Download presentation
Presentation is loading. Please wait.

2
Femtosecond-assisted Astigmatic Keratotomy
MOHAMMAD RABEI, H. MD. IMAM HOSSEIN MEDICAL CENTER SHAHID BEHESHTI UNIVERSITY The speaker have no financial interest on this presentation

3
Introduction Naturally occurring and postsurgical astigmatism cause reduced uncorrected visual acuity (UCVA), Corneal astigmatism between 0.25 and 1.25D occurs in up to 64% and >1.5 D in 22%of patients undergoing cataract surgery. The average magnitude of astigmatism after PK, is D

4
Introduction 8% to 20% of PK patients requiring surgical intervention.
Mild degrees of astigmatism may be manage with: Spectacles Soft toric CL RGP

5
Introduction Higher degrees of astigmatism may require surgical management. In phakic patients, Toric IOL. Other Relaxing incisions, wedge resection or compression sutures in PK Lasik PRK

6
Relaxing incisions Relaxing incision is one of the most commonly performed procedures for astigmatic reduction as it can correct high levels of astigmatism with fast visual recovery. Incisions can be: Limbal, Arcuate, Transverse Free hand or with a mechanical keratome. Arcuate keratotomy remains the most popular procedure as it has better predictability.

7
Relaxing incisions Complications include: Microperforation,
Wound gape, Infection, Epithelial inclusion Femtosecond laser technology has been used to perform astigmatic keratotomy with promising results. Femtosecond laser-assisted incisions (FSL-assisted AK)have the advantage of no skip lesions, minimized risk of perforation, and increased precision in terms of incision depth, length, angulation, and centration.
have the advantage of no skip lesions, minimized risk of perforation, and increased precision in terms of incision depth, length, angulation, and centration.")
8
Femtosecond Astigmatic keratotomy
Femtosecond laser systems: IntraLase FS (Advanced Medical Optics, Santa Ana, CA), Technolas Perfect Vision 520 FS (Technolas Perfect Vision, Munich, Germany), VisuMax Femtosecond System (Carl Zeiss Meditec, Jena, Germany), Femto LDV (Ziemer Group, Port, Switzerland). The IntraLase and Femto LDV systems are enabled with software for astigmatic keratotomy in the United States,
, Technolas Perfect Vision 520 FS (Technolas Perfect Vision, Munich, Germany), VisuMax Femtosecond System (Carl Zeiss Meditec, Jena, Germany), Femto LDV (Ziemer Group, Port, Switzerland). The IntraLase and Femto LDV systems are enabled with software for astigmatic keratotomy in the United States,")
9
On the IntraLase FS 30 kHz system, incision depth is restricted to a maximum of 400 mm,
The 60 and 150 kHz systems include a keratoplasty mode with greater incision depth flexibility. treatment parameters:

10
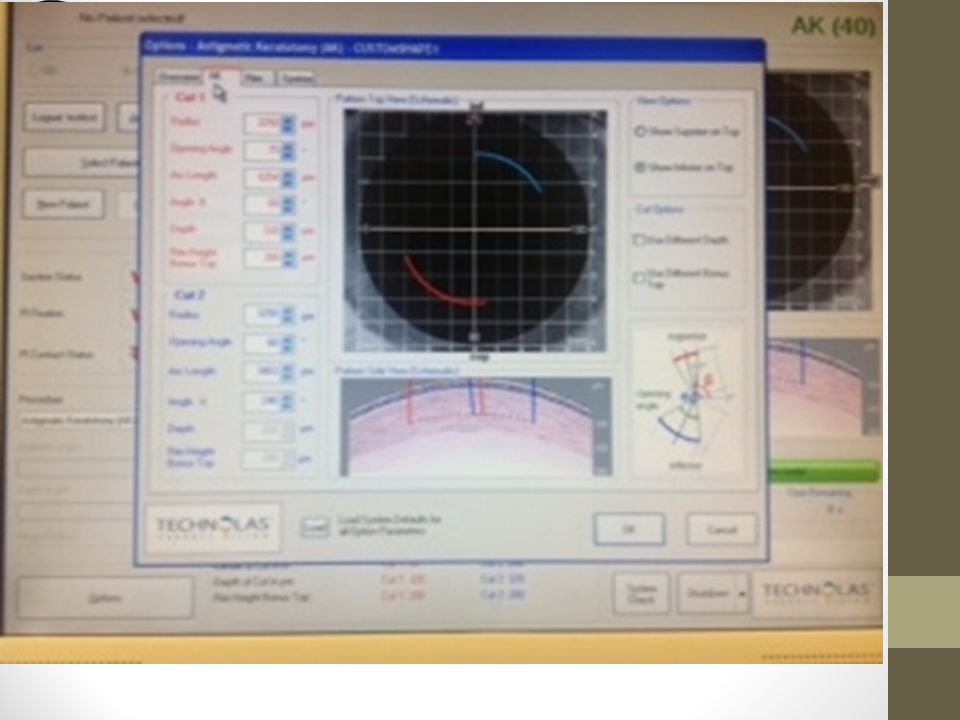
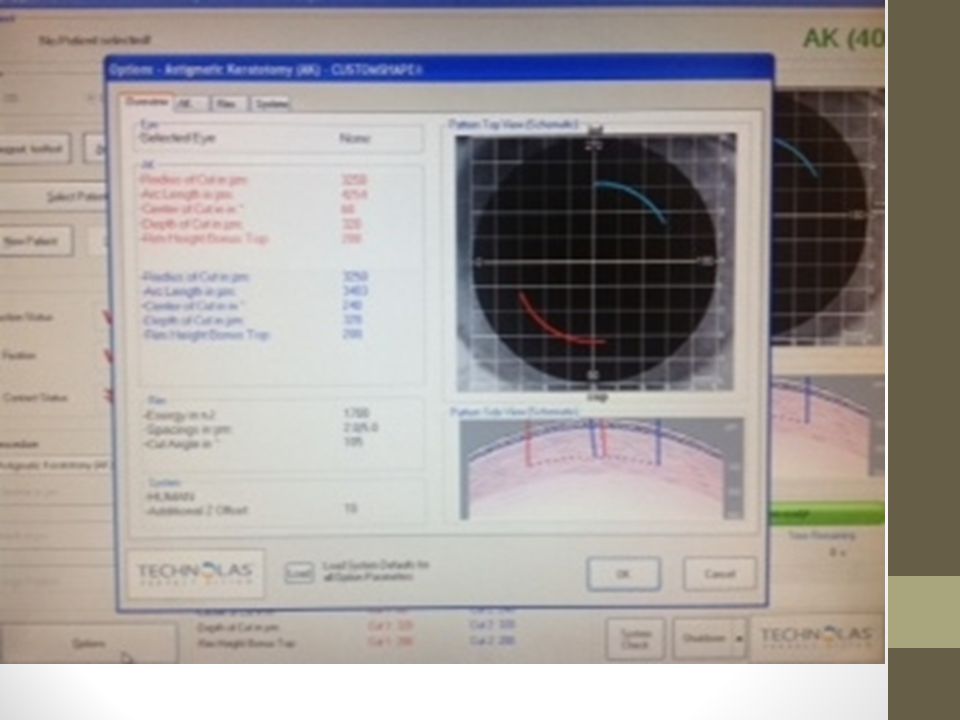
The energy settings, Horizontal overlap, Layer separation, Spot separation, Depth in glass values The side cut angle (angle of incision to surface of cornea) have been set at 75 or 90 degrees The parameters that are individualized to the patient are posterior depth in micron (intended depth of incision or percent depth of corneal thickness at incision site), diameter in mm (optical zone diameter), cut position (axis where center of incision is to be placed), and cut angle (angular length of incision in degrees).
 have been set at 75 or 90 degrees. The parameters that are individualized to the patient are posterior depth in micron (intended depth of incision or percent depth of corneal thickness at incision site), diameter in mm (optical zone diameter), cut position (axis where center of incision is to be placed), and cut angle (angular length of incision in degrees).")
11
Surgical Technique Mark the limbus with gentian violet at the slit lamp. Prepped and anesthetized topically similar Mark the zone diameter Mark the planned locations of incisions Corneal thickness measurment AC-OCT can be used in the preoperative surgical planning

12
Surgical Technique Treatment parameters are entered,
The suction ring followed by the applanation cone Centering on the pupil. The treatment screen shows the locations of the incisions and the suction ring can be used to rotate the eye to ensure proper axis alignment. Release of the suction ring and applanation cone, the incisions are immediately opened with a Sinskey hook. Postoperative care includes use of topical antibiotics until epithelization is achieved and topical steroids for several weeks.

20
Overlay of the femtosecond arcuate, phaco, and sideport incisions.
Optical coherence tomography of the cornea in the area of the arcuate incision confirms its depth.

21
LASER SETTINGS (30-KHZ) IN FEMTOSECOND-ASSISTED ANTERIOR KERATOTOMY
Posterior depth : 420 μm Anterior sidecut diameter : 6.0 mm Anterior sidecut energy : 2.3 mJ Anterior sidecut 1 position : 3° Anterior sidecut 1 angle : 80° Anterior sidecut 2 position : 183° Anterior sidecut 2 angle : 80° Anterior sidecut angle : 80° Anterior sidecut spot separation : 5 μm Anterior sidecut layer separation : 5 μm Depth in contact glass : 50 μm

22
Articles The FS laser has been used to perform AK with promising results. In a German study, Kiraly et al described the use of the FS laser to perform arcuate incisions in 10 postkeratoplasty patients. BCVA improved in 8 patients. The average corneal astigmatism was reduced by 3 D and average refractive astigmatism by 4 D.

23
Articles Harissi-Dagher and Azar were the first in the US to report their results of femtosecond for postkeratoplasty astigmatism in 2 patients. BCVA improved from 20/100 to 20/30 and from 20/200 to 20/60 and astigmatism reduced by 3.6 D (from 8.5 to 4.9 D) and 2.7 D (from 7.0 to 4.3 D).
 and 2.7 D (from 7.0 to 4.3 D).")
24
Articles Kymionis et al similarly reported a beneficial result in their patient with postkeratoplasty irregular astigmatism and showed improvement of BCVA from 20/50 to 20/32 and reduction of manifest cylinder from 4.0 to 0.5 D.

25
Articles Nubile et al treated 12 postkeratoplasty eyes (including 2 eyes with DALK) with incision depth of 90% and arc length of 40 to 80 degrees within 1mm of graft-host junction. Mean logarithm of the minimum angle of resolution (logMAR) of BCVA improved from 0.25±0.16 to 0.11±0.12 at 6 months and UCVA improved from 1.05±0.18 to 0.55±0.34. Mean astigmatism reduced from 7.16±3.07 to 2.23±1.55 diopters at 1 month.
 with incision depth of 90% and arc length of 40 to 80 degrees within 1mm of graft-host junction. Mean logarithm of the minimum angle of resolution (logMAR) of BCVA improved from 0.25±0.16 to 0.11±0.12 at 6 months and UCVA improved from 1.05±0.18 to 0.55±0.34. Mean astigmatism reduced from 7.16±3.07 to 2.23±1.55 diopters at 1 month.")
26
Articles In a large series of 37 eyes with >5 D of regular astigmatism after keratoplasty with at least 6 months follow-up, Kumar et al showed improvement of UCVA (logMAR 1.08±0.34 to 0.80±0.42), BCVA (logMAR 0.45±0.27 to 0.37±0.27), reduction of absolute cylindrical power (7.46±2.70 to 4.77±3.29), and reduction of astigmatism vector (2.52×122 degrees±5.4 to 0.41×126±4.0 degrees).
, BCVA (logMAR 0.45±0.27 to 0.37±0.27), reduction of absolute cylindrical power (7.46±2.70 to 4.77±3.29), and reduction of astigmatism vector (2.52×122 degrees±5.4 to 0.41×126±4.0 degrees).")
27
Articles In a retrospective analysis, Bahar et al described results of 20 eyes that underwent manual AK using a diamond blade and 20 eyes that underwent FS keratotomy. Both groups had improvement of UCVA and BCVA, however, only the FS group achieved a statistical significant improvement. Compared with the manual technique, use of FS showed a trend toward greater FS-assisted AK improvement of visual acuity and defocus equivalent (which correlates better with UCVA than spherical equivalent) and greater reduction of absolute cylinder. Although manual keratotomy resulted in shift of astigmatism axis, FS brought the mean astigmatic vector closer to neutral.
 and greater reduction of absolute cylinder. Although manual keratotomy resulted in shift of astigmatism axis, FS brought the mean astigmatic vector closer to neutral.")
28
Articles In the only randomized study to date, Hoffart et al compared mechanized AK with FS astigmatic keratotomy. Twenty eyes were randomized to either mechanized treatment using the Hanna keratotome or FS using the Femtec FSL with incision depth set at 75% depth and other treatment parameters based on the Hanna nomogram. The FS group had a higher reduction of cylinder power ( – 55.4±20.7%, from mean preoperative refractive cylinder of 8.6±3.0 to 3.9±2.4 D) compared with mechanized group ( – 29.7±30.0%, from 6.7±2.1 to 4.7±2.4 D). Both mechanized and laser groups suffer from undercorrection, however, there was a tendency toward greater axis misalignment with the keratotome. One microperforation and 1 off-center incision were noted in the keratotome group.
 compared with mechanized group ( – 29.7±30.0%, from 6.7±2.1 to 4.7±2.4 D). Both mechanized and laser groups suffer from undercorrection, however, there was a tendency toward greater axis misalignment with the keratotome. One microperforation and 1 off-center incision were noted in the keratotome group.")
29
Articles Abbey et al reported their results in a patient with naturally occurring astigmatism of 5.25 D in both eyes. Treatment parameter was based on the modified Lindstrom nomogram for naturally occurring astigmatism and guided by topographic cylinder axis. Significant improvement of UCVA (counting fingers to 20/50, 20/200 to 20/30) and reduction of manifest cylinder power (2.5 D, 3.0 D) were seen at 1 year.
 and reduction of manifest cylinder power (2.5 D, 3.0 D) were seen at 1 year.")
30
Complications In Kumar et al series of 37 eyes, 8% of eyes experienced rejection, all of which resolved with topical steroids. Overcorrection occurred initially in 24% of eyes, which required resuturing of the astigmatic keratotomy incisions. After adjusting the treatment parameters in the subsequent eyes, overcorrection decreased to 11%. Two thirds of the eyes that experienced overcorrection were keratoconic, suggesting the ecstatic eyes may be at increased risk of overcorrection.

31
In Nubile et al series of 12 eyes with incision depth of 90%, 2 microperforations occurred while the incision was opened with a blunt spatula after creation with the femtosecond laser. However, it is the authors’ belief that the perforations were a result of mechanical stress on the thin deep stromal bed under the incision exerted by the spatula rather than the occurrence of primary full-thickness femtosecond laser cut.

32
Conclusions High levels of astigmatism, either naturally occurring or more commonly post surgical, may require surgical interventions, of which AK remains the mainstay of treatment. Compared with traditional techniques of AK, FS assisted AK has shown to be efficacious and safe with greater precision and predictability. Larger studies to formulate nomograms specific for FS AK are needed. Future developments in FS laser technology may allow creation of subepithelial stromal incisions with potential for greater safety.

33
Conclusion Lens material and design is essential for long-term quality of vision Predicting future sometimes difficult The lens we use today, although very efficient, will be antics in a few months! Thank you

35
Thank you

Similar presentations











 Dr Rajesh Fogla DNB, FRCS, MMed Senior Consultant,>")














