Download presentation
Presentation is loading. Please wait.

1
e-Preference: A Tool for Incorporating Patient Preferences into Health Decision Aids Amar K. Das, MD, PhD Assistant Professor Departments of Medicine (Medical Informatics) and Psychiatry and Behavioral Sciences Stanford University Amar K. Das, MD, PhD Assistant Professor Departments of Medicine (Medical Informatics) and Psychiatry and Behavioral Sciences Stanford University
 and Psychiatry and Behavioral Sciences Stanford University Amar K. Das, MD, PhD Assistant Professor Departments of Medicine (Medical Informatics) and Psychiatry and Behavioral Sciences Stanford University.")
2
Outline Health decision aids Clinical example e-Preference approach Prototype system and evaluation Health decision aids Clinical example e-Preference approach Prototype system and evaluation

3
Health Decisions in Aging Older individuals often face complex health decisions involving significant risk of morbidity and/or mortality Patient participation is desirable in such decisions Clinicians’ ability to facilitate shared decision making varies Older individuals often face complex health decisions involving significant risk of morbidity and/or mortality Patient participation is desirable in such decisions Clinicians’ ability to facilitate shared decision making varies

4
Health Decision Aids Focus typically on Improvements in patient knowledge Explanation of treatment alternatives Communication of risk Focus typically on Improvements in patient knowledge Explanation of treatment alternatives Communication of risk

5
HDA Presentation Non-interactive formats Brochure (paper booklet or Web based) Audiotape Video Interactive formats Decision board Computer Multimedia Non-interactive formats Brochure (paper booklet or Web based) Audiotape Video Interactive formats Decision board Computer Multimedia
 Audiotape Video Interactive formats Decision board Computer Multimedia Non-interactive formats Brochure (paper booklet or Web based) Audiotape Video Interactive formats Decision board Computer Multimedia")
6
Outline Health decision aids Clinical example e-Preference approach Prototype system and evaluation Health decision aids Clinical example e-Preference approach Prototype system and evaluation

7
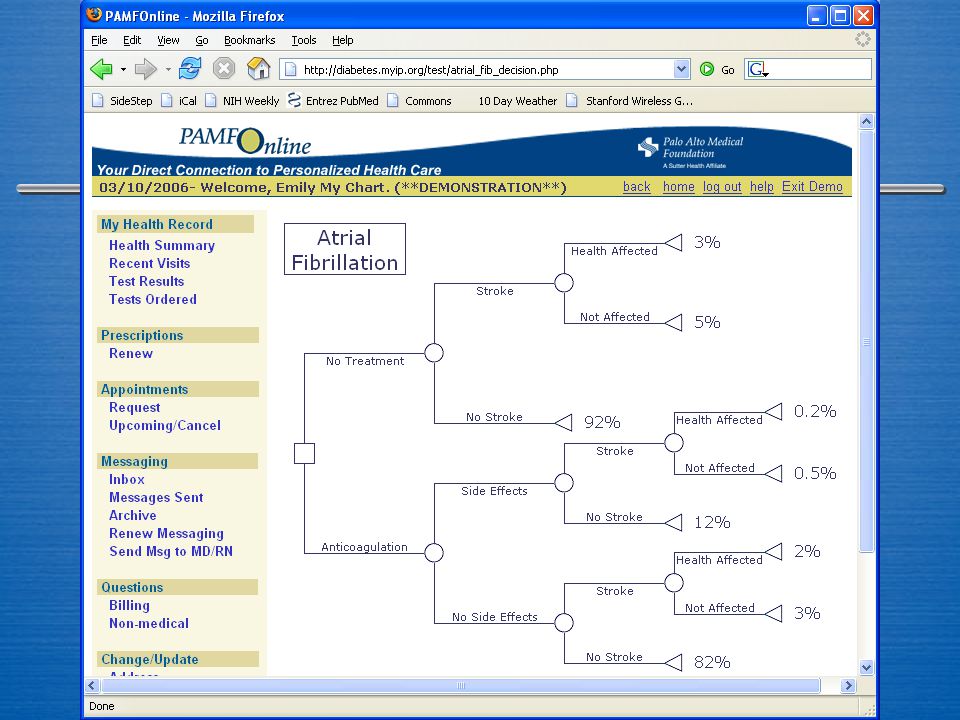
Atrial Fibrillation Atrial fibrillation leads to a significant risk of stroke, ranging from 1% to 15% per year, based on patient factors Anticoagulation therapy (warfarin) can reduce the risk of stroke by approximately two thirds, but incurs a risk of major bleeding complications of 1% to 3% per year Atrial fibrillation leads to a significant risk of stroke, ranging from 1% to 15% per year, based on patient factors Anticoagulation therapy (warfarin) can reduce the risk of stroke by approximately two thirds, but incurs a risk of major bleeding complications of 1% to 3% per year
 can reduce the risk of stroke by approximately two thirds, but incurs a risk of major bleeding complications of 1% to 3% per year Atrial fibrillation leads to a significant risk of stroke, ranging from 1% to 15% per year, based on patient factors Anticoagulation therapy (warfarin) can reduce the risk of stroke by approximately two thirds, but incurs a risk of major bleeding complications of 1% to 3% per year")
8
Measuring Preferences Eight studies that modeled treatment preferences of patients with atrial fibrillation Studies used three methods Probability tradeoff technique Decision aid Decision analysis Eight studies that modeled treatment preferences of patients with atrial fibrillation Studies used three methods Probability tradeoff technique Decision aid Decision analysis (Man-Son-Hing et al., 2005)
")
9
Audiobooklet (Man-Son-Hing et al., 2000)
")
10
Audiobooklet (Man-Son-Hing et al., 2000)
")
11
Audiobooklet (Man-Son-Hing et al., 2000)
")
12
Decision Analysis (Protheroe et al., 2000)
")
13
Decision Analysis Guideline Decision Analysis Total TreatDo not treat Treat 482270 Do not treat 111627 593897 17 on treatment 28 on treatment (Protheroe et al., 2000)
")
14
Decision-Support Tool (Thomson et al., 2002)
")
15
Decision-Support Tool (Thomson et al., 2002)
")
16
HDA Limitations Typically designed for one type of health decision May not provide patient-specific information on alternatives and risks May be only accessible in particular settings Does not have readily modifiable design Typically designed for one type of health decision May not provide patient-specific information on alternatives and risks May be only accessible in particular settings Does not have readily modifiable design

17
Design Desiderata for HDAs We need a design that can Be tailored to specific health problems Incorporate patient-specific data Be accessible via the Internet Be easily modified We need a design that can Be tailored to specific health problems Incorporate patient-specific data Be accessible via the Internet Be easily modified

18
Outline Health decision aids Clinical example e-Preference approach Prototype system and evaluation Health decision aids Clinical example e-Preference approach Prototype system and evaluation

19
Motivation for e-Preference Create an environment for clinical experts and software developers to design and implement HDAs Based on our research group’s long standing interest in developing customizable and reusable software architectures for decision support Create an environment for clinical experts and software developers to design and implement HDAs Based on our research group’s long standing interest in developing customizable and reusable software architectures for decision support

20
EON Architecture Protocol KB Patient Database Patient Database Problem-Solving Method Problem-Solving Method Query Engine Query Engine End-User Application End-User Application Protégé

21
Design of e-Preference A set of software methods for Knowledge representation Decision-analytic computation Data access from existing database Web-based multimedia presentation A set of software methods for Knowledge representation Decision-analytic computation Data access from existing database Web-based multimedia presentation

22
e-Preference Architecture KBDM Patient Database Patient Database Query Engine Query Engine HDA Protégé FLAIR Netica

23
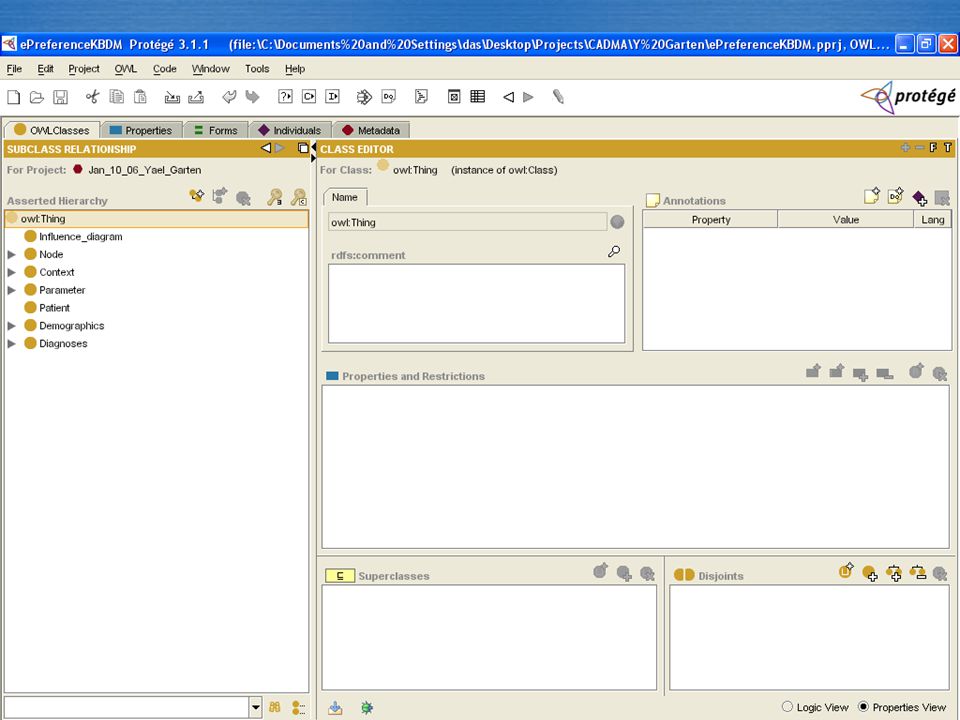
Knowledge-Based Decision Model Encode concepts related to Influence diagrams Health decisions and outcomes Risk factors Patient preferences Relationships between these factors Encode concepts related to Influence diagrams Health decisions and outcomes Risk factors Patient preferences Relationships between these factors

24
Netica

25
FLAIR

26
Supreme genus: SUBSTANCE Subordinate genera: BODYSPIRIT Differentiae: material immaterial Differentiae: animate inanimate Differentiae: sensitive insensitive Subordinate genera: LIVING MINERAL Proximate genera: ANIMALPLANT Species: HUMANBEAST Differentiae: rational irrational Individuals: Socrates Plato Aristotle … Aristotle’s Categories

28
The NCI Thesaurus

29
Structuring Knowledge

30
Web Ontology Language A Semantic Web standard to use ontologies to represent knowledge on the Internet OWL can be used to build ontologies of high- level descriptions, based on three concepts: Classes (e.g., Influence Diagram, Nodes, Patient) Properties (e.g., has_node, has_disease) Individuals (e.g., “atrial fibrilaton”) A Semantic Web standard to use ontologies to represent knowledge on the Internet OWL can be used to build ontologies of high- level descriptions, based on three concepts: Classes (e.g., Influence Diagram, Nodes, Patient) Properties (e.g., has_node, has_disease) Individuals (e.g., “atrial fibrilaton”)
 Properties (e.g., has_node, has_disease) Individuals (e.g., atrial fibrilaton ) A Semantic Web standard to use ontologies to represent knowledge on the Internet OWL can be used to build ontologies of high- level descriptions, based on three concepts: Classes (e.g., Influence Diagram, Nodes, Patient) Properties (e.g., has_node, has_disease) Individuals (e.g., atrial fibrilaton )")
31
Diagnoses OWL Example Patient Nodes Influence Diagrams AF E. MyChart has_model Decision DMAF Chance Outcome has_diagnosis has_chance_node

32
Semantic Web Rule Language A language for expressing logical rules in terms of OWL concepts Rules in SWRL can be used to deduce new knowledge about an existing OWL ontology A language for expressing logical rules in terms of OWL concepts Rules in SWRL can be used to deduce new knowledge about an existing OWL ontology Patient(?pt) ^ has_dx(?pt, ?dx) ^ has_model(dx, ?hda) activate_HDA(?pt, ?hda)
 ^ has_dx( pt, dx) ^ has_model(dx, hda) activate_HDA( pt, hda)")
34
Making Restrictions

37
Generating a Decision Model

38
Remaining Challenges Modeling and editing probabilities in Protégé OWL Generating interface based on modified influence diagram Modeling and editing probabilities in Protégé OWL Generating interface based on modified influence diagram

39
KBDM Approach Advantages Ability to modify knowledgebase and create tailored decision model for HDA Disadvantages Efforts needed for acquiring and maintaining knowledge Advantages Ability to modify knowledgebase and create tailored decision model for HDA Disadvantages Efforts needed for acquiring and maintaining knowledge

40
Outline Health decision aids Clinical example e-Preference approach Prototype system and evaluation Health decision aids Clinical example e-Preference approach Prototype system and evaluation

51
Conclusions HDAs can help to incorporate patient preferences into shared decision making The knowledge used in developing HDAs using decision analyses can be encoded Such knowledge can be used to generate and tailor HDAs HDAs can help to incorporate patient preferences into shared decision making The knowledge used in developing HDAs using decision analyses can be encoded Such knowledge can be used to generate and tailor HDAs

52
Acknowledgments Stanford Medical Informatics Bilal AhmedDaniel Rubin Yael Garten Ravi Shankar Jeremy Robin Samson Tu Center for Primary Care and Outcomes Research Mary GoldsteinTamara Sims Doug Owens NIA and CADMA for funding support Stanford Medical Informatics Bilal AhmedDaniel Rubin Yael Garten Ravi Shankar Jeremy Robin Samson Tu Center for Primary Care and Outcomes Research Mary GoldsteinTamara Sims Doug Owens NIA and CADMA for funding support

Similar presentations

















. Knowledge-based systems Knowledge based systems are artificial intelligent tools working in a narrow domain to.>")








 Norman Piedade de Noronha 16 th July, 2004.>")



