Download presentation
Presentation is loading. Please wait.

1
WHEN BACTERIA BECOMES A PROBLEM IN A WOUND MARCUS GÜRGEN SENIOR CONSULTANT SURGEON OUTPATIENT WOUND CLINIC/DEPT. OF SURGERY SØRLANDET HOSPITAL FLEKKEFJORD / NORWAY NORDIC SCIENTIFIC SYMPOSIUM 06.10.2005

2
ØVERLI

3
INTRODUCTION 1 in 4 people with chronic wounds are receiving antibiotics at any one time and 60% have received a systemic antibiotic within the previous 6 months (Tammelin, Hambræus, Lindhom 1998) There is uncertainty associated with managing infections in a chronic wound There is an overuse of antibiotics in patients with chronic wounds Antimicrobial resistance is a common problem
 There is uncertainty associated with managing infections in a chronic wound There is an overuse of antibiotics in patients with chronic wounds Antimicrobial resistance is a common problem")
4
BACTERIA IN PRESSURE ULCERS Tammelin, Lindhom, Hambræus. Chronic ulcers and antibiotic treatment. J Wound Care 1998;7(9):35-38. Staphylococcus aureus43,4% Coagulase neg. Staph. aureus42,1% Enterococcus faecalis32,3% Enterococcus faecium2,0% β-hemol. streptococcus (c,d,f,g)6,1% Enterobacter species3,0% Proteus spp. and E.coli43,4% Pseudomonas species13,1% Others (diphteroides, α-streptococci)12,1%
: Staphylococcus aureus43,4% Coagulase neg. Staph. aureus42,1% Enterococcus faecalis32,3% Enterococcus faecium2,0% β-hemol. streptococcus (c,d,f,g)6,1% Enterobacter species3,0% Proteus spp. and E.coli43,4% Pseudomonas species13,1% Others (diphteroides, α-streptococci)12,1%.")
5
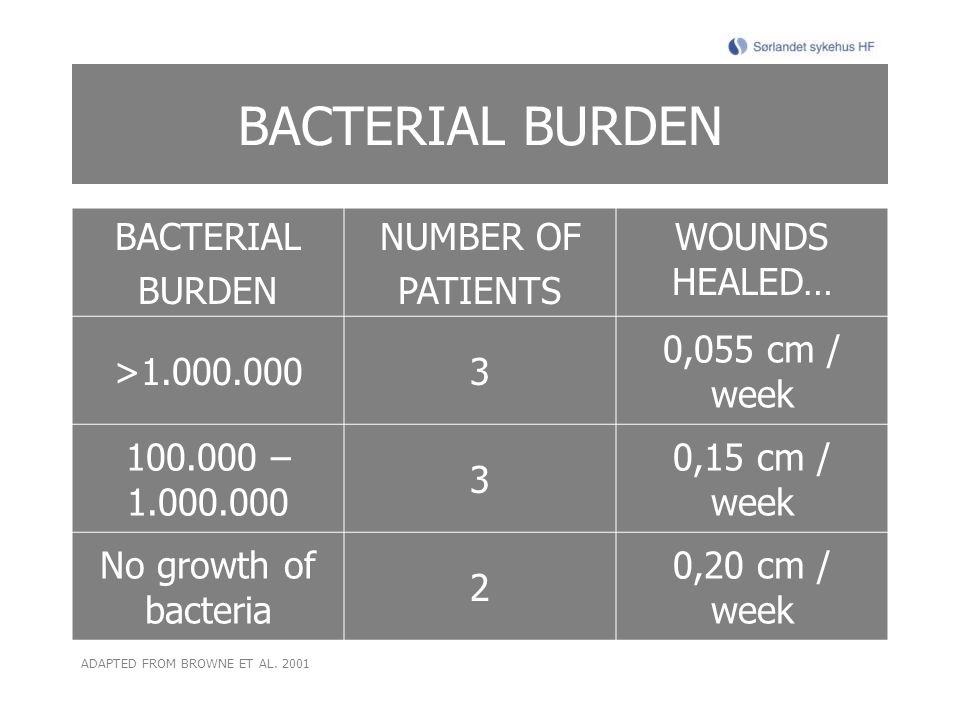
BACTERIAL BURDEN BACTERIAL BURDEN NUMBER OF PATIENTS WOUNDS HEALED… >1.000.0003 0,055 cm / week 100.000 – 1.000.000 3 0,15 cm / week No growth of bacteria 2 0,20 cm / week ADAPTED FROM BROWNE ET AL. 2001
6
CONTAMINATION BACTERIA IS FOUND IN ALL TYPES OF CHRONIC WOUNDS – NOT MULTIPLYING, NO TISSUE DAMAGE, TRANSIENT PRESENCE COLONIZATION BACTERIA ATTACHED TO TISSUE AND MULTIPLYING – DO NOT INITIATE WOUND INFECTION SYMBIOTIC RELATIONSHIPS TO HOST- ACCELERATES HEALING HEALINGHEALING BACTERIAL BALANCE INFECTION MICROBIAL GROWTH, MULTIPLICATION AND INVASION INTO HOST TISSUE - CELLULAR DAMAGE AND HOST IMMUNOLOGICAL REACTIONS CRITICAL COLONIZATION INCREASED BACTERIAL BURDEN IN THE SUPERFICIAL COMPARTMENT SUBTLE SIGNS OF INFECTION – LOCAL HOST RESPONSE? TRANSITION FROM COLONIZATION TO INFECTION OR TRANSITION TO PERSISTANCE / CHRONIC INFLAMMATION? NON-HEALINGNON-HEALING BACTERIAL IMBALANCE INFECTION = NUMBER OF ORGANISMS x VIRULENCE HOST RESISTANCE ADAPTED FROM SIBBALD 2002, BOWLER 2002, EWMA POSITION DOCUMENT 2005

7
INFECTION ”Host resistance is the single most important determinant of wound infection and must be meticulously assessed in every situation where a chronic wound fails to heal” ADAPTED FROM DOW 1999

8
” HOST RESISTANCE” FACTORS RESPONSIBLE FOR RISK OF INFECTION LOCAL FACTORS Wound size Wound age Wound localization Impaired blod flow / pressure Necrosis Excessive moisture Edema Foreign bodies Inciting event SYSTEMIC FACTORS Metabolic disease Systemic disease Chronic disease Old age Malnutrition Alcohol- / drug abuse Steroids / hormones / vitamine-K-antagonist Use of antibiotics without indication

9
INFECTION IN CHRONIC WOUNDS

10
IDENTIFYING INFECTION ”Infection” is a clinical diagnosis Traditional signs of infection Abscess (swelling) Cellulitis (local redness and warmth) Discharge (serous + inflammation, sero-/ hemopurulent, pus)
 Cellulitis (local redness and warmth) Discharge (serous + inflammation, sero-/ hemopurulent, pus)")
11
WOUND INFECTION INCREASE IN MOISTURE VOLUME INCREASE IN MOISTURE VOLUME POCKETING FRIABLE GRANULATION TISSUE FRIABLE GRANULATION TISSUE MALODOUR INCREASE IN PAIN INCREASE IN PAIN FORMATION OF NECROSIS FORMATION OF NECROSIS NON-HEALING WOUND ENLARGING WOUND ENLARGING DISCOLOURATION OTHER CRITERIA

12
A DELPHI APPROACH Cutting KF, White RJ, Mahoney P, Harding KG. Clinical identification of wound infection: a Delphi approach. European Wound Management Association (EWMA). Position Document: Identifying criteria for wound infection. London: MEP Ltd, 2005: 6-9. Cellulitis Delayed healing despite appropriate compression therapy Increase in local skin temperature Increase in ulcer pain / change in nature of pain Newly formed ulcers within inflamed margins of pre-existing ulcers Wound bed extension within inflamed margins EG VENOUS ULCERS Discolouration eg dull, dark brick red Friable granulation tissue Increase in wound viscosity Increase in exudate volume Malodour Sudden increase in amount of slough Sudden appearance of necrotic black spots Ulcer enlargement KEY HIGH mean score 8 or 9 MEDIUM mean score 6 or 7 LOWmean score 4 or 5 EG DIABETIC ULCERS Cellulitis Lymphangitis Phlegmon Purulent exudate Pus / absess Crepitus in the joint Erythema Fluctuation Increase in exudate volume Induration Localised pain in a normally asensate foot Malodour Probes to bone Unexpected pain / tenderness Blue-black discolouration and haemorrhage Bone or tendon exposed Delayed / arrested wound healing despite offloading and debridement Deterioration of the wound Friable granulation tissue Local edema Sinuses developing Spreading necrosis / gangrene Colour change to yellow or gray
. Position Document: Identifying criteria for wound infection. London: MEP Ltd, 2005: 6-9. Cellulitis Delayed healing despite appropriate compression therapy Increase in local skin temperature Increase in ulcer pain / change in nature of pain Newly formed ulcers within inflamed margins of pre-existing ulcers Wound bed extension within inflamed margins EG VENOUS ULCERS Discolouration eg dull, dark brick red Friable granulation tissue Increase in wound viscosity Increase in exudate volume Malodour Sudden increase in amount of slough Sudden appearance of necrotic black spots Ulcer enlargement KEY HIGH mean score 8 or 9 MEDIUM mean score 6 or 7 LOWmean score 4 or 5 EG DIABETIC ULCERS Cellulitis Lymphangitis Phlegmon Purulent exudate Pus / absess Crepitus in the joint Erythema Fluctuation Increase in exudate volume Induration Localised pain in a normally asensate foot Malodour Probes to bone Unexpected pain / tenderness Blue-black discolouration and haemorrhage Bone or tendon exposed Delayed / arrested wound healing despite offloading and debridement Deterioration of the wound Friable granulation tissue Local edema Sinuses developing Spreading necrosis / gangrene Colour change to yellow or gray.")
13
LABORATORY TESTS Swabs Clean wound for debris (irrigation) and necrosis Collect material from the center of the wound, best from the border between healthy and infected tissue (not the edges!) Take biopsies in case of exposed / infected bone Choice of antibiotic after testing No need to take swabs from all chronic wounds! Blood tests CRP WBC Blood sedimentation Radiologic In case of osteomyelitis SUPPORT CLINICAL DIAGNOSIS

14
TREATING INFECTION IDENTIFY UNDERLYING HOST FACTORS CORRECT UNDERLYING HOST FACTORS DEBRIDEMENT WOUND CLEANSING CONSIDER SPECIFIC ANTIMICROBIAL THERAPY OBSERVE AND ADJUST THERAPY IF NECESSARY MOISTURE CONTROL

15
TREATING INFECTION UNDERLYING CAUSES LOCAL FACTORS Wound size Wound age Wound localization Impaired blood flow / pressure Necrosis Excessive moisture Edema Foreign bodies Inciting event SYSTEMIC FACTORS Metabolic disease Systemic disease Chronic disease Old age Malnutrition Alcohol- / drug abuse Steroids / hormones / vitamine-K-antagonist Use of antibiotics without indication

16
TREATING INFECTION DEBRIDEMENT Debridement Reduces bacterial burden Important: continuity Method of debridement must meet patient-related criteria

17
TREATING INFECTION WOUND CLEANSING Wound cleansing can in most cases be done with water from the spring (irrigation) Antiseptics are generally cytotoxic If use of antiseptics is considered one must remember that wounds are most vulnerable for cytotoxic substances in the inflammatory phase of wound healing Can be used in case of MRSA, stimulation of non- healing wounds, wounds with increased bacterial burden or infected wounds (Schultz, Sibbald, Falanga 2003) I do not recommend this because we have better tools to treat these types of wounds
 Antiseptics are generally cytotoxic If use of antiseptics is considered one must remember that wounds are most vulnerable for cytotoxic substances in the inflammatory phase of wound healing Can be used in case of MRSA, stimulation of non- healing wounds, wounds with increased bacterial burden or infected wounds (Schultz, Sibbald, Falanga 2003) I do not recommend this because we have better tools to treat these types of wounds")
18
TREATING INFECTION MOISTURE CONTROL Moisture-absorbing products Compression Topical negative pressure Elevation

19
TREATING INFECTION ANTIMICROBIAL THERAPY SUPERFICIAL LOCAL THERAPY WITH SILVER OR IODINE DEEP SYSTEMIC THERAPY Non-healing Increase in exudate volume Friable granulation tissue Discolouration New areas of slough Malodour Local warmth Pain Cellulitis > 2 cm Exposed bone Necrosis spreading Streptococcus gr. A ADAPTED FROM SIBBALD 2003

20
TREATING INFECTION SUPERFICIAL COMPARTMENT Use of local antibiotics is not recommended because of: Common allergens Breed resistance Lack of therapeutic amount of antibiotic substances No moisture balance properties Lack of autolytic debridement Cadexomer with iodine: Starch molecules provide absorption capacity Slow release of iodine which in other forms would be cytotoxic Autolytic debridement modality Not available in all countries

21
TREATING INFECTION SUPERFICIAL COMPARTMENT Silver: Silver has antimicrobial properties, nanocrystalline silver kills more than 150 different types of bacteria / fungi, and MRSA Kills microbes at the infection site by blocking transport mechanisms in bacteria, impairing bacterias cell replication and by damaging structural and receptor functions in bacteria Has antiinflammatory capability Allergy to silver is rare No resistance if concentration of silver > 30- 40 ppm Bonded to several dressing materials fitting different types of wounds in different phases of wound healing Safe Up to 7 days wear-time Cost-effective

22
TREATING INFECTION SUPERFICIAL COMPARTMENT Protease-modulating matrix One product binds harmful MMP to cellulose and thus protects GF Another product replaces damaged ECM proteins Promising study results Expensive products

23
TREATING INFECTION SUPERFICIAL COMPARTMENT pH-modulating matrix Chronic wounds have higher pH (alkaline) Weakly acidic environment promotes wound healing Proteases levels are high in chronic wound Proteases activity can be lowered by reducing wound pH to around 5 pH DEPENDANT ENZYME ACTIVITY LEVELS OF PROTEASES IN WOUNDS Schultz G, Mozingo D, Romanelli M, Claxton K. Wound healing and TIME; new concepts and scientific applications. Wound Rep Regen 2005;13(4): S1-11
: S1-11.")
24
TREATING INFECTION DEEP COMPARTMENT PRESENTATIONSEVERITYORGANISMSROUTEDURATION WOUND < 4 WEEKS, SUPERFICIAL, NO SYSTEMIC RESPONSE, OUTPATIENT MILDS. AUREUS, STREPTOCOCCUS SP. PER OS10-14 DAYS WOUND < 4 WEEKS, SUPERFICIAL, EXTENSIVE CELLULITIS + SYST. RESPONSE, NO OSTEOMYELITIS, INPATIENT SEVERES. AUREUS, STREPTOCOCCUS SP. I.V., PER OS IF CELLULITIS RESOLVING AND AFEBRILE 14 DAYS TOTAL WOUND > 4 WEEKS, DEEP TISSUE INFECTION, NO SYSTEMIC RESPONSE, OUTPATIENT MILD TO MODERATE S. AUREUS, STREPTOCOCCUS SP., COLIFORMS, ANAEROBES,+ PSEUDOMONAS PER OS2-12 WEEKS (12 WEEKS IF OSTEOMYELITIS) WOUND > 4 WEEKS, DEEP TISSUE INFECTION, SYSTEMIC RESPONSE, LIMB OR LIFE-THREATENING, INPATIENT SEVERES. AUREUS, STREPTOCOCCUS SP., COLIFORMS, ANAEROBES,+ PSEUDOMONAS I.V.14 DAYS I.V. ADAPTED FROM DOW 2001
 WOUND > 4 WEEKS, DEEP TISSUE INFECTION, SYSTEMIC RESPONSE, LIMB OR LIFE-THREATENING, INPATIENT SEVERES. AUREUS, STREPTOCOCCUS SP., COLIFORMS, ANAEROBES,+ PSEUDOMONAS I.V.14 DAYS I.V. ADAPTED FROM DOW")
25
TREATING INFECTION DEEP COMPARTMENT TYPE OF INFECTIONRECOMMENDED ANTIBIOTIC ALTERNATIVE ERYSIPELASPENICILLIN CLINDAMYCIN CEPHALEXIN PHLEGMONOUS INFECTION, ABSCESS PENICILLIN CLINDAMYCIN CEPHALEXIN MOIST GANGRENE PENICILLIN + METRONIDAZOLE ENTEROCOCCUSAMPICILLIN GRAM-NEGATIVE / PSEUDOMONAS SP. CIPROFLOXACIN GANGRENE + SYSTEMIC RESPONSE CEPHALEXIN + METRONIDAZOLE CLINDAMYCIN + CIPROFLOXACIN OSTEOMYELITISDICLOXACILLIN CEPHALOTIN CLINDAMYCIN

26
SUMMARY Bacteria in all chronic wounds Host resistance is the most important factor which determines whether there will be infection or not To diagnose infection is a clinical skill Superficial / deep compartment = different treatment strategies Remember other Wound Bed Preparation measures to reduce both bacterial and cellular burden

27
THANK YOU! ØVERLI

28
NIFS-SEMINAR 2006 TOPIC: ”If wounds are not healing” WHERE: SAS Radisson Hotel, Tromsø / Norway WHEN: February 2nd and 3rd, 2006 INFORMATION: Guro Vaagbø, Seksjon for hyperbar medisin, Haukeland Universitetssykehus, N-5021 Bergen; http://www.nifs-saar.no

Similar presentations






, However it is often misdiagnosed and mistreated.>")












