Download presentation
Presentation is loading. Please wait.

1
Rabih R. Azar, MD, MSc, FACC Director of Cardiovascular Research Hotel Dieu de France Hospital Associate Professor of Medicine Saint Joseph University School of Medicine Beirut, Lebanon NSTEMI: GPIIB/IIIA Inhibitors & Emerging Antiplatelets: Where Do We Stand?

2
Role of the Platelets in Thrombosis UA/NQMI: Partially-occlusive thrombus (primarily platelets) Intra-plaque thrombus (platelet dominated) Plaque core ST MI: occlusive thrombus (platelets, red blood cells, and fibrin) Intra-plaque thrombus (platelet dominated) Plaque core SUDDEN DEATH Adapted from Davies MJ. Circulation. 1990; 82 (supl II): 30-46.
:")
3
GP IIb/IIIa Receptor Activation Pathway ASPIRIN ASPIRIN HEPARINS ASPIRIN ASPIRIN ASPIRIN ASPIRIN GP IIb/IIIa Thickness of line indicates strength of activator 5HT PAF Epi Thrombin ADP TXA 2 ASPIRIN Vasopressin Collagen Fibrinogen PLATELET PLATELET CLOPIDOGREL

4
Platelet-fibrinogen interaction

5
5 Time after bolus (minutes) 15304560120 0 60 80 100 abciximab plus infusion tirofiban 10 µg/kg bolus plus infusion 85% Inhibition of Light Transmission Aggregation Induced by 20 µM ADP After Treatment with Tirofiban or Abciximab Inhibition of Maximal Aggregation (%) TARGET DOSE
 abciximab plus infusion tirofiban 10 µg/kg bolus plus infusion 85% Inhibition of Light Transmission Aggregation Induced by 20 µM ADP After Treatment with Tirofiban or Abciximab Inhibition of Maximal Aggregation (%) TARGET DOSE")
6
6 Time after bolus (minutes) 15304560120 0 60 80 100 abciximab plus infusion tirofiban 10 µg/kg bolus plus infusion tirofiban 20 µg/kg bolus plus infusion tirofiban 25 µg/kg bolus plus infusion 85% Inhibition of Light Transmission Aggregation Induced by 20 µM ADP After Treatment with Tirofiban or Abciximab Inhibition of Maximal Aggregation (%) TARGET DOSE SHBD
 abciximab plus infusion tirofiban 10 µg/kg bolus plus infusion tirofiban 20 µg/kg bolus plus infusion tirofiban 25 µg/kg bolus plus infusion 85% Inhibition of Light Transmission Aggregation Induced by 20 µM ADP After Treatment with Tirofiban or Abciximab Inhibition of Maximal Aggregation (%) TARGET DOSE SHBD")
7
EPIC: 3-year Outcome JAMA 1997;278:478

8
8 PRISM-PLUS: Study Design Endpoints Primary: Composite death, MI, refractory ischemia, rehospitalization at 7 days Secondary: Death, MI, refractory ischemia, rehospitalization at 48 h, 30 days, and 6 months Safety: Major bleeding (>4.0 g/dL decrease in Hb, blood transfusion >2 U, need for corrective surgery, or intracranial or retroperitoneal hemorrhage, or any combo) Endpoints Primary: Composite death, MI, refractory ischemia, rehospitalization at 7 days Secondary: Death, MI, refractory ischemia, rehospitalization at 48 h, 30 days, and 6 months Safety: Major bleeding (>4.0 g/dL decrease in Hb, blood transfusion >2 U, need for corrective surgery, or intracranial or retroperitoneal hemorrhage, or any combo) AGGRASTAT 0.4 g/kg/min for 30 min, then 0.10 g/kg/min maintenance + heparin (n=773) AGGRASTAT 0.4 g/kg/min for 30 min, then 0.10 g/kg/min maintenance + heparin (n=773) Heparin 5000 U loading, then 1000 U maintenance (n=797) Heparin 5000 U loading, then 1000 U maintenance (n=797) Randomization UA or NSTEMI patients Chest pain within 12 h and ECG abnormalities or elevated CK-MB UA or NSTEMI patients Chest pain within 12 h and ECG abnormalities or elevated CK-MB 48 h PRISM-PLUS Study Investigators. N Engl J Med. 1998;338(21):1488-1497.
:")
9
PRISM PLUS: Results NEJM 1998;338:1488

12
Brenner et al. Circulation 1998;98:734 RAPPORT: Abciximab in primary PTCA reduces death/MI/urgent TVR at 30 days

13
Synergy between abciximab and stenting in primary angioplasty for acute MI. Event free suvival (death, acute coronary syndromes, TVR) Azar et al. J Am Coll Cardiol 1998;32:1996
 Azar et al. J Am Coll Cardiol 1998;32:1996.")
14
GP IIb/IIIa Receptor Activation Pathway ASPIRIN ASPIRIN HEPARINS ASPIRIN ASPIRIN ASPIRIN ASPIRIN GP IIb/IIIa Thickness of line indicates strength of activator 5HT PAF Epi Thrombin ADP TXA 2 ASPIRIN Vasopressin Collagen Fibrinogen PLATELET PLATELET CLOPIDOGREL

17
Does Clopidogrel Eliminate the Need for GPIIb/IIIa Antogonists?

18
Treatment with AGGRASTAT™ provides greater flexibility for early surgical procedures, transfer, or discharge Adapted from Kereiakes DJ et al. Am Coll Cardiol 1996;27(3):536-542 0.5 60 100 % inhibition Fast-On Approximate % platelet aggregation blocked Fast-Off Return to baseline of platelet function Hours of infusionHours postinfusion 80 40 20 122448 0 60 100 80 40 20 248 0 End infusion 3567 % inhibition Slide 14
: % inhibition Fast-On Approximate % platelet aggregation blocked Fast-Off Return to baseline of platelet function Hours of infusionHours postinfusion End infusion 3567 % inhibition Slide 14.")
21
EPISTENT: Effect of Thienopyridine Pretreatment Placebo No Pretreat Placebo Pretreat Abcix No Pretreat Abcix Pretreat 42% (P=0.028 ) 33% (P=0.033 ) Steinhubl S et al. Circulation 2001;103:1403-9

28
28

29
29 Tirofiban vs Placebo 00 22 44 66 Death 30 Days Death Death 5 Months Death 3.03.0 2.02.0 OR= 0.66 P<0.0001 OR= 0.66 P<0.0001 3.53.5 2.72.7 OR= 0.81 P=0.02 OR= 0.81 P=0.02 Placebo Tirofiban Meta-analysis of 22 RCTs including 12,874 pts 8-10 Deaths per 1000 pts NNT: 100 NNT: 125 Valgimigli M et al Eur Heart J. 2010; 31:35-49

30
30 Tirofiban vs Placebo 00 55 1010 1515 Death 30 Days Death Death/MI Death/MI 2.72.7 1.41.4 OR= 0.50 P=0.005 OR= 0.50 P=0.005 12.212.2 8.58.5 OR= 0.61 P<0.0001 OR= 0.61 P<0.0001 Placebo Tirofiban Meta-analysis of 14 RCTs including 3,424 pts 62 D/MI per 1000 pts NNT: 77 NNT: 16 On top of pre-treatment with Clopidogrel Valgimigli M et al Eur Heart J. 2010; 31:35-49

31
Enough Data to Support the Use of GPIIb/IIIa Antagonists during High-Risk PCI GPIIb/IIIa antagonists:GPIIb/IIIa antagonists: –Should be given for patients with high risk ACS undergoing PCI irrespective of the use of clopidogrel –Question is timing: upstream (as early as possible on admission) or downstream (in the cath lab at the time of PCI)
 or downstream (in the cath lab at the time of PCI)")
32
UpStream vs. Downstream GPIIb/IIIa Inhibitors ACUITY Timing trial 9207 patients with ACS9207 patients with ACS Upstream vs. downstream use of GPIIb/IIIaUpstream vs. downstream use of GPIIb/IIIa Upstream: 98% received GPIIb/IIIa; mean duration 18.3 hUpstream: 98% received GPIIb/IIIa; mean duration 18.3 h Downstream: 56% received GPIIb/IIIa; mean duration 13.1 hDownstream: 56% received GPIIb/IIIa; mean duration 13.1 h Use of thienopyridines: 64% before angiography or PCIUse of thienopyridines: 64% before angiography or PCI

33
UpStream vs. Downstream GPIIb/IIIa Inhibitors ACUITY Timing trial P = 0.009 P = NS Stone et al. JAMA 2007;297:591-602

42
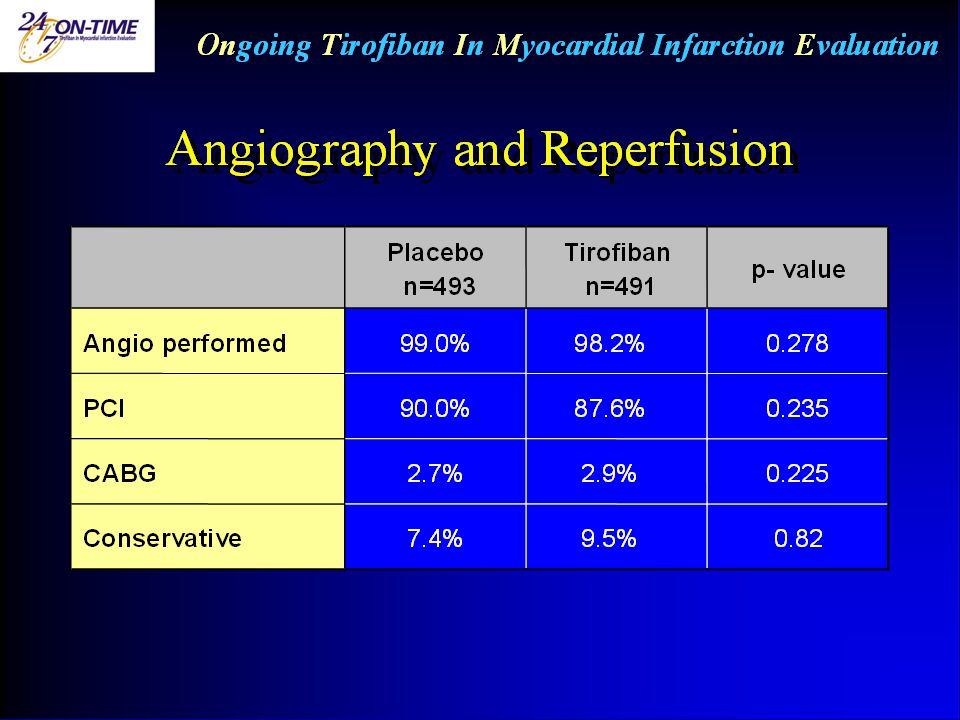
Ongoing Tirofiban In Myocardial Infarction Evaluation All-Cause Mortality 30 Days open label & double-blind, n = 1398

43
Ongoing Tirofiban In Myocardial Infarction Evaluation All-Cause Mortality 1-Year P = 0.077 open label & double-blind, n = 1398

44
Ongoing Tirofiban In Myocardial Infarction Evaluation 1 Year Survival: Patients with Primary PCI P = 0.007 open label & double-blind, n = 1.155

45
EARLY-ACS trial 9492 patients with non-ST elevation MI9492 patients with non-ST elevation MI All assigned to an invasive strategyAll assigned to an invasive strategy Randomized to:Randomized to: –Early eptifibatide –Early placebo with provisional use of eptifibatide in the cath lab (38% received eptifibatide in the cath lab) Primary end-point: death or MI or recurrent ischemia requiring urgent revascularization or thrombotic bailoutPrimary end-point: death or MI or recurrent ischemia requiring urgent revascularization or thrombotic bailout 5559 underwent PCI5559 underwent PCI
 Primary end-point: death or MI or recurrent ischemia requiring urgent revascularization or thrombotic bailoutPrimary end-point: death or MI or recurrent ischemia requiring urgent revascularization or thrombotic bailout 5559 underwent PCI5559 underwent PCI")
46
EARLY-ACS trial: Results P = ns P = 0.015 Guigliano RP et al. N Engl J Med 2009;360:2176-2190

47
But We Have New Oral Anti-platelet Agents that are MORE POTENT than Clopidogrel

48
What is the role of GPIIb/IIIa antagonists when those agents are used?

50
Patients included in TRITON were “clopidogrel and prasugrel naives”. Patients included in TRITON were “clopidogrel and prasugrel naives”. There was no PRE-TREATMENT with either of the 2 drug. There was no PRE-TREATMENT with either of the 2 drug. Clopidogrel or prasugrel were given on the cath table, immediately prior or during PCI Clopidogrel or prasugrel were given on the cath table, immediately prior or during PCI

54
Eff-SK-2-MENA-07/10

58
Did the use of GPIIb/IIIa inhibitor affect the outcome? No data

59
PCI=Percutaneous Coronary Intervention; CABG=Coronary Artery Bypass Graft surgery TRITON-TIMI 38: Index Procedure Clopidogrel (n=6,795) % Prasugrel (n=6,813) % PCI99 CABG11 Any Stent9594 Bare-Metal Stent4748 Drug-Eluting Stent47 Multivessel PCI14 Anticoagulant Therapy Unfractionated heparin6566 Low Molecular Weight Heparin89 Bivalirudin33 GP IIb/IIIa- receptor antagonist5554 Wiviott SD et al. New Engl J Med 2007;357:2001-2015

60
O‘Donoghue et al. JACC 2009 No GP IIb/IIIa inhibitor + GP IIb/IIIa inhibitor CV death, MI, stroke

64
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLAT elet Inhibition and patient O utcomes trial Outcomes in patients with STEMI and planned PCI The PLATO trial was funded by AstraZeneca STEMI Ph.Gabriel Steg*, Stefan James, Robert A Harrington, Diego Ardissino, Richard C. Becker, Christopher P. Cannon, Håkan Emanuelsson, Ariel Finkelstein, Steen Husted, Hugo Katus, Jan Kilhamn, Sylvia Olofsson, Robert F. Storey, Douglas Weaver, Lars Wallentin, for the PLATO study group *Unité INSERM U-698 Hôpital Bichat – Claude Bernard Université Paris VII – Denis Diderot

65
STEMI Patient disposition 18,758 patients enrolled in PLATO 134 patients not randomized 18,624 patients randomized NSTEMI/UA/other: 10,194 patients STEMI: 8,430 patients Randomized to ticagrelor: efficacy population N= 4,201 Randomized to clopidogrel: efficacy population N= 4,229 No intake of study medication: 36 patients No intake of study medication: 48 patients Safety population N=4,165 Safety population N=4,181

66
STEMI Primary endpoint: CV death, MI or stroke 0123456789101112 12 11 10 9 8 7 6 5 4 3 2 1 0 Months HR: 0.85 (95% CI = 0.74–0.97), p=0.02 No. at risk Clopidogrel Ticagrelor 4,229 4,201 3,892 3,887 3,823 3,834 3,7303,022 3,011 2,333 2,297 1,868 1,8913,732 11.0 9.3 Clopidogrel Ticagrelor K-M estimated rate (% per year)
.")
67
Proposed Algorithm for Initial Management of NSTEMI ST depression or + troponin ? -- clopidogrel (class I) or ticagrelor(class I) and early cath lab. If PCI: Tirofiban in cath lab (class I). If CABG: WAIT 5 DAYS OR -Tirofiban (class I ACC/ Iia ESC) and early cath lab. If PCI prasugrel (class I) (or clopidogrel) on the table. If CABG, do it same or next day Aspirin + Hep or Enoxaparin NO Conservative therapy: No indication for GPIIb/IIIa antagonists YES
 or ticagrelor(class I) and early cath lab. If PCI: Tirofiban in cath lab (class I). If CABG: WAIT 5 DAYS OR -Tirofiban (class I ACC/ Iia ESC) and early cath lab. If PCI prasugrel (class I) (or clopidogrel) on the table. If CABG, do it same or next day Aspirin + Hep or Enoxaparin NO Conservative therapy: No indication for GPIIb/IIIa antagonists YES.")
68
Proposed Algorithm for Initial Management of STEMI Possibility of Primary PCI? NO Yes Aspirin + clopidogrel or prasugrel or ticagrelor * (class I) IIb/IIa antagonist - pre cath: IIb - During PCI: IIa Fibrinolysis
 IIb/IIa antagonist - pre cath: IIb - During PCI: IIa Fibrinolysis.")
69
ESC Guidelines for GPIIb/IIIa Inhibitors in NSTEMI RecommendationClassLevel of evidence Among patients on DAPT, if PCI is high risk (+trop; visible thrombus), add GPIIb/IIIa IB If high-risk patient not treated with P2Y12 inhibitor, add GPIIb/IIIa prior to angiography IIaC If high-risk patient treated with DAPT, add GPIIb/IIIa prior to PCI if on going ischemia and low bleeding risk IIbC GPIIb/IIIa routinely prior to angiographyIIIIA GPIIb/IIIa in patients on DAPT treated conservatively IIIIA
, add GPIIb/IIIa IB If high-risk patient not treated with P2Y12 inhibitor, add GPIIb/IIIa prior to angiography IIaC If high-risk patient treated with DAPT, add GPIIb/IIIa prior to PCI if on going ischemia and low bleeding risk IIbC GPIIb/IIIa routinely prior to angiographyIIIIA GPIIb/IIIa in patients on DAPT treated conservatively IIIIA")
70
ACC/AHA Guidelines for GPIIb/IIIa Inhibitors in NSTEMI RecommendationClassLevel of evidence Medium or high-risk patients clopidogrel or (upstream) GPIIb/IIIa in addition to ASA prior to PCI IA Medium or high-risk patients: GPIIb/IIIa at the time of PCI (downstream) IA Upstream GPIIb/IIIa in high-risk patients already on DAPT who are selected for an invasive approach and who are not at high risk of bleeding IIbB Low risk ischemia patients or patients at high risk of bleeding and who are receiving DAPT IIIB
 GPIIb/IIIa in addition to ASA prior to PCI IA Medium or high-risk patients: GPIIb/IIIa at the time of PCI (downstream) IA Upstream GPIIb/IIIa in high-risk patients already on DAPT who are selected for an invasive approach and who are not at high risk of bleeding IIbB Low risk ischemia patients or patients at high risk of bleeding and who are receiving DAPT IIIB")
75
Treatment with AGGRASTAT™ provides greater flexibility for early surgical procedures, transfer, or discharge Adapted from Kereiakes DJ et al. Am Coll Cardiol 1996;27(3):536-542 0.5 60 100 % inhibition Fast-On Approximate % platelet aggregation blocked Fast-Off Return to baseline of platelet function Hours of infusionHours postinfusion 80 40 20 122448 0 60 100 80 40 20 248 0 End infusion 3567 % inhibition Slide 14
: % inhibition Fast-On Approximate % platelet aggregation blocked Fast-Off Return to baseline of platelet function Hours of infusionHours postinfusion End infusion 3567 % inhibition Slide 14.")
76
Keys Points in Anti-Platelet Therapy in NSTEMI 1.During PCI: GPIIb/IIIa antogonists are class I indication in both ESC and ACC/AHA guidelines on top of aspirin and thienopyridines 2.Dual anti-platelet therapy as early as possible in high-risk patients (asa + clopidogrel or ticagrelor; class I) or (asa + GPIIb/IIIa class I in ACC and class IIa in ESC) I favor GPIIb/IIIa antagonists rather than thienopyridines because safer if surgery (allows surgery sooner) 3.Routine triple anti-platelet therapy in high-risk patients prior to PCI is class IIb indication in the ACC/AHA guidelines and class III indication in ESC guidelines (but it becomes class IIb if recurrent ischemia) 4.GPIIb/IIIa antagonists are not recommended for low risk patients
 or (asa + GPIIb/IIIa class I in ACC and class IIa in ESC) I favor GPIIb/IIIa antagonists rather than thienopyridines because safer if surgery (allows surgery sooner) 3.Routine triple anti-platelet therapy in high-risk patients prior to PCI is class IIb indication in the ACC/AHA guidelines and class III indication in ESC guidelines (but it becomes class IIb if recurrent ischemia) 4.GPIIb/IIIa antagonists are not recommended for low risk patients")
Similar presentations






























 Time AdmissionCathDischarge No Cath Cath PCI Surgery Medical Rx (no cath) Medical Rx No disease (82 % of total) (18 % of total) (52%>")





>")











 and Clopidogrel (Plavix™) Benedict R. Lucchesi, M.D., Ph.D. Department of Pharmacology University of Michigan Medical School.>")
 Prospective Randomized Double Blind.>")