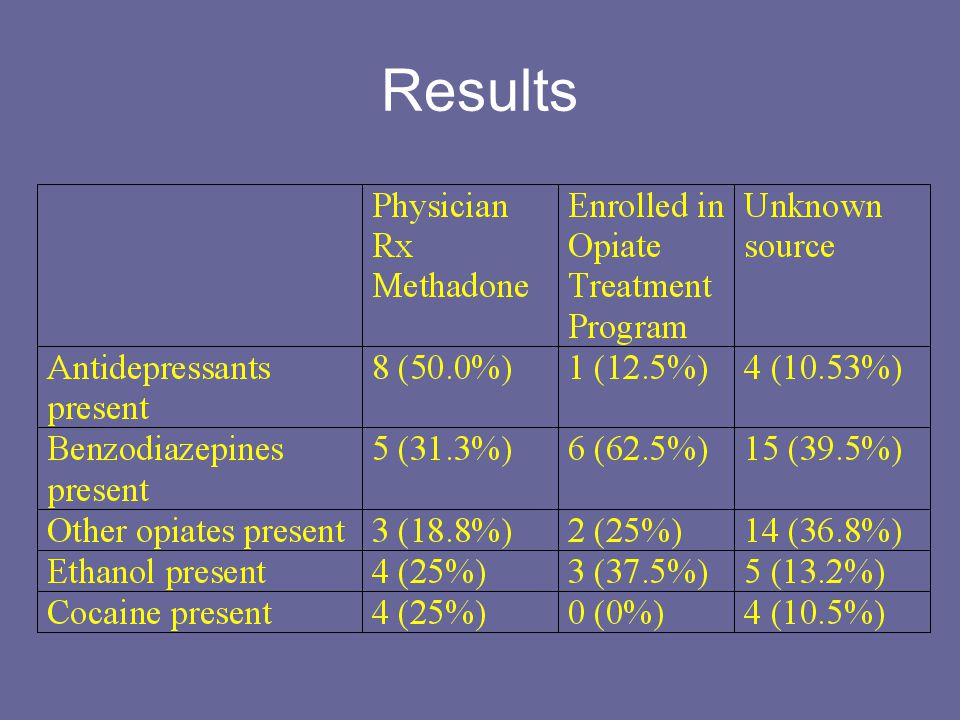
Results

42
Conclusions Minority of the cases were individuals who were enrolled in “methadone clinics” Majority of cases involved overdose with multiple substances Differences in those who were prescribed methadone for: –The treatment of pain –The treatment of opioid addiction Methadone: PK, metabolism, lethality

43
Treating Pain in midst of an “epidemic” of Prescription Drug Abuse Suggested Reading: Gourlay DL, Heit HA, Almahrezi A. Universal precautions in pain medicine: a rational approach to the treatment of chronic pain. Pain Medicine. 2005;6(2):107-12.
:")
44
Universal Precautions 1. Make a Diagnosis with Appropriate Differential 2. Conduct a Psychological Assessment Including Risk of Addictive Disorders 3. Informed Consent 4. Treatment Agreement 5. Pre- and Post-Intervention Assessment of Pain Level and Function

45
Universal Precautions 6. Appropriate Trial of Opioid Therapy +/– Adjunctive Medication 7. Reassessment of Pain Score and Level of Function at each visit 8. Regularly Assess the “Four A’s” of Pain Medicine 9. Periodically Review Pain Diagnosis and Comorbid Conditions, Including Addictive Disorders 10. Documentation: careful and complete recording of the initial evaluation and at each follow up is both medically and legally indicated and in the best interest of all parties.

46
Literature Havens JR, Oser CB, Leukefeld CG, Webster JM, Martin SS, O'Connell DJ, Surratt HL, Inciardi JA. Differences in prevalence of prescription opiate misuse among rural and urban probationers. Am J Drug Alcohol Abuse. 2007;33(2):309-17. Cicero TJ, Surratt H, Inciardi JA, Munoz A. Relationship between therapeutic use and abuse of opioid analgesics in rural, suburban, and urban locations in the United States. Pharmacoepidemiol Drug Saf. 2007 Aug;16(8):827-40.
: Cicero TJ, Surratt H, Inciardi JA, Munoz A. Relationship between therapeutic use and abuse of opioid analgesics in rural, suburban, and urban locations in the United States. Pharmacoepidemiol Drug Saf Aug;16(8):")
47
Literature Cited Paulozzi LJ, Budnitz DS, Xi Y. Increasing deaths from opioid analgesics in the United States. Pharmacoepidemiol Drug Saf. 2006 Sep;15(9):618- 27 Centers for Disease Control and Prevention. Unintentional and undetermined poisoning deaths- 11 states, 1990-2001. MMWR Weekly. 2004;53(11):233-238. Substance Abuse and Mental Health Services Administration. The New DAWN Report: Opiate-Related Drug Misuse Death in Six States: 2003; 2006, Issue 19.
: Centers for Disease Control and Prevention. Unintentional and undetermined poisoning deaths- 11 states, MMWR Weekly. 2004;53(11): Substance Abuse and Mental Health Services Administration. The New DAWN Report: Opiate-Related Drug Misuse Death in Six States: 2003; 2006, Issue 19..")
48
Literature Cited Wunsch MJ, Nakamoto K, Goswami A, Schnoll SH. Prescription Drug Abuse among Prisoners in Rural Southwestern Virginia. Journal of Addictive Disease. 26(4): 15-22. Wunsch MJ, Cropsey KL, Campbell E, Knisely JC. OxyContin® Use, Abuse, and Diversion in Three Populations in Southwestern Virginia. Under review Journal of Opioid Managment
: Wunsch MJ, Cropsey KL, Campbell E, Knisely JC. OxyContin® Use, Abuse, and Diversion in Three Populations in Southwestern Virginia. Under review Journal of Opioid Managment.")
Similar presentations






 patients Policy.>")















