Download presentation
Presentation is loading. Please wait.

1
Preparing for an Unplanned Radiation Event

2
Radiation Terrorism and Response
OUTLINE Radiation Terrorism and Response Radiation Basics Radiation Protection Rules Radiation Threats Nuclear device, “dirty” bomb Equivalent Experiences: Chernobyl, Goiana 4. Health Management of Affected Population

3
What is Radiation? For the purpose of this presentation, defined as energetic emissions from unstable atoms that can result in ionizing events to target atoms Ionizing radiation is radiation capable of imparting its energy to the body and causing chemical changes Ionizing radiation is emitted by - Radioactive material Some devices such as x-ray machines

4
Common Radiation Terms
Radioisotope - a generic name for a radioactive element Radionuclide - a specific radioisotope such as Uranium-235 These terms are often used interchangeably

5
Radiation Physics Ionizing Radiation Types of Radiation X-ray, Gamma
Radiation with enough energy to cause ionization of atoms by ejecting electrons from their atomic orbits Types of Radiation Electromagnetic (Photons - No Mass) X-ray, Gamma Particulate Alpha (helium nucleus), Beta (electron), Proton, Neutron
 X-ray, Gamma. Particulate. Alpha (helium nucleus), Beta (electron), Proton, Neutron.")
6
Types of Radiation Emitted from Radioactive Material
Particulate Charged Alpha Radiation Beta Radiation Uncharged Neutron Radiation Electromagnetic Gamma Radiation

7
Types of Ionizing Radiation
Alpha Particles Stopped by a sheet of paper Radiation Source Beta Particles Stopped by a layer of clothing or less than an inch of a substance (e.g. plastic) 5. Types of Ionizing Radiation Alpha particles. Alpha particles are ejected (thrown out of) the nuclei of some very heavy radioactive atoms (atomic number > 83). An alpha particle is composed of two neutrons and two protons. Alpha particles do not penetrate the dead layer of skin and can be stopped by a thin layer of paper or clothing. If an alpha emitting radioactive material gets inside the body through inhalation, ingestion, or through a wound, the emitted alpha particles can cause ionization that results in damage to tissue. It is less likely that a patient would be contaminated with an alpha emitter. Beta particles. A beta particle is an electron ejected from the nucleus of a radioactive atom. Depending on its energy, beta radiation can travel from inches to many feet in air and is only moderately penetrating in other materials. Some beta radiation can penetrate human skin to the layer where new skin cells are produced. If high enough quantities of beta emitting contaminants are allowed to remain on the skin for a prolonged period of time, they may cause skin injury. Beta emitting contaminants may be harmful if deposited internally. Protective clothing (e.g., universal precautions) typically provides sufficient protection against most external beta radiation. Gamma rays and x-rays (photons). Gamma rays and x-rays are able to travel many feet in air and many inches in human tissue. They readily penetrate most materials and are sometimes called “penetrating” radiation. Thick layers of dense materials are needed to shield against gamma radiation. Protective clothing provides little shielding from gamma and x radiation, but will prevent contamination of the skin with the gamma emitting radioactive material. Gamma and x radiation frequently accompanies the emission of beta and alpha radiation. Gamma Rays Stopped by inches to feet of concrete or less than an inch of lead
 5. Types of Ionizing Radiation. Alpha particles. Alpha particles are ejected (thrown out of) the nuclei of some very heavy radioactive atoms (atomic number > 83). An alpha particle is composed of two neutrons and two protons. Alpha particles do not penetrate the dead layer of skin and can be stopped by a thin layer of paper or clothing. If an alpha emitting radioactive material gets inside the body through inhalation, ingestion, or through a wound, the emitted alpha particles can cause ionization that results in damage to tissue. It is less likely that a patient would be contaminated with an alpha emitter. Beta particles. A beta particle is an electron ejected from the nucleus of a radioactive atom. Depending on its energy, beta radiation can travel from inches to many feet in air and is only moderately penetrating in other materials. Some beta radiation can penetrate human skin to the layer where new skin cells are produced. If high enough quantities of beta emitting contaminants are allowed to remain on the skin for a prolonged period of time, they may cause skin injury. Beta emitting contaminants may be harmful if deposited internally. Protective clothing (e.g., universal precautions) typically provides sufficient protection against most external beta radiation. Gamma rays and x-rays (photons). Gamma rays and x-rays are able to travel many feet in air and many inches in human tissue. They readily penetrate most materials and are sometimes called penetrating radiation. Thick layers of dense materials are needed to shield against gamma radiation. Protective clothing provides little shielding from gamma and x radiation, but will prevent contamination of the skin with the gamma emitting radioactive material. Gamma and x radiation frequently accompanies the emission of beta and alpha radiation. Gamma Rays. Stopped by inches to feet of concrete. or less than an inch of lead.")
8
Alpha and Beta Radiation
Typically emitted from a heavy element Most have energies between 4-8 MeV Particles up to 7.5 MeV stopped by dead skin layer (only a few microns penetration) Can be shielded by paper Penetrates a few cm in air Does not penetrate the dead layer of skin Beta Travels about 4 meters in air per MeV Penetrates about 0.5 cm in soft tissue per MeV Can reach the basal cell layer of skin
 Can be shielded by paper. Penetrates a few cm in air. Does not penetrate the dead layer of skin. Beta. Travels about 4 meters in air per MeV. Penetrates about 0.5 cm in soft tissue per MeV. Can reach the basal cell layer of skin.")
9
Pertinent Alpha Emitters

10
Neutron Radiation Neutral particle emitted from the nucleus
Can be very penetrating Requires special consideration for shielding Can induce radioactivity when absorbed by stable elements (N, Na, Al, S, Cl, P, etc.)
")
11
Electromagnetic Radiation
Energy = hf Energy expressed typically in KeV or MeV (not joules) Absorption of Electromagnetic Radiation by matter Photoelectric Compton Scattering Pair production (photon energy must exceed 1.02 MeV) Stochastic event Low energy photons more readily absorbed
 Absorption of Electromagnetic Radiation by matter. Photoelectric. Compton Scattering. Pair production (photon energy must exceed 1.02 MeV) Stochastic event. Low energy photons more readily absorbed.")
12
The Electromagnetic Spectrum

13
Gamma Radiation Electromagnetic energy emitted from the nucleus
Specific energies can be analyzed to identify source Very penetrating (many meters in air) Difficult to shield, often shielded with lead
 Difficult to shield, often shielded with lead.")
14
X-ray Radiation Electromagnetic energy emitted from outside the nucleus May be “machine-produced” by bombarding high energy electrons on a target May also be emitted from radioactive materials Similar shielding and penetrating powers as gamma radiation

15
Radiation Units Measure of Amount of radioactive material
Ionization in air Absorbed energy per mass Absorbed dose weighted by type of radiation Quantity Activity Exposure Absorbed Dose Dose Equivalent Unit curie (Ci) roentgen (R) rad rem 6. Radiation Units A curie is a very large amount of radioactivity. Contamination of individuals usually involve µCi to mCi quantities. Nuclear medicine patients are injected with µCi to mCi quantities of radioactive material for routine diagnostic exams. The basic unit of radiation dose is the rad. The rad is defined as the deposition of 0.01 joule of energy (a small amount) per kilogram (kg) of tissue. A rad of x-rays, a rad of gamma rays, and a rad of beta particles are about equally damaging to tissue. However, a rad of another type of ionizing radiation, such as alpha particles or neutrons, is much more damaging to tissue than a rad of gamma rays. The rem was introduced to take into account this variation in tissue damage. This is important because a person may be exposed to more than one type of radiation. For example, it was found that 100 rad of gamma and beta radiation produced the same effect as 100 rad of x-rays. However, only 20 rad of neutrons and 5 rad of alpha particles produced the same effect as 100 rad of x-rays. Therefore, neutron and alpha radiations were more potent and required fewer rad to produce the same effect. The number of rem is calculated by multiplying the number of rad by a radiation weighting factor that accounts for the relative amount of biological damage produced by a specific type of radiation. The radiation weighting factor for x-rays, gamma rays, and beta particles is 1. Thus, a rad of one of these radiations is equal to one rem. For other types of radiation (that are less likely to be present in accidents), the quality factor may be higher. The International Scientific System (SI) assigns different units to the quantities: 1 R = 2.58 X 10-4 C kg-1 1 gray (Gy) = 100 rad 1 sievert (Sv) = 100 rem 1 becquerel (Bq) = 1 disintegration per second For most types of radiation 1 R 1 rad 1 rem
 roentgen (R) rad. rem. 6. Radiation Units. A curie is a very large amount of radioactivity. Contamination of individuals usually involve µCi to mCi quantities. Nuclear medicine patients are injected with µCi to mCi quantities of radioactive material for routine diagnostic exams. The basic unit of radiation dose is the rad. The rad is defined as the deposition of 0.01 joule of energy (a small amount) per kilogram (kg) of tissue. A rad of x-rays, a rad of gamma rays, and a rad of beta particles are about equally damaging to tissue. However, a rad of another type of ionizing radiation, such as alpha particles or neutrons, is much more damaging to tissue than a rad of gamma rays. The rem was introduced to take into account this variation in tissue damage. This is important because a person may be exposed to more than one type of radiation. For example, it was found that 100 rad of gamma and beta radiation produced the same effect as 100 rad of x-rays. However, only 20 rad of neutrons and 5 rad of alpha particles produced the same effect as 100 rad of x-rays. Therefore, neutron and alpha radiations were more potent and required fewer rad to produce the same effect. The number of rem is calculated by multiplying the number of rad by a radiation weighting factor that accounts for the relative amount of biological damage produced by a specific type of radiation. The radiation weighting factor for x-rays, gamma rays, and beta particles is 1. Thus, a rad of one of these radiations is equal to one rem. For other types of radiation (that are less likely to be present in accidents), the quality factor may be higher. The International Scientific System (SI) assigns different units to the quantities: 1 R = 2.58 X 10-4 C kg-1 1 gray (Gy) = 100 rad. 1 sievert (Sv) = 100 rem 1 becquerel (Bq) = 1 disintegration per second. For most types of radiation 1 R 1 rad 1 rem.")
16
Units of Radioactivity
Quantity 1 Becquerel (Bq) = 1tps 1 Curie (Ci) = 3.7 x 1010 tps Exposure 1 Roentgen (R) = 2.58 x 10-4 C/Kgair 87.7 ergs/gair Exposure to Dose Relationship 1 R exposure 95 ergs/g absorption in muscle
 = 1tps. 1 Curie (Ci) = 3.7 x 1010 tps. Exposure. 1 Roentgen (R) = 2.58 x 10-4 C/Kgair. 87.7 ergs/gair. Exposure to Dose Relationship. 1 R exposure 95 ergs/g absorption in muscle.")
17
Half-Life The time required for a radioactive substance to loose 1/2 of its radioactivity Each radionuclide has a unique half-life Half-lives range from extremely short (fraction of a second) to billions of years
 to billions of years.")
18
Example of the Effect of Half-Life
Assume an initial amount of 32 uCi of TC-99m with a half-life (T1/2) of 6 hours after 1 half-life (6 h): uCi after 2 half-lives (12 h): uCi after 3 half-lives (18 h): uCi after 4 half-lives (24 h): uCi After 10 half-lives, less than 1/1000 of the original activity remains
 of 6 hours. after 1 half-life (6 h): 16 uCi. after 2 half-lives (12 h): 8 uCi. after 3 half-lives (18 h): 4 uCi. after 4 half-lives (24 h): 2 uCi. After 10 half-lives, less than 1/1000 of the original activity remains.")
19
Selected Radionuclides with Radiations
Half-Life Eff. Half-Life Hydrogen-3 12 y 12 d Cobalt-60 5.26 y 10 d Strontium-90 28 y 15 y Iodine-131 8.05 d 8 d Cesium-137 30 y 70 d Iridium-192 74 d - Radium-226 1602 y 44 y From Mettler, Jr., F.A. and Upton, A.C., Medical Effects of Ionizing Radiation 2nd edition

20
Radiation Dose Absorbed Dose (D)
1 Gray (Gy) = 1 J/Kg 1 rad = 100 ergs/g 100 rad = 1 Gy Dose Equivalent (HT) [ HT = DQ] 1 Seivert (Sv) = 1 J/Kg 1 rem = 100 ergs/g 100 rem = 1 Sv Deterministic Acute Effects Stochastic Late Effects Note: 1 MeV = 1.6 x Joules
 = 1 J/Kg. 1 rad = 100 ergs/g. 100 rad = 1 Gy. Dose Equivalent (HT) [ HT = DQ] 1 Seivert (Sv) = 1 J/Kg. 1 rem = 100 ergs/g. 100 rem = 1 Sv. Deterministic Acute Effects Stochastic Late Effects. Note: 1 MeV = 1.6 x Joules.")
21
Weighting Factors Organization NRC ICRU NCRP ICRP Weighting factor Q
WR X &Gamma Rays 1 Beta Rays Thermal Neutrons 2 5 Fast Neutrons 10 25 20 Hi Energy Protons Alpha Particles

22
Radiation Doses and Dose Limits
Flight from Los Angeles to London mrem Annual public dose limit mrem Annual natural background mrem Fetal dose limit mrem Barium enema mrem Annual radiation worker dose limit 5,000 mrem Heart catheterization (skin dose) ,000 mrem Life saving actions guidance (NCRP-116) ,000 mrem Mild acute radiation syndrome ,000 mrem LD50/60 for humans (bone marrow dose) ,000 mrem Radiation therapy (localized & fractionated) ,000,000 mrem 7. Radiation Doses and Dose Limits Radioactive material has always been a natural part of the earth. It has existed for millions of years in the crust of the earth, in building materials, in the food we eat, the air we breathe, and in nearly everything that surrounds us. Radiation from these materials, as well as cosmic radiation from the sun and universe, makes up the natural background radiation to which we are constantly exposed. On the average, persons are exposed to about 300 millirem per year from natural sources (NCRP Report No. 101). The guidance from NCRP Report No. 116, Limitation of Exposure to Ionizing Radiation, states that for life saving or equivalent purposes, workers may approach or exceed 50,000 mrem to a large portion of the body. Emergency exposures are considered once-in-a-lifetime. This is below the threshold for the acute radiation syndrome, discussed later. If an individual is exposed to more than 100 rem at one time, predictable signs and symptoms will develop within a few hours, days, or weeks depending on the magnitude of the dose. About half of all people exposed to a single dose of 350 rem will die within 60 days (LD50/60) without medical intervention. The large doses used in medicine for radiation therapy, while higher than this dose, are given to only part of the body and are typically given over a period of weeks. Heart catheterization is a skin dose; barium enema is an effective dose. (NRPB Report R-200, 1986) The dose limits are highlighted in orange.
 45,000 mrem. Life saving actions guidance (NCRP-116) 50,000 mrem. Mild acute radiation syndrome 200,000 mrem. LD50/60 for humans (bone marrow dose) 350,000 mrem. Radiation therapy (localized & fractionated) 6,000,000 mrem. 7. Radiation Doses and Dose Limits. Radioactive material has always been a natural part of the earth. It has existed for millions of years in the crust of the earth, in building materials, in the food we eat, the air we breathe, and in nearly everything that surrounds us. Radiation from these materials, as well as cosmic radiation from the sun and universe, makes up the natural background radiation to which we are constantly exposed. On the average, persons are exposed to about 300 millirem per year from natural sources (NCRP Report No. 101). The guidance from NCRP Report No. 116, Limitation of Exposure to Ionizing Radiation, states that for life saving or equivalent purposes, workers may approach or exceed 50,000 mrem to a large portion of the body. Emergency exposures are considered once-in-a-lifetime. This is below the threshold for the acute radiation syndrome, discussed later. If an individual is exposed to more than 100 rem at one time, predictable signs and symptoms will develop within a few hours, days, or weeks depending on the magnitude of the dose. About half of all people exposed to a single dose of 350 rem will die within 60 days (LD50/60) without medical intervention. The large doses used in medicine for radiation therapy, while higher than this dose, are given to only part of the body and are typically given over a period of weeks. Heart catheterization is a skin dose; barium enema is an effective dose. (NRPB Report R-200, 1986) The dose limits are highlighted in orange.")
23
Radioactive Material Radioactive material consists of atoms with unstable nuclei The atoms spontaneously change (decay) to more stable forms and emit radiation A person who is contaminated has radioactive material on their skin or inside their body (e.g., inhalation, ingestion or wound contamination) 8. Radioactive Material The difference between radioactive material and radiation should be explained. Radioactivity is a mechanism whereby an unstable nucleus rearranges itself to become more stable. The process often involves the ejection of charged particles from the atomic nuclei. This ejection of particles (beta or alpha) is often accompanied by the emission of gamma rays from the nucleus or x-rays from the atom’s electron shells. Beta particles, alpha particles, gamma rays and x-rays are all forms of radiation that can be emitted from radioactive atoms. Radioactive contamination is simply radioactive material (often attached to dust or dirt) that is either on the skin or clothes of the patient or has been taken into the body via inhalation, ingestion, or through a wound. Usually most of the external contamination can be removed from the patient by carefully removing the patient’s clothing.
 to more stable forms and emit radiation. A person who is contaminated has radioactive material on their skin or inside their body (e.g., inhalation, ingestion or wound contamination) 8. Radioactive Material. The difference between radioactive material and radiation should be explained. Radioactivity is a mechanism whereby an unstable nucleus rearranges itself to become more stable. The process often involves the ejection of charged particles from the atomic nuclei. This ejection of particles (beta or alpha) is often accompanied by the emission of gamma rays from the nucleus or x-rays from the atom’s electron shells. Beta particles, alpha particles, gamma rays and x-rays are all forms of radiation that can be emitted from radioactive atoms. Radioactive contamination is simply radioactive material (often attached to dust or dirt) that is either on the skin or clothes of the patient or has been taken into the body via inhalation, ingestion, or through a wound. Usually most of the external contamination can be removed from the patient by carefully removing the patient’s clothing.")
24
Examples of Radioactive Materials
Physical Radionuclide Half-Life Activity Use Cesium yrs x106 Ci Food Irradiator Cobalt yrs ,000 Ci Cancer Therapy Plutonium ,000 yrs Ci Nuclear Weapon Iridium days Ci Industrial Radiography Hydrogen yrs Ci Exit Signs Strontium yrs Ci Eye Therapy Device Iodine days Ci Nuclear Medicine Therapy Technetium-99m hrs Ci Diagnostic Imaging Americium yrs Ci Smoke Detectors Radon days pCi/l Environmental Level 10. Examples of Radioactive Materials Radioactive materials emit ionizing radiation. They are used in medical diagnosis (nuclear medicine), medical therapy (cancer treatment), industry (food irradiation), and for research. Many radioactive materials, including radioactive waste, are commercially shipped in special containers. A radionuclide is chemically identical to and behaves in the body the same way as the non-radioactive form of the element. For example, radioactive iodine (e.g. I-131) is concentrated in the thyroid in the same way as non-radioactive iodine (i.e. I-127). Quantities of radioactive material (i.e. activity) range from trivial amounts in typical laboratories, to much larger quantities, such as in nuclear reactors. Half-lives can range from seconds to millions of years. The nuclides that are in orange are those that are considered to be potential nuclides that could be present in a radiological dispersal device.
, medical therapy (cancer treatment), industry (food irradiation), and for research. Many radioactive materials, including radioactive waste, are commercially shipped in special containers. A radionuclide is chemically identical to and behaves in the body the same way as the non-radioactive form of the element. For example, radioactive iodine (e.g. I-131) is concentrated in the thyroid in the same way as non-radioactive iodine (i.e. I-127). Quantities of radioactive material (i.e. activity) range from trivial amounts in typical laboratories, to much larger quantities, such as in nuclear reactors. Half-lives can range from seconds to millions of years. The nuclides that are in orange are those that are considered to be potential nuclides that could be present in a radiological dispersal device.")
25
Radiation vs. Radioactive Material
The energetic emissions of radioactive material Can be subatomic particles (, , n), photons (X-ray, ) or combinations Results in ionization of the absorbing material (if living tissue radiation injury) Radioactive Material Any substance that spontaneously gives off radiation Can be in various chemical forms If not contained (sealed source) can lead to contamination - External, Internal or Both
, photons (X-ray, ) or combinations. Results in ionization of the absorbing material (if living tissue radiation injury) Radioactive Material. Any substance that spontaneously gives off radiation. Can be in various chemical forms. If not contained (sealed source) can lead to contamination - External, Internal or Both.")
26
Half-Life (HL) Physical Half-Life Biological Half-Life
Time (in minutes, hours, days or years) required for the activity of a radioactive material to decrease by one half due to radioactive decay Biological Half-Life Time required for the body to eliminate half of the radioactive material (depends on the chemical form) Effective Half-Life The net effect of the combination of the physical & biological half-lives in removing the radioactive material from the body Half-lives range from fractions of seconds to millions of years 1 HL = 50% 2 HL = 25% 3 HL = 12.5% 9. Half-Life In any sample of radioactive material, the amount of radioactive material constantly decreases with time because of radioactive decay. The physical half-life is the amount of time required for a given amount of radioactive material to be reduced to half the initial amount by radioactive decay. The biological half-life is the time required for the human body to eliminate half of the radioactive material taken into it. For many radioactive materials, the elimination from the body occurs via urination. However, depending on the chemical composition of the radioactive material, other pathways can also help to eliminate the radioactive material from the body. The effective half-life is a measure of the time it takes for half the radioactive material taken into the body to disappear from the body. Both the physical half-life and the biological half-life contribute to the elimination of the radioactive material from the body. The combination of these two half-lives is called the effective half-life. After one half-life, half of the material remains. After a second half-life, a half of a half, i.e. 25% of the initial amount remains. After 10 half-lives, about 1/1000 remains. After 20 half-lives, only one millionth of the material remains.
 required for the activity of a radioactive material to decrease by one half due to radioactive decay. Biological Half-Life. Time required for the body to eliminate half of the radioactive material (depends on the chemical form) Effective Half-Life. The net effect of the combination of the physical & biological half-lives in removing the radioactive material from the body. Half-lives range from fractions of seconds to millions of years. 1 HL = 50% 2 HL = 25% 3 HL = 12.5% 9. Half-Life. In any sample of radioactive material, the amount of radioactive material constantly decreases with time because of radioactive decay. The physical half-life is the amount of time required for a given amount of radioactive material to be reduced to half the initial amount by radioactive decay. The biological half-life is the time required for the human body to eliminate half of the radioactive material taken into it. For many radioactive materials, the elimination from the body occurs via urination. However, depending on the chemical composition of the radioactive material, other pathways can also help to eliminate the radioactive material from the body. The effective half-life is a measure of the time it takes for half the radioactive material taken into the body to disappear from the body. Both the physical half-life and the biological half-life contribute to the elimination of the radioactive material from the body. The combination of these two half-lives is called the effective half-life. After one half-life, half of the material remains. After a second half-life, a half of a half, i.e. 25% of the initial amount remains. After 10 half-lives, about 1/1000 remains. After 20 half-lives, only one millionth of the material remains.")
27
Criticality Incident Operation Upshot/Knothole, a 1953 test of nuclear artillery projectile at Nevada Test Site

28
Nuclear Fission

29
Fissile Material U-235 Pu-239
Enriched from 0.7% (Natural) to 3% > 90% Used: Commercial Reactors Research Reactors Naval Reactors Atomic Bomb Pu-239 Byproduct of U-235 fission Used in Breeder Reactor Also can be weaponized
 to 3% > 90% Used: Commercial Reactors. Research Reactors. Naval Reactors. Atomic Bomb. Pu-239. Byproduct of U-235 fission. Used in Breeder Reactor. Also can be weaponized.")
30
Radionuclides of Concern

31
Causes of Radiation Exposure/Contamination
Accidents Nuclear reactor Medical radiation therapy Industrial irradiator Lost/stolen medical or industrial radioactive sources Transportation Terrorist Event Low yield nuclear weapon Radiological dispersal device (dirty bomb) Attack on or sabotage of a nuclear facility 12. Causes of Radiation Exposure and Contamination Accidents - There are several settings or scenarios in which radiation accidents may occur: nuclear reactor accidents; medical radiation therapy accidents or errors in treatment dose; accidental overexposures from industrial irradiators; lost, stolen or misused medical or industrial radioactive sources; and accidents during the transportation of radioactive material. Terrorist Use of Nuclear Materials - The use of radioactive materials in an RDD or a nuclear weapon by a terrorist is a remote but plausible threat. The medical consequences depend on the type of device used in a terrorist event. An attack on or sabotage of a nuclear facility, such as an irradiation facility or a nuclear power plant, could result in the release of very large amounts of radioactive material. Radiological Dispersal Device (RDD) - A RDD disperses radioactive material for the purpose of terrorism. A RDD that uses a conventional explosive (e.g., TNT or a plastic explosive) to disperse the radioactive material is called a “dirty bomb”. A dirty bomb is NOT an atomic bomb. The initial explosion may kill or injure those closest to the bomb, while the radioactive material remains to expose and contaminate survivors and emergency responders. Low Yield Nuclear Weapon - A low yield nuclear weapon or partial failure of a high yield weapon could cause a low yield nuclear detonation. For example, if one considers the consequences of a 0.1 kiloton yield nuclear detonation (less than 1/100 the size of the weapon used on Hiroshima), then the following would occur within one minute surrounding ground zero. The effects listed below do not take into account that multiple injuries caused by the interaction of the various types of injury will increase the probability of fatality. (NCRP Report No. 138) - The range for 50% mortality from trauma from the blast is approximately 150 yards. - The range for 50% mortality from thermal burns is approximately 220 yards. - The range for 400 rad from gamma and neutron radiation would be approximately 1/3 mile. - The range for 400 rad in the first hour from radioactive fallout would be almost 2 miles in the downwind direction. - As the size of the weapon increases, the effects encompass a greater distance. This will result in the release of widespread contamination and substantial air blast and heat.
 Attack on or sabotage of a nuclear facility. 12. Causes of Radiation Exposure and Contamination. Accidents - There are several settings or scenarios in which radiation accidents may occur: nuclear reactor accidents; medical radiation therapy accidents or errors in treatment dose; accidental overexposures from industrial irradiators; lost, stolen or misused medical or industrial radioactive sources; and accidents during the transportation of radioactive material. Terrorist Use of Nuclear Materials - The use of radioactive materials in an RDD or a nuclear weapon by a terrorist is a remote but plausible threat. The medical consequences depend on the type of device used in a terrorist event. An attack on or sabotage of a nuclear facility, such as an irradiation facility or a nuclear power plant, could result in the release of very large amounts of radioactive material. Radiological Dispersal Device (RDD) - A RDD disperses radioactive material for the purpose of terrorism. A RDD that uses a conventional explosive (e.g., TNT or a plastic explosive) to disperse the radioactive material is called a dirty bomb . A dirty bomb is NOT an atomic bomb. The initial explosion may kill or injure those closest to the bomb, while the radioactive material remains to expose and contaminate survivors and emergency responders. Low Yield Nuclear Weapon - A low yield nuclear weapon or partial failure of a high yield weapon could cause a low yield nuclear detonation. For example, if one considers the consequences of a 0.1 kiloton yield nuclear detonation (less than 1/100 the size of the weapon used on Hiroshima), then the following would occur within one minute surrounding ground zero. The effects listed below do not take into account that multiple injuries caused by the interaction of the various types of injury will increase the probability of fatality. (NCRP Report No. 138) - The range for 50% mortality from trauma from the blast is approximately 150 yards. - The range for 50% mortality from thermal burns is approximately 220 yards. - The range for 400 rad from gamma and neutron radiation would be approximately 1/3 mile. - The range for 400 rad in the first hour from radioactive fallout would be almost 2 miles in the downwind direction. - As the size of the weapon increases, the effects encompass a greater distance. This will result in the release of widespread contamination and substantial air blast and heat.")
32
Size of Event Event No. of Deaths Most Deaths Due to Radiation
None/Few Radiation Accident Radioactive Few/Moderate Blast Trauma Dispersal (Depends on size of explosion & 13. Scope of Event 428 major radiation accidents have been reported worldwide in the years 1944 to These accidents caused 126 deaths due to radiation. Their effects were dependent on exposure, contamination and the number of people involved. There were an additional 8 non-radiation deaths that would likely have resulted in eventual death due to the radiation. (REAC/TS Registry, 2002) There have been no uses of radioactive dispersal devices. The outcome of such an event would depend on the size of the explosion, the radioactive material involved, the activity (amount) of the radioactive material, the number of people in the vicinity and the effectiveness of the emergency response. There have been no low-yield nuclear weapon detonations by terrorists. The outcome from such an event would depend on the yield, the location of the detonation and the number of people in the vicinity. Device proximity of persons) Low Yield Large Blast Trauma Nuclear Weapon (e.g. tens of thousands in Thermal Burns an urban area even from Radiation Exposure 0.1 kT weapon) Fallout (Depends on Distance)
 There have been no uses of radioactive dispersal devices. The outcome of such an event would depend on the size of the explosion, the radioactive material involved, the activity (amount) of the radioactive material, the number of people in the vicinity and the effectiveness of the emergency response. There have been no low-yield nuclear weapon detonations by terrorists. The outcome from such an event would depend on the yield, the location of the detonation and the number of people in the vicinity. Device. proximity of persons) Low Yield. Large. Blast Trauma. Nuclear Weapon. (e.g. tens of thousands in. Thermal Burns. an urban area even from. Radiation Exposure. 0.1 kT weapon) Fallout. (Depends on Distance)")
33
Effective dose averaged over
Dose Limits - ICRP 60 Application Occupational Public Whole Body 20 mSv/year Effective dose averaged over 5 years, max: 50 mSv/yr 1 mSv in 1 year Annual Equiv. Dose: Lens of eye 150 mSv 15 mSv Skin 500 mSv 50 mSv Hands & Feet _

34
Emergency Exposure Guidelines - ICRP 60
Dose Limit (Whole Body) Activity Performed Conditions 5 rems All….. ……. 10 rems Protecting major property Where lower dose limit not practicable. 25 rems Lifesaving or protection of large populations Where lower dose limit not practicable >25 rems Only on a voluntary basis to personnel fully aware of the risks involved
 Activity Performed. Conditions. 5 rems. All….. ……. 10 rems. Protecting major property. Where lower dose limit not practicable. 25 rems. Lifesaving or protection of large populations. Where lower dose limit not practicable. >25 rems. Only on a voluntary basis to personnel fully aware of the risks involved.")
35
Radiography Source

36
Sealed Source Accident
13 Curie Cs-137 Radiography Source Found by a man at an Argentina construction site Carried in front pockets for 18 hours

37
Accident Dose Calculation
Cs-137 Gamma Constant = R-m2/hr-Ci 0.323 R-m2 x (18hr)(13Ci) = 755,820 R hr-Ci (0.01m)2
(13Ci) = 755,820 R. hr-Ci (0.01m)2.")
38
Accident Isodose Curves

39
Basic Radiobiology Atom Ionization in Water or Cell Molecules
Molecule Chemical Damage Bond Breakage DNA Chromosomal Aberration Cell Death Mutation

40
Radiosensitivity (most to least):
Lymphocytes Erythroblasts Myeloblasts Epithelial Cells Intestinal crypts Testis Ovary Skin Secretory glands Lungs and bile ducts Endothelial Cells Connective Tissue Cells Tubular Cells of Kidneys Bone Cells Nerve Cells Brain Cells Muscle Cells 19-A

41
Classification of Medical Radiation Problems
Anxiety Acute Radiation Syndrome Local Radiation Injury External Radionuclide Contamination Local Trauma with Radionuclide Contamination Internal Radionuclide Contamination

42
Radiation Injuries External exposure to penetrating radiation
Criticality Incident (,N) Sealed Source (,) External Contamination (, ) Beam Generator (,N) Internal contamination with radionuclides Wound Contamination (, , ) Injection (, , ) Inhalation (, , ) Ingestion (, , )
 Sealed Source (,) External Contamination (, ) Beam Generator (,N) Internal contamination with radionuclides. Wound Contamination (, , ) Injection (, , ) Inhalation (, , ) Ingestion (, , )")
43
Late Health Effects from Radiation
Radiation is a weak carcinogen at low doses No unique effects (type, latency, pathology) Natural incidence of cancer ~ 40%; mortality ~ 25% Risk of fatal cancer is estimated as ~ 4% per 100 rem A dose of 5 rem increases the risk of fatal cancer by ~ 0.2% A dose of 25 rem increases the risk of fatal cancer by ~ 1% 37. Chronic Health Effects from Radiation High radiation doses have been linked to a modest increase in the incidence of cancer in exposed populations, such as the atomic bomb survivors. At low doses, below about 20 rem, the potential for cancer causation is uncertain and generally believed to be quite small. The natural incidence of cancer in the population of the United States, over a lifetime, is estimated to be approximately 40% and the risk of mortality is approximately 25%. [Reference - SEER (Surveillance, Epidemiology and End Results) Program of the National Cancer Institute] Risk of fatal cancer from ICRP Publication 60. There are several sets of recommendations for acceptable doses to emergency workers performing life saving actions. While these doses are 5 to 10 times higher than annual occupational dose limits, it represents a modest increase in cancer risk during life saving measures. EPA / NRC rem NCRP / ICRP Approach or exceed 50 rem (EPA, Manual of Protective Action Guides and Protective Actions for Nuclear Incidents, 1992) (NCRP Report 116, Limitation on Exposure to Ionizing Radiation, 1993) (IRCP Report 60, 1990 Recommendations of the International Commission on Radiological Protection, 1991)
 Natural incidence of cancer ~ 40%; mortality ~ 25% Risk of fatal cancer is estimated as ~ 4% per 100 rem. A dose of 5 rem increases the risk of fatal cancer by ~ 0.2% A dose of 25 rem increases the risk of fatal cancer by ~ 1% 37. Chronic Health Effects from Radiation. High radiation doses have been linked to a modest increase in the incidence of cancer in exposed populations, such as the atomic bomb survivors. At low doses, below about 20 rem, the potential for cancer causation is uncertain and generally believed to be quite small. The natural incidence of cancer in the population of the United States, over a lifetime, is estimated to be approximately 40% and the risk of mortality is approximately 25%. [Reference - SEER (Surveillance, Epidemiology and End Results) Program of the National Cancer Institute] Risk of fatal cancer from ICRP Publication 60. There are several sets of recommendations for acceptable doses to emergency workers performing life saving actions. While these doses are 5 to 10 times higher than annual occupational dose limits, it represents a modest increase in cancer risk during life saving measures. EPA / NRC 25 rem. NCRP / ICRP Approach or exceed 50 rem. (EPA, Manual of Protective Action Guides and Protective Actions for Nuclear Incidents, 1992) (NCRP Report 116, Limitation on Exposure to Ionizing Radiation, 1993) (IRCP Report 60, 1990 Recommendations of the International Commission on Radiological Protection, 1991)")
44
What are the Risks to Future Children? Hereditary Effects
Magnitude of hereditary risk per rem is 10% that of fatal cancer risk Risk to caregivers who would likely receive low doses is very small - 5 rem increases the risk of severe hereditary effects by ~ 0.02% Risk of severe hereditary effects to a patient population receiving high doses is estimated as ~ 0.4% per 100 rem 38. What are the Risks to Future Children? Hereditary Effects Concern over radiation-induced hereditary (genetic) effects is quite common due to a century of misrepresentation, by the media and the entertainment industry, of radiation’s ability to produce hereditary effects. The natural incidence of malformations and genetic disease at 1-2 years of age is 6-10%. (Mossman KL, Hill LT: Radiation Risks in Pregnancy , Obsts Gynecol 60: , 1982) No direct evidence of hereditary effects exceeding normal incidence have been observed in any of the studies of humans exposed to radiation, even with high doses. Risk of severe hereditary effects from UNSCEAR Hereditary Effects of Radiation, 2001.
 effects is quite common due to a century of misrepresentation, by the media and the entertainment industry, of radiation’s ability to produce hereditary effects. The natural incidence of malformations and genetic disease at 1-2 years of age is 6-10%. (Mossman KL, Hill LT: Radiation Risks in Pregnancy , Obsts Gynecol 60: , 1982) No direct evidence of hereditary effects exceeding normal incidence have been observed in any of the studies of humans exposed to radiation, even with high doses. Risk of severe hereditary effects from UNSCEAR Hereditary Effects of Radiation,")
45
Fetal Irradiation No significant risk of adverse developmental effects below 10 rem
Weeks After Fertilization Period of Development Effects <2 2-7 7-40 All Pre-implantation Organogenesis Fetal Little chance of malformation. Most probable effect, if any, is death of embryo. Reduced lethal effects. Teratogenic effects. Growth retardation. Impaired mental ability. Growth retardation with higher doses. Increased childhood cancer risk. (~ 0.6% per 10 rem) 39. Fetal Irradiation Termination of pregnancy is NOT justified based upon radiation risks for fetal doses less than 10 rem. Excess childhood cancer risk is ~0.06% per rem. Normal childhood cancer incidence is 0.075%. Fetal doses greater than 50 rem can cause significant fetal damage, the magnitude and type of which is a function of dose and stage of pregnancy. For fetal doses between 10 and 50 rem, decisions regarding termination of pregnancy should be made based upon individual circumstances.
 39. Fetal Irradiation. Termination of pregnancy is NOT justified based upon radiation risks for fetal doses less than 10 rem. Excess childhood cancer risk is ~0.06% per rem. Normal childhood cancer incidence is 0.075%. Fetal doses greater than 50 rem can cause significant fetal damage, the magnitude and type of which is a function of dose and stage of pregnancy. For fetal doses between 10 and 50 rem, decisions regarding termination of pregnancy should be made based upon individual circumstances.")
46
Types of Radiation Hazards
Internal Contamination External Exposure - whole-body or partial-body (no radiation hazard to EMS staff) Contaminated - external radioactive material: on the skin internal radioactive material: inhaled, swallowed, absorbed through skin or wounds External Contamination External Exposure 11. Types of Radiation Hazards Patients who have only been exposed to the radiation from a radioactive source or a machine, such as an x-ray machine or a linear accelerator, are not contaminated and do not pose any radiation contamination or exposure potential for hospital personnel. Radiation safety precautions are not needed for patients who have only been exposed and are not contaminated. Patients with radioactive material on them or inside their bodies are said to be contaminated. Contaminated patients require care in handling to effectively remove and control the contamination. Analogy - You can think of radiation exposure and radioactive material in terms of a trip to the beach. Sand is like radioactivity. The sun is like radiation exposure. Once you go inside, you are not in the sun any longer and there is no more exposure (radiation stops). On the other hand, most of the sand came off when you walked off the beach, however, some sand remains on your skin until you physically remove it (brush or wash it off). The same is true for radioactivity contamination on the skin. A small amount may remain on the skin and need to be washed off.
 Contaminated - external radioactive material: on the skin. internal radioactive material: inhaled, swallowed, absorbed through skin or wounds. External. Contamination. External. Exposure. 11. Types of Radiation Hazards. Patients who have only been exposed to the radiation from a radioactive source or a machine, such as an x-ray machine or a linear accelerator, are not contaminated and do not pose any radiation contamination or exposure potential for hospital personnel. Radiation safety precautions are not needed for patients who have only been exposed and are not contaminated. Patients with radioactive material on them or inside their bodies are said to be contaminated. Contaminated patients require care in handling to effectively remove and control the contamination. Analogy - You can think of radiation exposure and radioactive material in terms of a trip to the beach. Sand is like radioactivity. The sun is like radiation exposure. Once you go inside, you are not in the sun any longer and there is no more exposure (radiation stops). On the other hand, most of the sand came off when you walked off the beach, however, some sand remains on your skin until you physically remove it (brush or wash it off). The same is true for radioactivity contamination on the skin. A small amount may remain on the skin and need to be washed off.")
47
Radioactive Contamination
Contamination is simply the presence of radioactive material where it is not wanted Persons may be contaminated either externally, internally or both Exposure does not necessarily imply contamination

48
In order to limit the amount of radiation you are exposed to, think about: SHIELDING, DISTANCE and TIME Shielding: If you have a thick shield between yourself and the radioactive materials more of the radiation will be absorbed, and you will be exposed to less. Distance: The farther away from the blast and the fallout the lower your exposure. Time: Minimizing time spent exposed will also reduce your risk.

49
ALARA Techniques Work quickly and efficiently (TIME)
Rotate personnel if qualified replacements are available (TIME) When not involved in patient care, remain a few feet away from the patient (DISTANCE) Use long-handled forceps to remove contaminated particles, contaminated dressings, etc. (DISTANCE) Remove contaminated materials from the treatment area (DISTANCE & QUANTITY) Put contaminated metal or glass in lead in lead “pigs” obtained from nuclear medicine department (SHIELDING)
 When not involved in patient care, remain a few feet away from the patient (DISTANCE) Use long-handled forceps to remove contaminated particles, contaminated dressings, etc. (DISTANCE) Remove contaminated materials from the treatment area (DISTANCE & QUANTITY) Put contaminated metal or glass in lead in lead pigs obtained from nuclear medicine department (SHIELDING)")
50
Radiation Protection: Reducing Radiation Exposure
Time Minimize time spent near radiation sources To Limit Caregiver Dose to 5 rem Distance Rate Stay time 1 ft R/hr min 2 ft R/hr hr 5 ft R/hr hr 8 ft R/hr hr Distance Maintain maximal practical distance from radiation source 14. Reducing Radiation Exposure There are three methods for reducing radiation exposure: time, distance, and shielding. All three of these methods can be used to keep radiation exposure to a minimum. The longer a person is exposed to a radiation source, the higher will be the dose received. To minimize the dose, reduce the time of exposure to the radiation. For example, ED nurses who do not have to stand beside a contaminated patient can minimize exposure by stepping close to the patient only when assistance is needed and stepping away as soon as they are done. In addition to minimizing the exposure time, the nurse can further reduce exposure by taking advantage of distance. Radiation dose rate falls off very quickly as the distance between the radiation source and the individual is increased. Time and distance are effective methods of minimizing dose. Another method of minimizing dose is through the use of shielding. Radiology personnel use leaded aprons to shield themselves from the x-rays that are scattered from the patient undergoing an x-ray procedure. Leaded aprons are not recommended and usually provide little shielding protection from the types of radiation expected from contaminated patients. An effective way to use shielding is to place radioactive materials removed from patients into lead containers called “pigs.” The thick lead walls of these containers absorb the radiation from the radioactive material. Shielding Place radioactive sources in a lead container

51
Risk to Contaminated Patient
ARS, local radiation injury or contamination (both internal & external) never demands immediate medical attention. Priority 1: True medical emergencies ABC’s Bleeding assessment Trauma assessment Wound assessment Remove contaminated clothing as soon as reasonably possible (removes 80% of external contamination) Proceed with decontamination procedures after patient stabilized
 never demands immediate medical attention. Priority 1: True medical emergencies. ABC’s. Bleeding assessment. Trauma assessment. Wound assessment. Remove contaminated clothing as soon as reasonably possible (removes 80% of external contamination) Proceed with decontamination procedures after patient stabilized.")
52
Risk to Healthcare Provider
Minimal if using proper precautions Remember ALARA techniques Worst case - 15 mSv/hr close to contaminated wound At 1 foot ( 30 cm) mSv/hr NCRP public monthly equivalent dose to embryo/fetus: 0.5 mSv
 mSv/hr. NCRP public monthly equivalent dose to embryo/fetus: 0.5 mSv.")
53
Healthcare Provider - Controlling the Spread of Contamination
Goal: Minimize and control contamination Use proper protective clothing Do not eat drink or smoke in contamination areas Check yourself for contamination prior to leaving a potentially contaminated area Limit access to treatment area to necessary personnel only

54
Putting It All Together

55
Radiation Terrorism and Response
OUTLINE Radiation Terrorism and Response Radiation Basics Radiation Protection Rules Radiation Threats Nuclear device, “dirty” bomb Equivalent Experiences: Chernobyl, Goiana 4. Health Management of Affected Population

56
Mass Exposure Events Criticality Events Nuclide Contamination
Improvised Nuclear Device (IND) Reactor Release Nuclide Contamination Radiological Dispersal Device (RDD) aka: Dirty Bomb Intentional Contamination of Resources External Radiation Source -- Industrial or Medical Source
 Reactor Release. Nuclide Contamination. Radiological Dispersal Device (RDD) aka: Dirty Bomb. Intentional Contamination of Resources. External Radiation Source. -- Industrial or Medical Source.")
57
Injury Sources From Nuclear Device Detonation
Terrorist Event Low yield nuclear weapon Energy Distribution 50% Blast 35% Thermal Radiation 15% Ionizing Radiation Health Consequences Injury Burns Penetrating Ionizing Radiation Prompt (1/3) Delayed (2/3) Fallout Contamination
 Delayed (2/3) Fallout. Contamination.")
58
A nuclear weapon is expected to cause many deaths and injuries: radiation is not the primary hazard
Blast and thermal effect comprise of the majority of effects/casualties Radiation lethality out-distances thermal and blast damage only in low yield weapons (≤ 1 kiloton)
")
59
Thermal: 35% of the energy
1st “flash” Pulse Thermal pulse . Immediately after an explosion, energy is emitted in the form of thermal radiation and, due to the extremely high temperatures, as x rays, which are absorbed within a few feet of air. The energy is then re-emitted and, due to certain phenomena occurring within the fireball, the secondary thermal radiation emission occurs in two pulses. First pulse. The first pulse lasts only about one tenth of a second. It consists of approximately 1 percent of the total thermal radiation release, and much of the thermal release is in the ultraviolet region. Although ultraviolet radiation can cause skin burns, it appears that this occurs only at ranges at which other thermal radiation effects are more serious. However, although this first pulse may be disregarded as a source of skin burns, it is capable of producing permanent or temporary effects on the eyes, especially if one is looking in the direction of the detonation at the time of the explosion. Second pulse. The second pulse lasts for several seconds and carries about 99 percent of the total thermal radiation energy. Since the temperature is lower than that in the first pulse, most of the rays reaching the Earth consist of visible and infrared light. This radiation is the main cause of various degrees of skin burns suffered by exposed individuals up to at least 12 miles. Flash burns. This image of a Nagasaki woman shows flash burns in the pattern of the kimono she was wearing at the time of the blast. The light-colored fabric reflected the thermal radiation whereas the dark-colored fabric absorbed it and became hot, causing contact burns on the skin immediately beneath the fabric. Medical records indicate that, in some cases, dark-colored clothing actually burst into flames and ignited the undergarments, causing flame burns. It should be noted that light-colored clothing does NOT ensure total protection from thermal radiation. Some light-colored fabrics actually transmit enough thermal radiation to allow direct flash burning of the skin. 2nd pulse (99% of the energy) The pattern is from the dark colored areas on her kimono
 The pattern is from the dark. colored areas on her kimono.")
60
Long distance visual effects
Retinal burn: visual capacity is permanently lost in the burned area. Retinal burns can be produced at great distances from the nuclear detonation because the probability of occurrence does not follow the inverse square law as is true of many other types of nuclear radiation. Eye injuries. Ultraviolet radiation primarily is responsible for eye injuries, which can be transient, like flash blindness, or permanent, like retinal burns. Flash blindness is the most common eye injury, but ultraviolet radiation can cause retinal burns if a person looks directly at the explosion. Flash blindness. Flash blindness, also referred to as "dazzle," is a temporary impairment of vision caused by a bleaching of the rods and cones in the retina. It can be produced by scattered light and does not necessarily require the eye to be focused on the light source, the fireball in the case of a nuclear detonation. Flash blindness usually blanks out the entire field of vision with a bright afterimage. Fortunately, the effects are temporary, and complete recovery occurs within a short time. Retinal burns. A retinal burn is a permanent injury that occurs when the retinal tissue is heated excessively by an extremely bright image, the fireball in this case. The underlying pigmented cells absorb much of the light (radiation) energy, and the temperature is increased in that area. A temperature elevation of 12 ƒC to 20 ƒC in the eye will produce a thermal injury that involves both the pigmented layer and the adjacent rods and cones. Thus, visual capacity is permanently lost in the burned area. The natural tendency of people to look at a fireball increases the chance of retinal burns. Also worthy of note is that retinal burns can be produced at great distances from the nuclear detonation because the probability of occurrence does not follow the inverse square law as is true of many other types of nuclear radiation. Protection against thermal radiation . Thermal radiation travels at the speed of light. So, unless you have adequate forewarning, there is little you can do to protect yourself from injury. If provided advance warning, any light-impermeable object provides adequate protection from direct exposure since electromagnetic radiation waves travel in a straight line. Protective barriers might include hills, buildings, tanks, bunkers, and trees. Loose-fitting, light-colored clothing provides a degree of protection because of the insulating layer of air between the clothing and the skin and because it reflects some of the thermal radiation Flash Blindness, also referred to as "dazzle," is a temporary impairment of vision. Victim does not have to be looking directly at the source for this to occur. Nighttime greatly increases distance of effect
 energy, and the temperature is increased in that area. A temperature elevation of 12 ƒC to 20 ƒC in the eye will produce a thermal injury that involves both the pigmented layer and the adjacent rods and cones. Thus, visual capacity is permanently lost in the burned area. The natural tendency of people to look at a fireball increases the chance of retinal burns. Also worthy of note is that retinal burns can be produced at great distances from the nuclear detonation because the probability of occurrence does not follow the inverse square law as is true of many other types of nuclear radiation. Protection against thermal radiation . Thermal radiation travels at the speed of light. So, unless you have adequate forewarning, there is little you can do to protect yourself from injury. If provided advance warning, any light-impermeable object provides adequate protection from direct exposure since electromagnetic radiation waves travel in a straight line. Protective barriers might include hills, buildings, tanks, bunkers, and trees. Loose-fitting, light-colored clothing provides a degree of protection because of the insulating layer of air between the clothing and the skin and because it reflects some of the thermal radiation. Flash Blindness, also referred to as dazzle, is a temporary impairment of vision. Victim does not have to be looking directly at the source for this to occur. Nighttime greatly increases distance of effect.")
61
Fallout: important for surface bursts
A nuclear detonation results in a fireball with a temperature estimated to be several tens of millions of degrees. The radioactive particles resulting from nuclear fission and activation of surrounding materials are carried up by the fireball and then drift downwind to later settle on the ground. Nuclear fallout The detonation of a nuclear weapon releases a tremendous amount of energy. While the majority of that released is blast and thermal energy, 15 percent of it is in the form of nuclear radiation. Nuclear radiation is categorized as initial or delayed, according to the time after detonation that it is produced. Initial radiation, in the form of gamma rays, is produced within the first 60 seconds after detonation. Within that 60 seconds, the fireball reaches an estimated height of 2 miles, the estimated effective range of gamma rays in air. Delayed radiation is that produced after the first 60 seconds and includes induced radiation and fallout. Process and product The term "fallout" was used to describe radioactive material "falling out" of the mushroom cloud produced by the explosion of the first nuclear device, the TRINITY, detonated in Alamogordo, New Mexico, on July 16, Today, the term refers both to the process by which radioactively contaminated particles fall back to Earth and to the airborne, radioactively contaminated dust and debris. Fallout is classified as early fallout and delayed fallout. Early fallout, that which returns to Earth within 24 hours of detonation, tends to be particles that have a high concentration of radioactivity and that vary from 0.01 to 1 centimeter. The particles travel a few hundred miles, with the larger particles returning closer than smaller particles to ground zero. Delayed fallout, that which returns to Earth later than 24 hours after a detonation, consists of particles from approximately 0.01 centimeter to a few micrometers, or roughly from a fine sand to a very fine sand. Because they are smaller than early fallout particles, delayed fallout particles tend to contain less radioactivity. Their small size also means very little mass, causing delayed fallout particles to descend slowly, often reaching Earth at locations far from the point of the detonation. This makes delayed fallout a global concern. Particle formation The energy released during a nuclear detonation is greater than 4 billion BTU per kiloton yield. This energy elevates the temperature inside the fireball to phenomenally high levels, causing the materials trapped in the fireball to change almost instantaneously from a solid state to a plasma state. The extreme temperatures cause the fireball to rise quickly and expand, engulfing and vaporizing tiny particles suspended in the environment. As the fireball rises, a vacuum is created, resulting in a tremendous updraft. The surrounding atmosphere fills the void created by the updraft, creating afterwinds.

62
Real-World Example Similar to Russian Suitcase Nukes
Same type of nuclear warhead was used in a small artillery round, called Davy Crockett. Show slide 13 The effects from a Davy Crockett round would be expected to be similar to the effects from a backpack nuke or a terrorist-built weapon that fails to function properly. Next slide is a video of a real world example. 7 July 1962 live-fire test of the Davy Crockett small nuclear weapon. Davy Crockett video and following pictures taken from THE U.S. ARMY PRESENTS MF , IVY FLATS FILM REPORT, UNC 6/97 The yield from this device was less than one kiloton. (equivalent to less than 1,000 tons of TNT)
")
63
Davy Crockett Fallout – NYC
10,000 mrem/hr Point of Detonation FOR TRAINING PURPOSES ONLY 1,000 mrem/hr Lethal Dose Area Results from Davy Crockett overlaid on New York City map Building that houses detonation device is destroyed Adjoining buildings damaged People within 1200 feet receive lethal dose of radiation (650,000 mrem or higher) from blast (not fallout) 1~50,000 fatalities in estimation 1~200,000 casualties
 from blast (not fallout) 1~50,000 fatalities in estimation. 1~200,000 casualties.")
64
Atomic Weapon NuclideYields
Approximate Yields of the Principal Nuclides per Megaton of Fission Nuclide Half-life MCi 89Sr 90Sr 95Zr 103Ru 106Ru 131I 137Cs 131Ce 144Ce 53 d 28 y 65 d 40 d 1 y 8 d 30 y 33 d 20.0b 0.1b 25.0b 18.5b 0.29b 125.0c 0.16b 39.0b 3.7b bFrom Klement (1965) cFrom Knapp (1963) Environmental Radioactivity 4th Ed., Eisenbud M (1997)
 cFrom Knapp (1963) Environmental Radioactivity 4th Ed., Eisenbud M (1997)")
65
The Chernobyl Accident

66
Chernobyl: Healthcare Resources Used
Local medical facilities 400 special medical brigades M.D., H.P., etc. 15,000 health workers 2,000 M.D.’s, 4,000 nurses, med students, etc 213 mobile laboratories Special hospitals (Kiev, Moscow)
")
67
Chernobyl: Healthcare Procedures
Medical Examinations 1,000,000 persons Dosimetric & lab tests 700,000 (216,000 children) Inpatient care 32,000 persons (12,000 children) Iodine prophylaxis 5,400,000 persons (1,700,000 children)
 Inpatient care. 32,000 persons. (12,000 children) Iodine prophylaxis. 5,400,000 persons (1,700,000 children)")
68
Chernobyl: Aftermath 31 deaths
1 from roof collapse 1 severe burns 21 of 22 with ARS and skin burns ( r) 7 of 23 ( r) Estimate additional 300 cases of thyroid cancer in exposed children and 100 cases in exposed adults. 135,000 persons from 176 communities evacuated out to 30 km from plant Dose to public (3-15 km zone): estimate 43 rem (50 year commited dose)
 7 of 23 ( r) Estimate additional 300 cases of thyroid cancer in exposed children and 100 cases in exposed adults. 135,000 persons from 176 communities evacuated out to 30 km from plant. Dose to public (3-15 km zone): estimate 43 rem (50 year commited dose)")
69
Lessons Learned In the USSR highly organized Civil Defense, Health system, Military and other government resources were quickly mobilized. In the US less centralized resources might currently have more difficulties, although the maturation of the Homeland Security Agency should facilitate such a response.

70
Radiation Terrorism and Response
OUTLINE Radiation Terrorism and Response Radiation Basics Radiation Protection Rules Radiation Threats Nuclear device, “dirty” bomb Equivalent Experiences: Chernobyl, Goiana 4. Health Management of Affected Population

71
What Is a Radiation Threat?
A radiation threat or "Dirty Bomb" is the use of common explosives to spread radioactive materials. It is not a nuclear blast. The force of the explosion and radioactive contamination will be more localized. In order to limit the amount of radiation you are exposed to, think about shielding, distance and time. Local authorities may not be able to immediately provide information on what is happening and what you should do. However, you should watch TV, listen to the radio, or check the Internet often for official news and information as it becomes available.

72
Russian Nuclear SuitcaseDevices
84 of 132 devices are missing “We do not know what the status of the other devices is, we just could not locate them…” Russian General Lebed, 1998 “No direct evidence that any have been stolen.” US Assistant Sec of Defense of Nuclear Chemical Biological Programs, January 2003 Show slide 12 In 1998, General Lebed said one of his assignments was to account for 132 suitcase-size nuclear weapons that the Soviet Union had manufactured during the seventies and the eighties, of which he could only find 48 (84 missing). “We do not know what the status of the other devices is, we just could not locate them….” General Lebed, Former Russian National Security Advisor, later recanted this story and then reinstated it with different numbers. Currently, the actual numbers of the missing suitcase nukes are uncertain.
. We do not know what the status of the other devices is, we just could not locate them…. General Lebed, Former Russian National Security Advisor, later recanted this story and then reinstated it with different numbers. Currently, the actual numbers of the missing suitcase nukes are uncertain.")
73
Black Market Smuggling Total Number of Material Seizures (April 2001)
217 low-grade nuclear material 14 weapons usable material 299 Radioactive Sources Show slide 45 Total Number of Seizures (April 2001) by Material The Low Grade Nuclear material is uranium or plutonium that may be suitable for use in a nuclear reactor, but cannot be made into a nuclear weapon. The weapons usable material is uranium or plutonium that is the right type to be used in a nuclear bomb. Most of these seizures have been very amounts, not enough to make a nuclear bomb out of. REF: The picture shows a standard Russian radiological material container used in nuclear industries in Russia (model BGI-45A)
 by Material. The Low Grade Nuclear material is uranium or plutonium that may be suitable for use in a nuclear reactor, but cannot be. made into a nuclear weapon. The weapons usable material is uranium or plutonium that is the right type to be used in a nuclear bomb. Most of these seizures have been very amounts, not enough to make a nuclear bomb out of. REF: The picture shows a standard Russian radiological material container used in nuclear industries in Russia (model BGI-45A)")
74
Sophisticated RDD May not be recognized before it is exploded
Show slide 24 Sophisticated RDD If a more sophisticated RDD is disguised as an everyday item, the public and responders may not recognize the device as an RDD. A bomb squad or Explosive Ordinance Disposal (EOD) team may be able to recognize the radiological material inside the device. The picture shows a simulated dirty bomb assembled built by the Nevada Test Site staff from with fake explosives, real radiological material (gray cylinders), and fake industrial radiation sources.
 team may be able to recognize the radiological material inside the device. The picture shows a simulated dirty bomb assembled built by the Nevada Test Site staff from with fake explosives, real radiological material (gray cylinders), and fake industrial radiation sources.")
75
Probability of RDD Terrorist Event Radiological dispersal device (dirty bomb) Health Consequences: Injury Burns Single Nuclide Contamination(?) Much higher probability than the use of a nuclear weapon: Simple to build Widely available materials Ease of building simple explosives More than 200 naturally-occurring and man-made radionuclides can be potentially used for RDD Show slide 23 Probability of RDD An RDD may be as simple as a pipe bomb or explosives attached to a shipping container of radiological material. Because of the wide availability of radiological material throughout the world, and the ease of building simple explosives, the probability of use of an RDD is much higher than that of a nuclear weapon. The picture shows a simulated dirty bomb assembled from a fake pipe bomb and a real radiological shipping container. (Note: Radioactive Yellow II shipping label on container. The “II” (two) is hard to read in this photo, but you can see the yellow color and the radiation symbol, so you can tell it is either Rad yellow one or rad yellow two label).
 Much higher probability than the use of a nuclear weapon: Simple to build. Widely available materials. Ease of building simple explosives. More than 200 naturally-occurring and man-made radionuclides can be potentially used for RDD. Show slide 23. Probability of RDD. An RDD may be as simple as a pipe bomb or explosives attached to a shipping container of radiological material. Because of. the wide availability of radiological material throughout the world, and the ease of building simple explosives, the probability of use of an RDD is much higher than that of a nuclear weapon. The picture shows a simulated dirty bomb assembled from a fake pipe bomb and a real radiological shipping container. (Note: Radioactive Yellow II shipping label on container. The II (two) is hard to read in this photo, but you can see the yellow color and the radiation symbol, so you can tell it is either Rad yellow one or rad yellow two label).")
76
Background After the 1991 Gulf War Iraqis disclosed they had worked on an RDD made of iron bombs packed with zirconium oxide irradiated in a research reactor. (USAF SAB, 1998 and IAEA documentation) ~ 200 of the 2 million regulated radioactive sources and devices are lost, stolen, or abandoned each year in the USA. Cesium-137, the most commonly lost radiation source has a 33 year half-life emits Beta (0.510, 1.17 MeV), and Gamma (~0.662 KeV) and substitutes for Potassium in the body. Biological half-life is ~109 days for men, 84 days for women, and 57 day in kids. Cesium in atmosphere enters plants via roots and can pose threat for years.
 ~ 200 of the 2 million regulated radioactive sources and devices are lost, stolen, or abandoned each year in the USA. Cesium-137, the most commonly lost radiation source has a 33 year half-life emits Beta (0.510, 1.17 MeV), and Gamma (~0.662 KeV) and substitutes for Potassium in the body. Biological half-life is ~109 days for men, 84 days for women, and 57 day in kids. Cesium in atmosphere enters plants via roots and can pose threat for years.")
77
Radiation exposure from most RDDs in urban areas would expose many, kill few
The principal type of dirty bomb, or Radiological Dispersal Device (RDD), combines a conventional explosive, such as dynamite, with radioactive material. In most instances, the conventional explosive itself would have more immediate lethality than the radioactive material. At the levels created by most probable sources, not enough radiation would be present in a dirty bomb to kill people or cause severe illness. However, certain other radioactive materials, dispersed in the air, could contaminate up to several city blocks, creating fear and possibly panic and requiring potentially costly cleanup. Prompt, accurate, non-emotional public information might prevent the panic sought by terrorists. A second type of RDD might involve a powerful radioactive source hidden in a public place, such as a trash receptacle in a busy train or subway station, where people passing close to the source might get a significant dose of radiation. A dirty bomb is in no way similar to a nuclear weapon. The presumed purpose of its use would be therefore not as a Weapon of Mass Destruction but rather as a Weapon of Mass Disruption. Good reference:
, combines a conventional explosive, such as dynamite, with radioactive material. In most instances, the conventional explosive itself would have more immediate lethality than the radioactive material. At the levels created by most probable sources, not enough radiation would be present in a dirty bomb to kill people or cause severe illness. However, certain other radioactive materials, dispersed in the air, could contaminate up to several city blocks, creating fear and possibly panic and requiring potentially costly cleanup. Prompt, accurate, non-emotional public information might prevent the panic sought by terrorists. A second type of RDD might involve a powerful radioactive source hidden in a public place, such as a trash receptacle in a busy train or subway station, where people passing close to the source might get a significant dose of radiation. A dirty bomb is in no way similar to a nuclear weapon. The presumed purpose of its use would be therefore not as a Weapon of Mass Destruction but rather as a Weapon of Mass Disruption. Good reference:")
78
Concerns Immediate radiation injury—very few
Cancer—small (if any) increase on overall 25% probability of dying from cancer Exceptions: iodine and children’s thyroid cancer Birth defects—only a concern for a few (if any), has been dramatically overestimated in the past
 increase on overall 25% probability of dying from cancer. Exceptions: iodine and children’s thyroid cancer. Birth defects—only a concern for a few (if any), has been dramatically overestimated in the past.")
79
Goiania Contamination Accident
454-2

80
Location of Goiania, Brazil
451-1

81
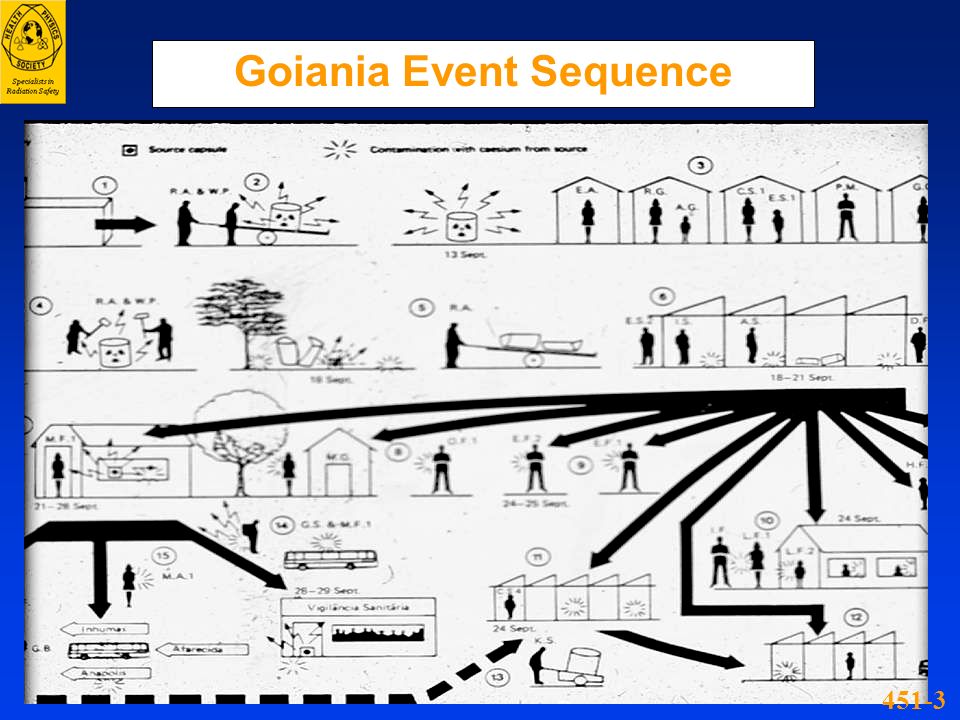
Goiania Accident Source
137Cs teletherapy source capsule: Physical form: CsCl hygroscopic powder with blue fluorescence as it absorbed moisture. Radioactivity: 50.9 TBq (1375Ci) Dose m: 4.56 Gy/hr (456 rad/hr)
 Dose m: 4.56 Gy/hr (456 rad/hr)")
82
Goiania Event Sequence
451-3
83
Goiania Medical Disposition
580-9

84
Goiania Casualty Burial

85
Goiania Local Injury 454-5

86
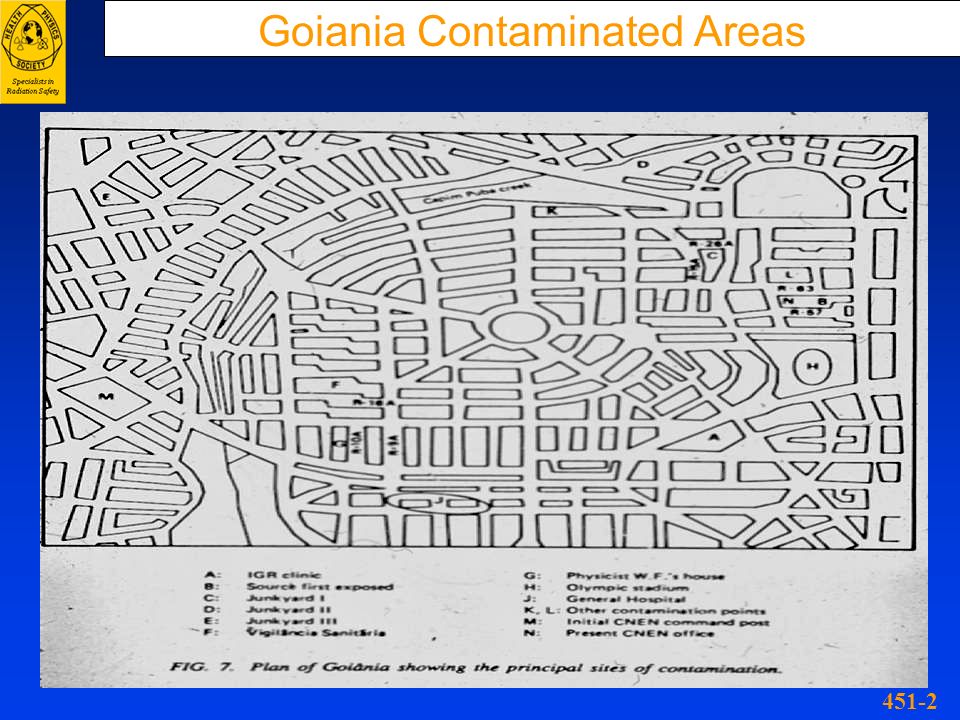
Goiania Contaminated Areas
451-2
87
Goiania Population Screening
55-3

88
Goiania Accident Magnitude
People monitored: ,000 Chromosome analyses: Roads monitored: ,000 Km Remediation workers: Above DL: (Highest: 10 mSv CDE) Homes contaminated: Demolished: Vehicles contaminated: Radwaste created: , L drums
 Homes contaminated: 85. Demolished: 7. Vehicles contaminated: 50. Radwaste created: 3, L drums.")
89
Lessons Learned Lack of awareness of the detrimental health effects of radiation exposure can impede its recognition on the part of patients and medical practitioners until much damage is done. The alert M.D. who faces an unusual public health problem must find a collaborating H.P. to evaluate its possible radiogenic origin and if confirmed, to help deal with it.

90
Shelter if you can’t evacuate
Use the Shelter to Shield and Distance yourself from the fallout contamination. Buildings Buildings provide considerable protection from fallout. A brick building provides better protection than does a brick veneer building, which is better than that of a frame building. Multiple stories increase protection as well. The interior of a one-story building reduces exposure by 50 percent. A level below ground reduces exposure by 90 percent. Additional levels provide more shielding and increase the overall effectiveness above and below ground. However, notice in the five-story example that the middle floors provide better shielding than the ground floor because fallout that covers the ground emits gamma radiation along with that on the exterior surfaces of the building. Moving to a higher floor in the building increases the distance from the ground source but, at some point, increases exposure from the source on the rooftop. The best option is to move to the center of the building away from the exterior walls and below ground, if possible, or to a middle floor above ground. In a detailed illustration of a building, note how the position in the building and surroundings affect the percentage by which exposure is reduced in various locations.

91
Particle Filtering Factors
Filtration Efficiencies Man’s cotton handkerchief, 16 thick. 94% Man’s cotton handkerchief, 8 thick. 88% Toilet paper, 3 thick. 91% Bath towel, 2 thick % Cotton Shirt, 2 thick. 65% Turn off ventilation

92
Recommended Accumulated Dose Levels at which to Consider Evacuation and/or Relocation

93
Fallout: The 7-10 Rule of Thumb
Time (hours) Relative Fallout Dose Rates H + 1* 100% H + 7 (1•7) 10 % H+49 (7•7) 1% H+343 (7•7•7) ~14 Days 0.1% H+2401 (74) ~100 Days 0.01% Shelter as long as possible before evacuating across fallout contamination. Waiting 2 days will reduce exposure by a factor of 100! Time The mixture of radionuclides in the fission products formed after a nuclear detonation is so complex that it is not possible to represent their decay in terms of a single half-life. However, it has been found that for every sevenfold increase in time after a nuclear explosion, the relative activity decreases by a factor of ten. As shown, 1 hour after detonation is used as a reference point and assigned a relative activity of 100 percent. At 7 hours after detonation, the relative activity decreases to 10 percent. If this curve were extended, it would show that, at 49 (7x7) hours after detonation, the relative activity decreases to 1 percent and that, at 2 weeks (7x7x7 hours), it is 1/10 of 1 percent. *Prior to H+1, the dose rates from fall out is significantly higher
 Relative Fallout. Dose Rates. H + 1* 100% H + 7 (1•7) 10 % H+49 (7•7) 1% H+343 (7•7•7) ~14 Days. 0.1% H+2401 (74) ~100 Days. 0.01% Shelter as long as possible before evacuating across fallout contamination. Waiting 2 days will reduce exposure by a factor of 100! Time. The mixture of radionuclides in the fission products formed after a nuclear detonation is so complex that it is not possible to represent their decay in terms of a single half-life. However, it has been found that for every sevenfold increase in time after a nuclear explosion, the relative activity decreases by a factor of ten. As shown, 1 hour after detonation is used as a reference point and assigned a relative activity of 100 percent. At 7 hours after detonation, the relative activity decreases to 10 percent. If this curve were extended, it would show that, at 49 (7x7) hours after detonation, the relative activity decreases to 1 percent and that, at 2 weeks (7x7x7 hours), it is 1/10 of 1 percent. *Prior to H+1, the dose rates from fall out is significantly higher.")
94
Decontamination: important for nuclear weapons and radiation dispersal devices

95
Evacuate the Fallout Path
Although dose rates are highest within the first few hours, this only represents a relatively small area Evacuating the fallout area before fallout arrival will save the most lives Ideal pattern The time sequence illustrated is for a 1-megaton fission yield weapon and a 15-mile-per-hour effective wind speed. The dose rates are external gamma dose rates. As shown, 20 miles downwind from the explosion at 1 hour after the detonation is a 3-rad-per-hour fallout field. The ideal fallout pattern is based on a given weapon and yield and assumes a smooth, open terrain. Using the fission yield of the weapon, an average fallout pattern is determined for a given steady state wind condition. This results in ideal isodose rates with a cigar-like shape, having ideal width and ideal distance upwind and downwind. In the example, although not illustrated, the dose rate would increase to more than 500 rads per hour between 1 and 2 hours after detonation. By 6 hours after the explosion, the dose rate would decrease to less than 100 rads per hour. The increase in dose rates after 1 hour would indicate that, at the specified location, the fallout is not yet complete. The subsequent drop after the maximum dose rate is achieved would be attributed to the natural decay of the fission products. At 18 hours after the burst, the dose rates would decrease even farther to near 30 rads per hour at 20 miles directly downwind.

96
If there is a radiation or a “dirty bomb” threat
If you are outside and there is an explosion or authorities warn of a radiation release nearby, cover your nose and mouth and quickly go inside a building that has not been damaged. If you are already inside check to see if your building has been damaged. If your building is stable, stay where you are. Close windows and doors; turn off air conditioners, heaters or other ventilation systems.

97
If there is a radiation or a “dirty bomb” threat
If you are inside and there is an explosion near where you are or you are warned of a radiation release inside, cover nose and mouth and go outside immediately. Look for a building or other shelter that has not been damaged and quickly get inside. Once you are inside, close windows and doors; turn off air conditioners, heaters or other ventilation systems. If you think you have been exposed to radiation, take off your clothes and wash as soon as possible. Stay where you are, watch TV, listen to the radio, or check the Internet for official news as it becomes available.

98
If there is a nuclear blast
If there is advance warning: Take cover immediately, as far below ground as possible, though any shield or shelter will help protect you from the immediate effects of the blast and the pressure wave. If there is no warning: Quickly assess the situation. Consider if you can get out of the area or if it would be better to go inside a building to limit the amount of radioactive material you are exposed to. If you take shelter go as far below ground as possible, close windows and doors, turn off air conditioners, heaters or other ventilation systems. Stay where you are, watch TV, listen to the radio, or check the Internet for official news as it becomes available. To limit the amount of radiation you are exposed to, think about shielding, distance and time. Use available information to assess the situation. If there is a significant radioactive contamination threat, health care authorities may advise you to take potassium iodide. It may protect your thyroid gland, which is particularly vulnerable, from radioactive iodine exposure. Plan to speak with your health care provider in advance about what makes sense for your family.

99
Conclusions Radiation dispersal devices could cause significant contamination with low levels of radiation, but would result in few if any radiation casualties. Much of the radiation dispersal device’s impact will depend on how much we over-react to the dangers of radiation. A nuclear weapon would result in substantial casualties and confusion from many effects, with radiation injury being the dominant one in the fallout region. In a fallout scenario, wise actions on sheltering/evacuation will save thousands of lives. You can prepare by knowing (and teaching) the facts about radiation, and having a plan about what to do in a radiation emergency—a good place to start is
 the facts about radiation, and having a plan about what to do in a radiation emergency—a good place to start is")
100
Radiation Terrorism and Response
OUTLINE Radiation Terrorism and Response Radiation Basics Radiation Protection Rules Radiation Threats Nuclear device, “dirty” bomb Equivalent Experiences: Chernobyl, Goiana 4. Health Management of Affected Population

101
The Real Medical Radiation Problems
Fear Communication Failure Uncertainty Inaction Chaos

102
Key Points for Emergency Responders
Lifesaving first aid is the First Priority Familiarize yourself with work area Survey instrumentation, protective clothing, respiratory protection suitable to accident conditions Evacuate personnel to safe areas Assessment of radiological hazard Public Prevention is key as therapeutic measures are limited Shelter vs Evacuation Contamination Rule of thumb: % contamination removed with clothing Showering will remove an additional 7%

103
Facility Preparation Activate hospital plan
Obtain radiation survey meters Call for additional support: Staff from Nuclear Medicine, Radiation Oncology, Radiation Safety (Health Physics) Establish area for decontamination of uninjured persons Establish triage area Plan to control contamination Instruct staff to use universal precautions and double glove Establish multiple receptacles for contaminated waste Protect floor with covering if time allows For transport of contaminated patients into ED, designate separate entrance, designate one side of corridor, or transfer to clean gurney before entering, if time allows 19. Facility Preparation The hospital should activate its radiological emergency medical response plan. A triage area should be identified for accepting patients and the worried well. The plan should address contamination control for staff and facilities. There should be a call out list to obtain additional staff and equipment. Staff protects themselves from contamination by using universal precautions and double gloving. Staff should know where to obtain radiation survey meters and personnel to operate them. Environmental Services should establish multiple receptacles for contaminated waste. Call for additional support from hospital staff: Nuclear Medicine, Radiation Oncology, Radiation Safety/ Health Physics. Plan for the decontamination of uninjured persons away from the ED. Protect the floor with covering if time allows.
 Establish area for decontamination of uninjured persons. Establish triage area. Plan to control contamination. Instruct staff to use universal precautions and double glove. Establish multiple receptacles for contaminated waste. Protect floor with covering if time allows. For transport of contaminated patients into ED, designate separate entrance, designate one side of corridor, or transfer to clean gurney before entering, if time allows. 19. Facility Preparation. The hospital should activate its radiological emergency medical response plan. A triage area should be identified for accepting patients and the worried well. The plan should address contamination control for staff and facilities. There should be a call out list to obtain additional staff and equipment. Staff protects themselves from contamination by using universal precautions and double gloving. Staff should know where to obtain radiation survey meters and personnel to operate them. Environmental Services should establish multiple receptacles for contaminated waste. Call for additional support from hospital staff: Nuclear Medicine, Radiation Oncology, Radiation Safety/ Health Physics. Plan for the decontamination of uninjured persons away from the ED. Protect the floor with covering if time allows.")
104
Decontamination Center
Establish a decontamination center for people who are contaminated, but not significantly injured. Center should provide showers for many people. Replacement clothing must be available. Provisions to transport or shelter people after decontamination may be necessary. Staff decontamination center with medical staff with a radiological background, health physicists or other staff trained in decontamination and use of radiation survey meters, and psychological counselors 17. Decontamination Center A decontamination center should be established to monitor people who may be contaminated and provide facilities for decontamination. Ideally, it should provide showers. In a crisis, hoses could be used. A decontamination center should be staffed by physicians with a radiological background, health physicists or other staff familiar with decontamination procedures and the use of radiation survey meters, and psychological counselors. Towels and replacement clothing should be available. Provisions, especially in inclement weather, may be needed to shelter people or to transport them elsewhere after decontamination.

105
Protecting Staff from Contamination
Universal precautions Survey hands and clothing with radiation meter Replace gloves or clothing that is contaminated Keep the work area free of contamination Key Points Contamination is easy to detect and most of it can be removed It is very unlikely that ED staff will receive large radiation doses from treating contaminated patients 15. Protecting Staff from Contamination Hospital staff are well versed in protecting themselves and their work areas from microbiological contamination through the use of “Universal Precautions.” The same techniques can be used effectively to protect personnel and the work area from contamination by radioactive materials. One great advantage that hospital personnel have, when it comes to radioactive contamination, is the ease with which radioactive material can be detected. Most radioactive material can be detected easily and in very small quantities with the use of a simple instrument such as a GM survey meter (Geiger counter). Frequent use of the GM survey meter can alert personnel to the need to change their gloves or clothing when they become contaminated or to tell them when contamination is being spread to the work area so that cleanup and extra precautions can be implemented. Such ease of detection and control is not possible with any other type of hazardous material. Medical personnel working on the Chernobyl site after the accident received less than 1000 mrem. (Mettler and Voelz, New England Journal of Medicine, 2002; 346: ) Emphasize the Key Points that most contamination is easy to detect and remove and it is very unlikely that ED staff will receive large radiation doses from treating contaminated patients.
. Frequent use of the GM survey meter can alert personnel to the need to change their gloves or clothing when they become contaminated or to tell them when contamination is being spread to the work area so that cleanup and extra precautions can be implemented. Such ease of detection and control is not possible with any other type of hazardous material. Medical personnel working on the Chernobyl site after the accident received less than 1000 mrem. (Mettler and Voelz, New England Journal of Medicine, 2002; 346: ) Emphasize the Key Points that most contamination is easy to detect and remove and it is very unlikely that ED staff will receive large radiation doses from treating contaminated patients.")
106
Treatment Area Layout Separate Entrance CONTAMINATED AREA Trauma Room
ED Staff Radiation Survey & Charting CONTAMINATED AREA Contaminated Waste Trauma Room HOT LINE STEP OFF PAD Radiation Survey Waste BUFFER ZONE 20. Treatment Area Layout The layout for the handling of a contaminated radiation accident victim should be established to control the spread of contamination by using universal precautions. Control of individuals and materials going into the area. Control and survey of materials and personnel coming out of the area. Use appropriate steps to prevent the spread of contamination (e.g., monitor gloves and change as necessary, monitor shoes when leaving, etc.). Monitoring of the patient and the trauma room to detect, control and remove contamination. Contaminated waste water need not be contained if it will unduly complicate the treatment of the patient or it is otherwise determined to be impractical. Release of waste water can be justified in almost all situations. Clean Gloves, Masks, Gowns, Booties CLEAN AREA
. Monitoring of the patient and the trauma room to detect, control and remove contamination. Contaminated waste water need not be contained if it will unduly complicate the treatment of the patient or it is otherwise determined to be impractical. Release of waste water can be justified in almost all situations. Clean. Gloves, Masks, Gowns, Booties. CLEAN. AREA.")
107
Detecting and Measuring Radiation
Instruments Locate contamination - GM Survey Meter (Geiger counter) Measure exposure rate - Ion Chamber Personal Dosimeters - measure doses to staff Radiation Badge - Film/TLD Self reading dosimeter (analog & digital) 21. Detecting and Measuring Radiation You cannot see, smell, taste, feel, or hear radiation, but we have very sensitive instrumentation to detect it at very low levels. Radiation monitoring instruments detect the presence of radiation. The radiation measured is usually expressed as exposure per unit time, using various units of measure, milliroentgen per hour (mR/hr) and counts per minute (CPM). Anything with “milli” in front of it is SMALL! The most commonly used instruments to detect the presence of radiation include: Geiger- Mueller Survey Meter. The Geiger-Mueller (GM) survey meter (also known as a Geiger counter) will detect low levels of gamma and most beta radiation. The instrument typically has the capability to distinguish between gamma and most beta radiation. This instrument is used to quickly determine if a person is contaminated. GM survey meters are very sensitive and other instruments may be needed to measure higher levels. Ionization Chamber Survey Meter. This device can accurately measure radiation exposure. These meters measure from low levels (mR/hr) to higher levels (many R/hr). To find the dose an individual is receiving, multiply the dose rate by the time that they are exposed. Personal Dosimeters. These devices measure the cumulative dose of radiation received by persons wearing them. Film and TLD badges must be analyzed by the company that supplies them and so the dose received is not typically known for several days. However, self reading dosimeters allow the wearer to immediately see the total dose they have received.
 Measure exposure rate - Ion Chamber. Personal Dosimeters - measure doses to staff. Radiation Badge - Film/TLD. Self reading dosimeter (analog & digital) 21. Detecting and Measuring Radiation. You cannot see, smell, taste, feel, or hear radiation, but we have very sensitive instrumentation to detect it at very low levels. Radiation monitoring instruments detect the presence of radiation. The radiation measured is usually expressed as exposure per unit time, using various units of measure, milliroentgen per hour (mR/hr) and counts per minute (CPM). Anything with milli in front of it is SMALL! The most commonly used instruments to detect the presence of radiation include: Geiger- Mueller Survey Meter. The Geiger-Mueller (GM) survey meter (also known as a Geiger counter) will detect low levels of gamma and most beta radiation. The instrument typically has the capability to distinguish between gamma and most beta radiation. This instrument is used to quickly determine if a person is contaminated. GM survey meters are very sensitive and other instruments may be needed to measure higher levels. Ionization Chamber Survey Meter. This device can accurately measure radiation exposure. These meters measure from low levels (mR/hr) to higher levels (many R/hr). To find the dose an individual is receiving, multiply the dose rate by the time that they are exposed. Personal Dosimeters. These devices measure the cumulative dose of radiation received by persons wearing them. Film and TLD badges must be analyzed by the company that supplies them and so the dose received is not typically known for several days. However, self reading dosimeters allow the wearer to immediately see the total dose they have received.")
108
Patient Management - Priorities
Triage Medical triage is the highest priority Radiation exposure and contamination are secondary considerations Degree of decontamination dictated by number of and capacity to treat other injured patients 22. Patient Management – Priorities Medical stabilization takes priority over decontamination.

109
Patient Management - Triage
Triage based on: Injuries Signs and symptoms - nausea, vomiting, fatigue, diarrhea History - Where were you when the bomb exploded? Contamination survey 23. Patient Management - Triage Resuscitation and stabilization are the primary objectives. Decontamination efforts should be secondary to patient stabilization. Severity and time of onset of nausea, vomiting, diarrhea and fatigue are noted and treated in routine clinical manner. Patient history will assist in the triage process to predict the potential extent of radiation injury. Contamination surveys are secondary to patient stabilization.

110
Classification of Medical Radiation Problems
Anxiety Acute Radiation Syndrome Local Radiation Injury External Radionuclide Contamination Local Trauma with Radionuclide Contamination Internal Radionuclide Contamination 82-A

111
Mass Casualties, Contaminated but Uninjured People, and Worried Well
An incident caused by nuclear terrorism may create large numbers of contaminated people who are not injured and worried people who may not be injured or contaminated Measures must be taken to prevent these people from overwhelming the emergency department A triage site should be established outside the ED to intercept such people and divert them to appropriate locations. Triage site should be staffed with medical staff and security personnel Precautions should be taken so that people cannot avoid the triage center and reach the ED 16. Mass Casualties, Contaminated but Uninjured People, and Worried Well A mass casualty incident resulting from nuclear terrorism is likely to generate large numbers of frightened people who may not require decontamination or trauma care. It may also generate people who are contaminated, but not injured or whose injuries do not require care in the emergency department. It is important to take measures to prevent these people from overwhelming the emergency department. A triage site should be established outside the ED. Security personnel will be needed to directed people to the triage site and prevent them avoiding the triage site and reached the emergency department.

112
Radiation Anxiety In the event of a nuclear or radiological weapon detonation, thousands of victims will be concerned about their possible exposure to ionizing radiation. Accurate knowledge of radiation dose can dramatically affect the assignment of triage category, BUT accepted methods for accurate post-exposure dosimetry take days to measure. Thus, clinical signs, symptoms and blood counts are best early indicators of radiation injury.

113
Psychological Casualties
Terrorist acts involving toxic agents (especially radiation) are perceived as very threatening Mass casualty incidents caused by nuclear terrorism will create large numbers of worried people who may not be injured or contaminated Establish a center to provide psychological support to such people Set up a center in the hospital to provide psychological support for staff 18. Psychological Casualties The hospital should plan to provide psychological support to patients and set up a center in the hospital for counseling the staff. These should be staffed by physicians with a radiological background and psychological counselors.
 are perceived as very threatening. Mass casualty incidents caused by nuclear terrorism will create large numbers of worried people who may not be injured or contaminated. Establish a center to provide psychological support to such people. Set up a center in the hospital to provide psychological support for staff. 18. Psychological Casualties. The hospital should plan to provide psychological support to patients and set up a center in the hospital for counseling the staff. These should be staffed by physicians with a radiological background and psychological counselors.")
114
Acute Radiation Syndrome
Depending on the magnitude of the exposure, the hematopoietic system, the gastrointestinal tract, the cardiovascular and central nervous systems may be involved in damage. There are three major forms (in order of severity): Hematological form Gastrointestinal form Neurovascular form
: Hematological form. Gastrointestinal form. Neurovascular form.")
115
Thoma/Wald Prognostic Categories
Group 1: 0.5 to 1.5 Gy; mostly asymptomatic with occasional minimal prodromal symptoms Group 2: 1.5 to 4 Gy; clinically manifested by transient N/V and mild hemotopoietic changes Group 3: 4 to 6 Gy; clinically manifested by severe hematopoietic changes with some GI symptoms Group 4: 6 to 14 Gy; clinically manifested by severe hematopoietic complications dominated by GI complications Group 5: >50Gy; manifested by marked early neuro-vascular changes

116
Acute Radiation Syndrome (Cont.) For Doses > 100 rem
Prodromal stage nausea, vomiting, diarrhea and fatigue higher doses produce more rapid onset and greater severity Latent period (Interval) patient appears to recover decreases with increasing dose Manifest Illness Stage Hematopoietic Gastrointestinal CNS Time of Onset 31. Acute Radiation Syndrome (Cont.) The signs and symptoms that develop in the ARS occur in four distinct phases: prodromal (initial), latent period, manifest illness stage and recovery or death. Prodromal phase. Depending on the dose of radiation, patients may experience a variety of symptoms including loss of appetite, nausea, vomiting, fatigue, and diarrhea. After extremely high radiation doses, additional symptoms such as prostration, fever, respiratory difficulties, and increased excitability may develop. Latent period. This is a transitional period in which many of the initial symptoms partially or completely resolve. It may last for a few hours or up to a few weeks depending on the radiation dose. The latent period shortens as the initial dose increases. Manifest Illness Stage. These three phases occur with increasing radiation exposure and are described on the following slides. The severity of the symptoms increases with dose, amount of the body exposed (whole body vs. partial body exposure), and the penetrating ability of the radiation. The severity is also affected by factors such as age, gender, genetics, medical conditions, etc. Severity of Effect
 patient appears to recover. decreases with increasing dose. Manifest Illness Stage. Hematopoietic. Gastrointestinal. CNS. Time of Onset. 31. Acute Radiation Syndrome (Cont.) The signs and symptoms that develop in the ARS occur in four distinct phases: prodromal (initial), latent period, manifest illness stage and recovery or death. Prodromal phase. Depending on the dose of radiation, patients may experience a variety of symptoms including loss of appetite, nausea, vomiting, fatigue, and diarrhea. After extremely high radiation doses, additional symptoms such as prostration, fever, respiratory difficulties, and increased excitability may develop. Latent period. This is a transitional period in which many of the initial symptoms partially or completely resolve. It may last for a few hours or up to a few weeks depending on the radiation dose. The latent period shortens as the initial dose increases. Manifest Illness Stage. These three phases occur with increasing radiation exposure and are described on the following slides. The severity of the symptoms increases with dose, amount of the body exposed (whole body vs. partial body exposure), and the penetrating ability of the radiation. The severity is also affected by factors such as age, gender, genetics, medical conditions, etc. Severity of Effect.")
117
Prodromal Appearance Time
39-J

118
Clinical Effects of ARS

119
Acute Local Radiation Injury
Effect Time of Appearance (days) Threshold Dose (cGy) Erythema minutes to weeks (dose dependant) at threshold 8-17 600 Epilation 17-21 300 Dry desquamation 21 Moist desquamation 14-21
 Threshold Dose (cGy) Erythema. minutes to weeks (dose dependant) at threshold Epilation. Dry desquamation. Moist desquamation")
120
Localized Radiation Effects - Organ System Threshold Effects
Skin - No visible injuries < 100 rem Main erythema, epilation >500 rem Moist desquamation >1,800 rem Ulceration/Necrosis >2,400 rem Cataracts Acute exposure >200 rem Chronic exposure >600 rem Permanent Sterility Female >250 rem Male >350 rem 35. Localized Radiation Effects - Organ System Threshold Effects Partial body radiation can cause localized effects if the dose is sufficiently high. Radiation doses to the skin can cause reddening of the skin, blistering, and ulceration. Higher doses are required for blistering and ulceration than for skin reddening. This photo is from a patient who had 3 angioplasty procedures under fluoroscopic guidance. It shows deep necrosis of the skin 22 months after an exposure of ~2000 rem. A patient may present with injuries from exposure to a lost or stolen high-activity commercial radiation source. The patient may not be aware that he or she was exposed. Such a patient may have localized burn-like skin injuries without a history of heat exposure. Epilation, a tendency to bleed, nausea and vomiting and/or other symptoms of the acute radiation syndrome may be present. Cataracts have developed in some early radiation workers who received high doses to the lens of their eyes. Loss of fertility has occurred in both males and females whose gonads were exposed to very high doses of radiation.

121
Special Considerations
High radiation dose and trauma interact synergistically to increase mortality Close wounds on patients with doses > 100 rem Wound, burn care and surgery should be done in the first 48 hours or delayed for 2 to 3 months (> 100 rem) Hours ~3 Months Emergency Surgery Hematologic Recovery No Surgery After adequate hematopoietic recovery Permitted 36. Special Considerations Patients who have suffered trauma (from an explosive or burn) combined with an acute high level exposure to penetrating radiation will have increased morbidity as compared to patients who have received the same dose of radiation without trauma. If a patient has received an acute dose greater than 100 rad, efforts must be made to close wounds, cover burns, reduce fractures, and perform surgical stabilizing and definitive treatments within the first 48 hours after injury. After 48 hours, surgical interventions should be delayed until hematopoietic recovery has occurred.
 Hours. ~3 Months. Emergency. Surgery. Hematologic Recovery. No Surgery. After adequate. hematopoietic recovery. Permitted. 36. Special Considerations. Patients who have suffered trauma (from an explosive or burn) combined with an acute high level exposure to penetrating radiation will have increased morbidity as compared to patients who have received the same dose of radiation without trauma. If a patient has received an acute dose greater than 100 rad, efforts must be made to close wounds, cover burns, reduce fractures, and perform surgical stabilizing and definitive treatments within the first 48 hours after injury. After 48 hours, surgical interventions should be delayed until hematopoietic recovery has occurred.")
122
Radiation Terrorism and Response
OUTLINE Radiation Terrorism and Response Radiation Basics Radiation Protection Rules Radiation Threats Nuclear device, “dirty” bomb Equivalent Experiences: Chernobyl, Goiana 4. Health Management of Affected Population

123
Emergency Department Management of Radiation Casualties
CAUTION 1. Emergency Department Management of Radiation Casualties This training program was prepared by the Radiological Emergency Medical Preparedness & Management Subcommittee of the Homeland Security Committee of the Health Physics Society.* Every emergency department should have a medical radiation emergency plan that will allow effective and efficient handling of potentially contaminated radiation accident victims. When such a plan exists and is tested through periodic drills, it minimizes the potential for apprehension and panic should activation of the plan ever be needed. Talking points are provided with each slide to assist the presenter in answering questions. It is not expected that all the information in the talking points must be presented during the training. Health Physics Society Version 2.5 Disclaimer: The information contained herein was current as of October 5, 2004, and is intended for educational purposes only. The authors and the Health Physics Society (HPS) do not assume any responsibility for the accuracy of the information presented herein. The authors and the HPS are not liable for any legal claims or damages that arise from acts or omissions that occur based on its use. *The Health Physics Society is a non profit scientific professional organization whose mission is to promote the practice of radiation safety. Since its formation in 1956, the Society has grown to approximately 6,000 scientists, physicians, engineers, lawyers, and other professionals representing academia, industry, government, national laboratories, the department of defense, and other organizations. Society activities include encouraging research in radiation science, developing standards, and disseminating radiation safety information. Society members are involved in understanding, evaluating, and controlling the potential risks from radiation relative to the benefits. Official position statements are prepared and adopted in accordance with standard policies and procedures of the Society. The Society may be contacted at: 1313 Dolley Madison Blvd., Suite 402, McLean, VA 22101; phone: ; FAX: ;
 do not assume any responsibility for the accuracy of the information presented herein. The authors and the HPS are not liable for any legal claims or damages that arise from acts or omissions that occur based on its use. *The Health Physics Society is a non profit scientific professional organization whose mission is to promote the practice of radiation safety. Since its formation in 1956, the Society has grown to approximately 6,000 scientists, physicians, engineers, lawyers, and other professionals representing academia, industry, government, national laboratories, the department of defense, and other organizations. Society activities include encouraging research in radiation science, developing standards, and disseminating radiation safety information. Society members are involved in understanding, evaluating, and controlling the potential risks from radiation relative to the benefits. Official position statements are prepared and adopted in accordance with standard policies and procedures of the Society. The Society may be contacted at: 1313 Dolley Madison Blvd., Suite 402, McLean, VA 22101; phone: ; FAX: ;")
124
Patient Management - Decontamination
Carefully remove and bag patient’s clothing and personal belongings (typically removes 95% of contamination) Survey patient and, if practical, collect samples Handle foreign objects with care until proven non-radioactive with survey meter Decontamination priorities: Decontaminate wounds first, then intact skin Start with highest levels of contamination Change outer gloves frequently to minimize spread of contamination 24. Patient Management – Decontamination Patient decontamination should be performed after stabilization of the patient. Removal of clothing usually occurs in the field, prior to transport to the hospital. The approach to decontamination as described in the slide will minimize contamination of and exposure to attending personnel. If internal contamination is suspected, take nasal swipes and 24 hour urine and fecal collections. Unfamiliar embedded objects in patient’s clothing or wounds may be radioactive sources. Handle with long forceps, handle only briefly, and keep distant from staff and patients until proven, with a survey meter, not to be radioactive. If radioactive objects are recovered, they should be placed in a lead container using tongs or forceps and then placed at a distance from staff and patients.
 Survey patient and, if practical, collect samples. Handle foreign objects with care until proven non-radioactive with survey meter. Decontamination priorities: Decontaminate wounds first, then intact skin. Start with highest levels of contamination. Change outer gloves frequently to minimize spread of contamination. 24. Patient Management – Decontamination. Patient decontamination should be performed after stabilization of the patient. Removal of clothing usually occurs in the field, prior to transport to the hospital. The approach to decontamination as described in the slide will minimize contamination of and exposure to attending personnel. If internal contamination is suspected, take nasal swipes and 24 hour urine and fecal collections. Unfamiliar embedded objects in patient’s clothing or wounds may be radioactive sources. Handle with long forceps, handle only briefly, and keep distant from staff and patients until proven, with a survey meter, not to be radioactive. If radioactive objects are recovered, they should be placed in a lead container using tongs or forceps and then placed at a distance from staff and patients.")
125
Patient Management - Decontamination (Cont.)
Protect non-contaminated wounds with waterproof dressings Contaminated wounds: Irrigate and gently scrub with surgical sponge Extend wound debridement for removal of contamination only in extreme cases and upon expert advice Avoid overly aggressive decontamination Change dressings frequently Decontaminate intact skin and hair by washing with soap & water Remove stubborn contamination on hair by cutting with scissors or electric clippers Promote sweating Use survey meter to monitor progress of decontamination 25. Patient Management - Decontamination (Cont.) Protection of non-contaminated wounds with waterproof dressings will minimize the potential for uptake of radioactive material. To decontaminate wounds, irrigate and gently scrub with a surgical sponge. Normal wound debridement should be performed. Excision around wounds solely to remove contamination should only be performed in extreme cases and upon the advice of radiological emergency medical experts. Many times, radioactive material will exude from wounds into gauze dressings so frequent changing of dressings may aid wound decontamination. The dressing also serves to keep the contamination in place. Remove contaminated hair if necessary, using scissors or electric clippers. To avoid cutting the skin and providing an entry for internal contamination, do not shave. Usual washing methods are effective for removal of radioactive material. Overly aggressive decontamination may abrade the skin, which would increase absorption of radioactive material, and should be avoided. Sweating can remove radioactive material from pores. Cover the area with gauze and put a glove or tape plastic over the area to promote sweating. Use a GM survey meter to monitor the effectiveness of the cleaning method.
 Protection of non-contaminated wounds with waterproof dressings will minimize the potential for uptake of radioactive material. To decontaminate wounds, irrigate and gently scrub with a surgical sponge. Normal wound debridement should be performed. Excision around wounds solely to remove contamination should only be performed in extreme cases and upon the advice of radiological emergency medical experts. Many times, radioactive material will exude from wounds into gauze dressings so frequent changing of dressings may aid wound decontamination. The dressing also serves to keep the contamination in place. Remove contaminated hair if necessary, using scissors or electric clippers. To avoid cutting the skin and providing an entry for internal contamination, do not shave. Usual washing methods are effective for removal of radioactive material. Overly aggressive decontamination may abrade the skin, which would increase absorption of radioactive material, and should be avoided. Sweating can remove radioactive material from pores. Cover the area with gauze and put a glove or tape plastic over the area to promote sweating. Use a GM survey meter to monitor the effectiveness of the cleaning method.")
126
Patient Management - Decontamination (Cont.)
Cease decontamination of skin and wounds When the area is less than twice background, or When there is no significant reduction between decon efforts, and Before intact skin becomes abraded. Contaminated thermal burns Gently rinse. Washing may increase severity of injury. Additional contamination will be removed when dressings are changed. Do not delay surgery or other necessary medical procedures or exams…residual contamination can be controlled. 26. Patient Management - Decontamination (Cont.) Cease decontamination of the skin and wounds when the area is less than twice the background reading on the survey meter or there is no significant reduction between washings. Under no circumstances should decontamination cause the skin to become abraded. Contaminated thermal burns can be gently rinsed while ensuring that there will be no further damage to the skin. Additional contamination will be removed with the exudate as dressings are changed. Do not delay surgery or other necessary medical procedures because of contaminated skin or wounds. Staff will be protected from becoming contaminated by using universal precautions. Sheets and dressings will keep contamination in place.
 Cease decontamination of the skin and wounds when the area is less than twice the background reading on the survey meter or there is no significant reduction between washings. Under no circumstances should decontamination cause the skin to become abraded. Contaminated thermal burns can be gently rinsed while ensuring that there will be no further damage to the skin. Additional contamination will be removed with the exudate as dressings are changed. Do not delay surgery or other necessary medical procedures because of contaminated skin or wounds. Staff will be protected from becoming contaminated by using universal precautions. Sheets and dressings will keep contamination in place.")
127
Initial Management of Externally Contaminated Patient
Gross Decontamination Removal of Contaminated Clothing Washing and removal of Contaminated Hair Removal of Gross Wound Contamination Intermediate Stage (at clean location,if necessary) Further Local Decontamination, Swabs of Body Orifices Supportive Measures, First Aid Final Stage Patient Discharged with Fresh Clothing More Definitive Decontamination (surgical) and Other Therapy at Dispensary or Hospital
 Further Local Decontamination, Swabs of Body Orifices. Supportive Measures, First Aid. Final Stage. Patient Discharged with Fresh Clothing. More Definitive Decontamination (surgical) and Other Therapy at Dispensary or Hospital.")
128
Handling contaminated patients

129
Patient decontamination
Monitor to determine if decontamination is needed Remove outer clothing Wash exposed skin surfaces Flush wounds with water Do not scrub or abrade skin! Low levels of contamination are not a health hazard and can be left in place if not easily removed (they will decay quickly).
.")
130
Early Treatment For Radionuclide Contaminated Wounds
Irrigate Wound Saline Water Decontaminate Skin (But Do Not Injure) Detergent Continue Wound Irrigation Until Radiation Level Is Zero or Constant Treat Wound as Usual Consider Excision of Embedded Long-Lived High- Hazard Contaminants
 Detergent. Continue Wound Irrigation Until Radiation Level Is Zero or Constant. Treat Wound as Usual. Consider Excision of Embedded Long-Lived High- Hazard Contaminants.")
131
Therapy For Isotope Decorporation
Dilution 3H: Water 32P: Phosphorus (Neutraphos) Blocking 137Cs: Prussian Blue 131I, 99Tc: KI (Lugol’s) 90Sr, 85Sr: Na-Alginate (Gaviscon), Al-Phosphate or Hydroxide Gel (Phosphajel or Amphojel)
 Blocking. 137Cs: Prussian Blue. 131I, 99Tc: KI (Lugol’s) 90Sr, 85Sr: Na-Alginate (Gaviscon), Al-Phosphate or Hydroxide Gel (Phosphajel or Amphojel)")
132
Therapy For Isotope Decorporation (cont.)
Mobilization 86Rb: Chlorthalidone (Hygroton) Chelation 252Cf, 242Cm, 241Am, 239Pu, 144Ce, Rare Earths, 143Pm, 140La, 90Y, 65Zn, 46Sc: DTPA 210Pb: EDTA, Penicilamine 210Po: Dimercaprol (BAL) 203Hg, 60Co: Penicilamine
 Chelation. 252Cf, 242Cm, 241Am, 239Pu, 144Ce, Rare Earths, 143Pm, 140La, 90Y, 65Zn, 46Sc: DTPA. 210Pb: EDTA, Penicilamine. 210Po: Dimercaprol (BAL) 203Hg, 60Co: Penicilamine.")
133
Treatment of Internal Contamination
Radionuclide-specific Most effective when administered early May need to act on preliminary information NCRP Report No. 65, Management of Persons Accidentally Contaminated with Radionuclides Radionuclide Treatment Route Cesium-137 Prussian blue Oral Iodine-125/131 Potassium iodide Oral Strontium-90 Aluminum phosphate Oral Americium-241/ Ca- and Zn-DTPA IV /or Plutonium-239/ nebulizer Cobalt-60 27. Treatment of Internal Contamination Deposition of radioactive materials in the body (i.e., internal contamination), is a time-dependent, physiological phenomenon related to both the physical and chemical natures of the contaminant. The rate of radionuclide incorporation into organs can be quite rapid. Thus, time can be critical and treatment (decorporation) urgent. Several methods of preventing incorporation (e.g., catharsis, gastric lavage) might be applicable and can be prescribed by a physician. Some of the medications or preparations used in decorporation might not be available locally and should be stocked. NCRP Report No. 65, Management of Persons Accidentally Contaminated with Radionuclides, addresses the strategies to limit the exposure from internal contamination by radioactive materials. Radiation Protection Dosimetry published a Guidebook for the Treatment of Accidental Internal Radionuclide Contamination of Workers (1992) that provides additional information on patient management. In January 2003, the Food and Drug Administration (FDA) determined that Prussian blue had been shown to be safe and effective in treating people exposed to radioactive elements such as Cesium-137. In August 2004, the FDA determined that two drugs, pentetate calcium trisodium injection (Ca-DTPA) and pentetate zinc trisodium injection (Zn-DTPA), are safe and effective for treating internal contamination with plutonium, americium, or curium. The drugs increase the rate of elimination of these radioactive materials from the body.
, is a time-dependent, physiological phenomenon related to both the physical and chemical natures of the contaminant. The rate of radionuclide incorporation into organs can be quite rapid. Thus, time can be critical and treatment (decorporation) urgent. Several methods of preventing incorporation (e.g., catharsis, gastric lavage) might be applicable and can be prescribed by a physician. Some of the medications or preparations used in decorporation might not be available locally and should be stocked. NCRP Report No. 65, Management of Persons Accidentally Contaminated with Radionuclides, addresses the strategies to limit the exposure from internal contamination by radioactive materials. Radiation Protection Dosimetry published a Guidebook for the Treatment of Accidental Internal Radionuclide Contamination of Workers (1992) that provides additional information on patient management. In January 2003, the Food and Drug Administration (FDA) determined that Prussian blue had been shown to be safe and effective in treating people exposed to radioactive elements such as Cesium-137. In August 2004, the FDA determined that two drugs, pentetate calcium trisodium injection (Ca-DTPA) and pentetate zinc trisodium injection (Zn-DTPA), are safe and effective for treating internal contamination with plutonium, americium, or curium. The drugs increase the rate of elimination of these radioactive materials from the body.")
134
Treatment of Internal Contamination: Treatment Options
Reduce G.I. Absorption Hasten Excretion Use Blocking and Diluting Agents When Appropriate Use Mobilizing Agents Use Chelating Agents If Available

135
Patient Management - Patient Transfer
Transport injured, contaminated patient into or from the ED: Clean gurney covered with sheets Lift patient onto clean gurney Wrap sheets over patient Roll gurney into ED or out of treatment room 28. Patient Management Emergency personnel at the scene will probably remove patient’s clothing which will remove a significant amount of radioactive contamination. Contamination may persist when the patient arrives at the ED. The method shown on the slide can be used to transfer a contaminated patient into the ED without spreading contamination. The patient is transferred onto the clean gurney outside the ED, the sheets are wrapped over the patient, and the gurney is rolled into the ED and to the treatment room. When the patient is ready to be moved from the ED to other areas of the hospital, the patient can be transferred to a clean gurney. The gurney can be rolled into the potentially contaminated treatment room on a clean sheet or plastic. After the patient is transferred onto the gurney they can be transported through the hospital without concern for the spread of radioactive contamination.

136
Facility Recovery Remove waste from the Emergency Department and triage area Survey facility for contamination Decontaminate as necessary Normal cleaning routines (mop, strip waxed floors) typically very effective Periodically reassess contamination levels Replace furniture, floor tiles, etc. that cannot be adequately decontaminated Decontamination Goal: Less than twice normal background…higher levels may be acceptable 29. Facility Recovery If you have in-house radiation safety staff, they will supervise decontamination efforts. Environmental Services staff should remove waste from the Emergency Department and triage area and take it to a holding place until it can be surveyed for radioactive material before disposal. A radiation survey of the facility will identify any areas that need decontamination. Normal cleaning routines are typically very effective. If there is residual contamination after normal cleaning, items such as furniture and floor tiles can be replaced. The decontamination goal is for the equipment and floors to be less than twice the normal background reading. Higher levels of fixed contamination should not deter the use of emergency facilities during periods of critical need.
 typically very effective. Periodically reassess contamination levels. Replace furniture, floor tiles, etc. that cannot be adequately decontaminated. Decontamination Goal: Less than twice normal background…higher levels may be acceptable. 29. Facility Recovery. If you have in-house radiation safety staff, they will supervise decontamination efforts. Environmental Services staff should remove waste from the Emergency Department and triage area and take it to a holding place until it can be surveyed for radioactive material before disposal. A radiation survey of the facility will identify any areas that need decontamination. Normal cleaning routines are typically very effective. If there is residual contamination after normal cleaning, items such as furniture and floor tiles can be replaced. The decontamination goal is for the equipment and floors to be less than twice the normal background reading. Higher levels of fixed contamination should not deter the use of emergency facilities during periods of critical need.")
137
Key Points Medical stabilization is the highest priority
Train/drill to ensure competence and confidence Pre-plan to ensure adequate supplies and survey instruments are available Universal precautions and decontaminating patients minimizes exposure and contamination risk Early symptoms and their intensity are an indication of the severity of the radiation injury The first 24 hours are the worst; then you will likely have many additional resources 40. Key Points Emphasize that medical stabilization of the patients is the highest priority. Patients will not succumb immediately from radiation injury. Radiation exposure and contamination are not immediately life threatening nor are contamination levels or exposure levels of significant hazard to personnel. Training and drills are the best preparation to ensure competence and confidence by the the ED and other staff identified in the Emergency Plan. Pre-plan to ensure that adequate supplies and survey instruments are available. Identify non-ED staff that can assist. Staff from Nuclear Medicine, Radiation Oncology and Radiation Safety have expertise in radiation protection practices and the use of survey meters. The staff can protect themselves from radioactive contamination by using universal precautions while treating these patients. Treating these patients is not an immediate hazard to ED staff health and the long term risks from the radiation exposure are small. Early symptoms and their intensity in patients are an indication of the severity of the radiation injury. The first 24 hours are the worst. Then you will likely have many additional resources from state and federal agencies.

138
Resources Radiation Emergency Assistance Center/ Training Site (REAC/TS) (865) Medical Radiobiology Advisory Team (MRAT) Armed Forces Radiobiology Research Institute (AFRRI) (301) Medical Management of Radiological Casualties Handbook, 2003; and Terrorism with Ionizing Radiation Pocket Guide Websites: - Response to Radiation Emergencies by the Center for Disease Control - “Disaster Preparedness for Radiology Professionals” by American College of Radiology - “Medical Treatment of Radiological Casualties” 41. Resources This is a list of resources both for developing a plan for handling radiation casualties and for use in responding to an actual event. REAC/TS and MRAT can be contacted for advice during the management of a specific event. The phone numbers listed are answered 24/7. Medical Treatment of Radiological Casualties was prepared by the Department of Homeland Security Working Group on Radiological Dispersal Device Preparedness.
 Armed Forces Radiobiology Research Institute (AFRRI) (301) Medical Management of Radiological Casualties Handbook, 2003; and Terrorism with Ionizing Radiation Pocket Guide. Websites: - Response to Radiation Emergencies by the Center for Disease Control. - Disaster Preparedness for Radiology Professionals by American College of Radiology. - Medical Treatment of Radiological Casualties 41. Resources. This is a list of resources both for developing a plan for handling radiation casualties and for use in responding to an actual event. REAC/TS and MRAT can be contacted for advice during the management of a specific event. The phone numbers listed are answered 24/7. Medical Treatment of Radiological Casualties was prepared by the Department of Homeland Security Working Group on Radiological Dispersal Device Preparedness.")
139
Resources Books: Articles:
Medical Management of Radiation Accidents; Gusev, Guskova, Mettler, 2001. Medical Effects of Ionizing Radiation; Mettler and Upton, 1995. The Medical Basis for Radiation-Accident Preparedness; REAC/TS Conference, 2002. National Council on Radiation Protection Reports No. 65 (Contaminated Patient Care) and No. 138 (Radiation Injury Care). Articles: “Major Radiation Exposure - What to Expect and How to Respond,” Mettler and Voelz, New England Journal of Medicine, 2002, 346: “Medical Management of the Acute Radiation Syndrome: Recommendations of the Strategic National Stockpile Radiation Working Group,” Waselenko, et.al., Annals of Internal Medicine, 2004, 140: Guidebook for the Treatment of Accidental Internal Radionuclide Contamination of Workers; Gerber, Thomas RG (eds), Radiation Protection Dosimetry, 1992. 42. Resources This is a list of resources both for developing a plan for handling radiation casualties and for use in responding to an actual event. It is advised that some documents be procured in advance for reference during an event. For example, NCRP Report No. 65 is an excellent resource for treatment of patients who have inhaled, ingested, or absorbed radioactive material. Radiation Protection Dosimetry published a Guidebook for the Treatment of Accidental Internal Radionuclide Contamination of Workers (1992) that provides additional information on the treatment of such patients.
 and No. 138 (Radiation Injury Care). Articles: Major Radiation Exposure - What to Expect and How to Respond, Mettler and Voelz, New England Journal of Medicine, 2002, 346: Medical Management of the Acute Radiation Syndrome: Recommendations of the Strategic National Stockpile Radiation Working Group, Waselenko, et.al., Annals of Internal Medicine, 2004, 140: Guidebook for the Treatment of Accidental Internal Radionuclide Contamination of Workers; Gerber, Thomas RG (eds), Radiation Protection Dosimetry, Resources. This is a list of resources both for developing a plan for handling radiation casualties and for use in responding to an actual event. It is advised that some documents be procured in advance for reference during an event. For example, NCRP Report No. 65 is an excellent resource for treatment of patients who have inhaled, ingested, or absorbed radioactive material. Radiation Protection Dosimetry published a Guidebook for the Treatment of Accidental Internal Radionuclide Contamination of Workers (1992) that provides additional information on the treatment of such patients.")
Similar presentations



>")















