Download presentation
Presentation is loading. Please wait.

1
Chapter 12 Cardiac Disorders

2
Cardiovascular System
Heart fully functioning by 8th week of gestation Fetal circulation: placenta is the organ of oxygenation Ductus venosus Ductus arteriosus Foramen ovale The birthing process begins closure of fetal shunts Heart defects are the most common birth defect Leading cause of birth defect-related deaths The heart is a vital organ; parents confronted with a child’s cardiac problems are overwhelmed with fear and anxiety.

3
Congenital Heart Disease
Description A defect in the structure of the heart or in one or more of the large blood vessels that lead to and from the heart Multifactorial Result of genetic-environmental interactions Four classifications Based on defect’s effect on blood flow Hemodynamics: study of blood circulation Shunting: flow of blood through abnormal openings Defects with increased pulmonary blood flow Obstructive defects Defects with decreased pulmonary blood flow Mixed defects The rate of incidence of infants born with a congenital heart defect is about one per 125 to 150 deliveries. Genetic factors: History of CHD, chromosomal abnormalities Environmental factors: Alcoholism, cocaine, rubella, exposure to Coxsackie virus, diabetes mellitus, ingestion of lithium salts, Accutane, advanced maternal age

5
Congenital Heart Disease (CHD)
Diagnostic tools Not all testing is necessary for each child Lab tests, electrocardiogram, halter monitor, event recorder, chest radiography, echocardiogram, MRI, cardiac catherization Cardiac catherization is an invasive procedure Provides information about anatomy, cardiac pressure, oxygen saturation, cardiac function Sedation is necessary Entry site kept straight 4-6 hours after procedure

6
Congenital Heart Disease (CHD)
Signs and symptoms Depend on location and type of heart defect Child may be small for age, condition may be classified as a physiologic failure to thrive Exercise intolerance noticed anywhere from infancy to toddler age Clubbing of the fingers Frequent respiratory infections because of pulmonary vascular congestion Squatting position (TET spell) Polycythemia: Body compensates for hypoxemia by increasing number of RBCs Why do some children with CHD frequently assume a squatting position?
 Polycythemia: Body compensates for hypoxemia by increasing number of RBCs. Why do some children with CHD frequently assume a squatting position")
7
Clubbed fingers

8
Congestive Heart Failure (CHF)
Early symptoms Lack of infant weight gain Progressive symptoms Difficulty feeding/ sucking due to air hunger Periorbital/facial edema Vein distention Infant irritability and fatigue Hepatomegaly Splenomegaly Tachycardia/tachypnea Decreased urine output Increased work of breathing Diaphoresis Mottling Cyanosis Pallor CHF is not a disease, but rather symptoms caused by an underlying heart defect.

9
Defects with Increased Pulmonary Blood Flow
Patent ductus arteriosus (PDA) Passageway connecting pulmonary artery to aorta, avoiding fetal lungs Failure to close causes oxygenated blood to recycle through the lungs Overburdens pulmonary circulation Makes heart work harder One of the most common cardiac anomalies Symptoms Machine-like murmur, dyspnea, bounding pulses on exertion, failure to thrive, frequent respiratory infections Treatment Indomethacin/ibuprofen in premature infants to close ductus Amplatzer PDA device Surgical repair Symptoms of patent ductus arteriosus may go unnoticed during infancy. PDA occurs twice as frequently in females. Excellent prognosis for corrected PDA.
 Passageway connecting pulmonary artery to aorta, avoiding fetal lungs. Failure to close causes oxygenated blood to recycle through the lungs. Overburdens pulmonary circulation. Makes heart work harder. One of the most common cardiac anomalies. Symptoms. Machine-like murmur, dyspnea, bounding pulses on exertion, failure to thrive, frequent respiratory infections. Treatment. Indomethacin/ibuprofen in premature infants to close ductus. Amplatzer PDA device. Surgical repair. Symptoms of patent ductus arteriosus may go unnoticed during infancy. PDA occurs twice as frequently in females. Excellent prognosis for corrected PDA.")
10
Defects with Increased Pulmonary Blood Flow
Atrial septal defect (ASD) Abnormal opening between right and left atria Common congenital heart anomaly Symptoms Generally asymptomatic Cyanosis if blood flow is reversed by heart failure Large openings may cause failure to thrive Treatment Open heart surgery Percutaneous occluding devices ASD more common in females. Both surgical and nonsurgical procedures have good results.
 Abnormal opening between right and left atria. Common congenital heart anomaly. Symptoms. Generally asymptomatic. Cyanosis if blood flow is reversed by heart failure. Large openings may cause failure to thrive. Treatment. Open heart surgery. Percutaneous occluding devices. ASD more common in females. Both surgical and nonsurgical procedures have good results.")
11
Defects with Increased Pulmonary Blood Flow
Ventricular septal defect (VSD) Opening between right and left ventricles 75% of small VSDs close spontaneously by age 10 Symptoms Loud, harsh murmur Systolic tremor Moderate/large defects may present CHF symptoms Treatment Percutaneous transcatheter closure Occluder devices
 Opening between right and left ventricles. 75% of small VSDs close spontaneously by age 10. Symptoms. Loud, harsh murmur. Systolic tremor. Moderate/large defects may present CHF symptoms. Treatment. Percutaneous transcatheter closure. Occluder devices.")
12
Obstructive Defect Coarctation (tightening) of the aorta Symptoms
Increased pressure proximal to the defect Decreased pressure distal to the defect High blood pressure CHF symptoms Treatment Balloon angioplasty Surgical intervention; anastomosis Risk of developing subacute bacterial endocarditis High risk of recurrence for repairs done in infancy.

13
Defect with Decreased Pulmonary Blood Flow
Tetralogy of Fallot The most common cyanotic heart defect Four defects Stenosis (narrowing of pulmonary artery) Hypertrophy of the right ventricle Over-riding aorta VSD Symptoms Cyanosis/hypoxemia episodes with hyperpnea, irritability Hypoxia Treatment Open heart surgery to correct defects Hypoxia triggered when there is an acute demand for oxygen; i.e., during blood draw, defecation, feeding, crying. How should spells of hypoxia be handled? What is given to stop hyperpnea?
 Hypertrophy of the right ventricle. Over-riding aorta. VSD. Symptoms. Cyanosis/hypoxemia episodes with hyperpnea, irritability. Hypoxia. Treatment. Open heart surgery to correct defects. Hypoxia triggered when there is an acute demand for oxygen; i.e., during blood draw, defecation, feeding, crying. How should spells of hypoxia be handled What is given to stop hyperpnea")
14
Mixed Defect Transposition of the great arteries (TGA)
Pulmonary artery leaves left ventricle Aorta leaves the right ventricle Other defects (septal defects, PDA) must be present to exchange blood which sustains life Survival impossible without surgery Symptoms CHF symptoms Any murmur present is caused by other defects, not TGA Treatment Prostaglandin E1 (keeps PDA open) Balloon atrial septotomy (opens septal wall) Corrective surgery Performed within the first 2 weeks of life Prostaglandin E1 and balloon atrial septostomy are used as palliative measures until corrective surgery. Surgery involves switching the arteries. Antibiotic prophylaxis is done for the first 6 months.
 must be present to exchange blood which sustains life. Survival impossible without surgery. Symptoms. CHF symptoms. Any murmur present is caused by other defects, not TGA. Treatment. Prostaglandin E1 (keeps PDA open) Balloon atrial septotomy (opens septal wall) Corrective surgery. Performed within the first 2 weeks of life. Prostaglandin E1 and balloon atrial septostomy are used as palliative measures until corrective surgery. Surgery involves switching the arteries. Antibiotic prophylaxis is done for the first 6 months.")
15
Mixed Defect Hypoplastic left heart syndrome (HLHS)
Left side of the heart is underdeveloped Hypoplasia of aorta, left ventricle, mitral valve Systemic circulation provided by right side of the heart (Rt ventricle is force of circulation) Ductus arteriosus and foramen ovale must remain patent to survive with HLHS Treatment PGE1 is administered to maintain a PDA Surgery in several stages Norwood, Glenn, Fontan Transplants have been successful, but donor availability, organ rejection, infection, and immunosuppression are complicating factors.
 Ductus arteriosus and foramen ovale must remain patent to survive with HLHS. Treatment. PGE1 is administered to maintain a PDA. Surgery in several stages. Norwood, Glenn, Fontan. Transplants have been successful, but donor availability, organ rejection, infection, and immunosuppression are complicating factors.")
16
Congenital Heart Disease
Treatment and nursing care Nursing goals in the care of the newborn infant can be adapted for all children with heart defects Reduce the work of the heart Improve respiration Maintain proper nutrition Prevent infection Reduce the anxiety of the patient Support and instruct the parents Why is Lanoxin the preferred oral digitalis preparation for children with CHD? The parents of the child need support and understanding over a long period. Why is cerebral thrombosis a concern?

17
Congenital Heart Disease
Treatment and nursing care (continued) Change child’s position frequently to prevent respiratory complications Threat of cerebral thrombosis Chest tubes may be used after surgery System must be airtight Drainage containers always kept below the level of the chest Avoid unnecessarily disturbing the child; they need to conserve energy Common medications Digoxin (Lanoxin) Dopamine, dobutamine, epinephrine Amrinone, milrinone ACE inhibitors Angiotensin II receptor blockers Diuretics How should the nurse measure pulse before medicating with Lanoxin?
 Change child’s position frequently to prevent respiratory complications. Threat of cerebral thrombosis. Chest tubes may be used after surgery. System must be airtight. Drainage containers always kept below the level of the chest. Avoid unnecessarily disturbing the child; they need to conserve energy. Common medications. Digoxin (Lanoxin) Dopamine, dobutamine, epinephrine. Amrinone, milrinone. ACE inhibitors. Angiotensin II receptor blockers. Diuretics. How should the nurse measure pulse before medicating with Lanoxin")
18
Congenital Heart Disease
Treatment and nursing care (continued) Infective endocarditis (IE) High risk for children with complex cyanotic heart diseases or children who have had heart surgery Organisms grow on the endocardium or areas of turbulent blood flow Symptoms Fever, fatigue, headache, nausea, vomiting Diagnosis and treatment Blood cultures determine causative organism Antibiotics
 Infective endocarditis (IE) High risk for children with complex cyanotic heart diseases or children who have had heart surgery. Organisms grow on the endocardium or areas of turbulent blood flow. Symptoms. Fever, fatigue, headache, nausea, vomiting. Diagnosis and treatment. Blood cultures determine causative organism. Antibiotics.")
19
Congenital Heart Disease
Home care Family must understand medication administration Family must identify symptoms requiring medical attention Provide a normal environment within child’s limits Avoid allowing the child to gain control of the home Limit setting Integrate the child into family life Explain the possible need for frequent hospitalization to parents and child Avoid rough play for ~6 weeks. All day attendance in school may be too tiring for some conditions.

20
Question 12.2 Which of the following is NOT one of the four classifications of congenital heart disease? Defects with increased pulmonary blood flow Congestive heart failure Defects with decreased pulmonary blood flow Mixed defects Answer: B

21
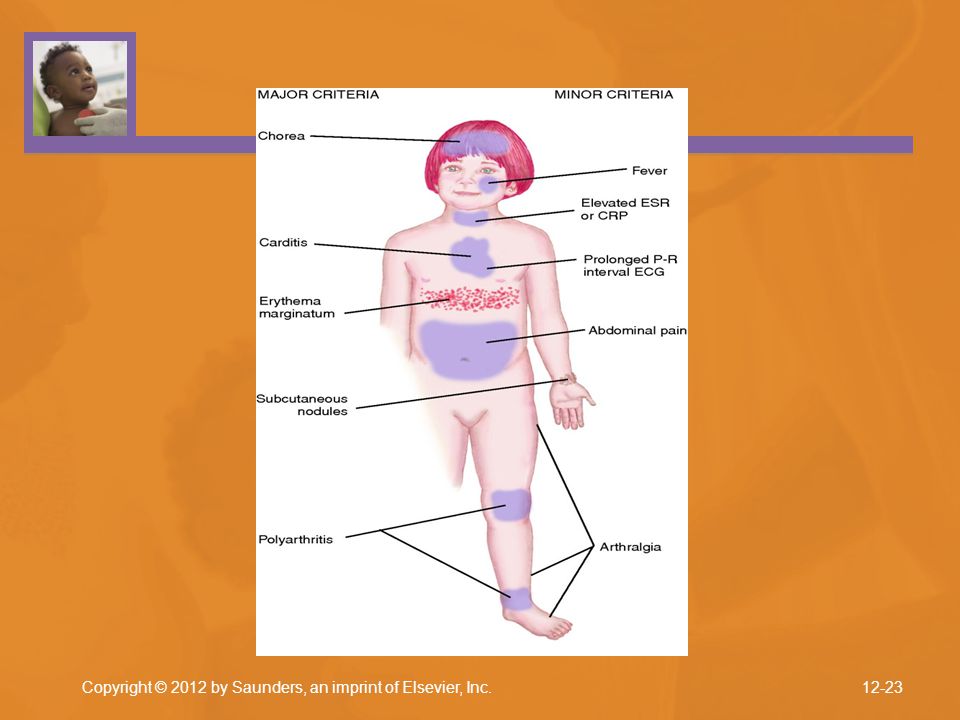
Acute Rheumatic Fever Description Signs and symptoms
Follows infection with certain strains of Group A beta-hemolytic streptococci Signs and symptoms Abdominal pain, fever, pallor, fatigue, anorexia, unexplained nosebleeds Jones criteria aid in diagnosis of rheumatic fever ECG is sometimes a useful diagnostic When does rheumatic fever typically occur? Rheumatic fever has a tendency to recur, and each attack carries the threat of further damage to the heart. Signs and symptoms of rheumatic fever: Range from mild to severe May not occur for several weeks after a streptococcal infection

24
Acute Rheumatic Fever Treatment and nursing care
Elimination of the initial infection is followed by long-term chemo-prophylaxis (prevention of disease by drugs) Intramuscular penicillin G benzathine (Bicillin), given as an intramuscular injection every 28 days Anti-inflammatory drugs are used to decrease pain and inflammation
 Intramuscular penicillin G benzathine (Bicillin), given as an intramuscular injection every 28 days. Anti-inflammatory drugs are used to decrease pain and inflammation.")
25
Acute Rheumatic Fever Home care
Bed rest during the initial attack is not necessary but is recommended if carditis is present Nurse must verify that parent and child understand activity limitations Parents should provide interesting quiet activities Long-term chemo-prophylaxis

26
Acute Rheumatic Fever Prevention
The nurse is involved in prevention of rheumatic fever in the community by recognizing signs and symptoms of streptococcal infections, doing screening, and referring for treatment

Similar presentations