Download presentation
Presentation is loading. Please wait.

1
Incorporating HIV Prevention into the Medical Care of Persons Living with HIV Ask ∙ Screen ∙ Intervene Developed by: The National Network of STD/HIV Prevention Training Centers, in conjunction with the AIDS Education Training Centers Module 4: Partner Counseling & Referral Services (PCRS)
")
2
Quick Poll What comes to mind when you hear the term partner notification?

3
Recommendations for HIV PCRS At the initial visit, ask patients if all of their sex and needle-sharing partners have been informed of their exposure to HIV At routine follow-up visits, ask patients about new sex or needle-sharing partners who have not been informed of their exposure to HIV

4
All patients should be referred to the appropriate health department to discuss partners who have not been informed of their exposure and to arrange for their notification and referral for HIV testing. In HIV health-care settings, access to available community partner counseling and referral resources should be established Recommendations for HIV PCRS

5
Upon completion of training, providers who care for HIV-infected persons will be able to: Define Partner Counseling and Referral Services (PCRS). Explain the importance of PCRS in relation to HIV. Initiate discussion of the 4 partner referral options. Learning Objectives: Module 4

6
Breaking the Chain of Infection Make no assumptions Maintain tact and respect Use open-ended questions Ask specific questions Identify and correct misconceptions Tailor the intervention Clinical Management Partner Services Behavioral Counseling Routinely integrate into clinical encounters

7
Upon completion of training, providers who care for HIV- infected persons will be able to: Define Partner Counseling and Referral Services (PCRS). Explain the importance of PCRS in relation to HIV. Initiate discussion of the four partner referral options. Learning Objectives: Module 4

8
What is HIV Partner Counseling and Referral Services (PCRS) ? HIV Partner Counseling and Referral Service: Is a voluntary and confidential service Assists persons living with HIV to tell their partner(s) about possible exposure Facilitates linkages to services. Is not widely available in Pacific jurisdictions
 about possible exposure Facilitates linkages to services. Is not widely available in Pacific jurisdictions.")
9
Upon completion of training, providers who care for HIV- infected persons will be able to: Define Partner Counseling and Referral Services (PCRS). Explain the importance of PCRS in relation to HIV. Initiate discussion of the four partner referral options. Learning Objectives: Module 4

10
Rationale for HIV PCRS HIV PCRS provides an opportunity to: Interrupt disease transmission and prevent complications Provide counseling and education for reducing behavioral risks that increase the risk of STD/HIV transmission Provide access to testing and other prevention services

11
Partner Counseling, Testing, and Referral in Ten States* with Highest Reported HIV/AIDS Cases in 2002 14,042 partners elicited through PCRS 14,042 partners elicited through PCRS 52 % (of those partners not previously known to be HIV+) were tested 18% of those were newly-identified HIV+ *California, Florida, Illinois, Louisiana, New York, New Jersey, North Carolina, Pennsylvania, Texas, Virginia
 were tested 18% of those were newly-identified HIV+ *California, Florida, Illinois, Louisiana, New York, New Jersey, North Carolina, Pennsylvania, Texas, Virginia")
12
Patient may not have to reveal HIV/STD status Fulfills ethical desires for patient Partner learns information about real risk Intervenes in spread to other partner(s) or unborn children Threat to confidentiality Potential for violence, especially against women, when HIV+ serostatus is revealed Stigma-related discrimination Common Concerns Key Benefits to Patients and Partners
 or unborn children Threat to confidentiality Potential for violence, especially against women, when HIV+ serostatus is revealed Stigma-related discrimination Common Concerns Key Benefits to Patients and Partners")
13
Fulfills public health and ethical concerns Can be performed by non-clinical staff Threat to confidentiality Increased work load in a time-limited environment Unclear legal expectations Key Benefits to Clinicians Common Concerns

14
Federal Regulations: Ryan White CARE Reauthorization Act Requires that health departments receiving Ryan White funds show “good faith” efforts to notify marriage partners of infected patients.

15
“Real Life” Scenario Tapu is a 35 y.o. married man with four children Travels often for business, away for several weeks at a time Frequently has sex with “massage parlor women” on Guam, and has several other occasional female partners on other islands; inconsistent condom use Returns from a trip with mild penile irritation, comes into the clinic to be checked out No abnormalities noted on exam; GC culture, syphilis test and HIV sent

16
“Real Life” Scenario Follow-up: GC culture negative, syphilis negative, but HIV positive! Instructed to not have sex with his wife, or to use condoms with her, until confirmatory test comes back Two weeks later, confirmatory test comes back positive; Tapu has had sex with his wife several times without a condom

17
“Real Life” Scenario What are your legal obligations in informing the partners? How would you talk to Tapu about informing his wife? How would you handle informing the occasional partners on the other islands? What if Tapu refuses to inform his partners?

18
Upon completion of training, providers who care for HIV- infected persons will be able to: Define Partner Counseling and Referral Services (PCRS). Explain the importance of PCRS in relation to HIV. Initiate discussion of the four partner referral options. Learning Objectives: Module 4

19
“Now that we’ve talked about ways to keep you healthy, let’s talk about ways to keep your partner(s) healthy. How do you feel about telling your partner(s) they’ve been exposed to HIV?” How to Bring Up the Subject of Partners Sample Transitional Phrases
 they’ve been exposed to HIV How to Bring Up the Subject of Partners Sample Transitional Phrases.")
20
Partner Management Options - At a Glance Type of Referral OptionWho notifies and refers this partner? Provider or PCRS Referral PCRS counselor, provider or clinic staff Patient ReferralPatient with coaching from provider Contract ReferralPatient makes initial attempt; if unsuccessful, PCRS provider or clinic staff conducts referral Dual ReferralPatient agrees to disclose HIV Status with provider present Four Referral Options Handout

21
Provider or PCRS Referral Often clinicians do not have sufficient time or training for PCRS A PCRS counselor or trained clinic staff can: o o Talk with your patients to identify partners and determine notification strategy o o Perform the notification o o Help other providers learn how to elicit and establish notification plans for each partner

22
Trained and experienced staff provide PCRS and other STD related counseling services in both field and clinic settings No information about your patient is given to the partner Immediate notification of partners (usually within 24-48 hours) Relieves you and your staff from those duties. PCRS Programs How Health Departments Protect Confidentiality

23
What if We Don’t Have a PCRS Program? Clinicians or clinic staff who wish to perform PCRS should know: CDC recommends in-depth standardized HIV PCRS training course(s) with subsequent mentoring and technical supervision by experienced supervisor. CDC HIV PCRS Guidelines (1998) and Interim Technical Guidance (2004) for Advancing HIV Prevention: HIV PCRS Interventions
 with subsequent mentoring and technical supervision by experienced supervisor. CDC HIV PCRS Guidelines (1998) and Interim Technical Guidance (2004) for Advancing HIV Prevention: HIV PCRS Interventions.")
24
Patient Referral The infected patient agrees to inform partners of their possible exposure and refer to appropriate services. Persons initially prefer to inform their partners themselves, although, many clients often find this more difficult than anticipated. Notification by PCRS staff seems to be substantially more effective than notification by the infected person. (CDC MMWR 2003)
.")
25
Patient should assess own willingness & ability to: Disclose own HIV status Accept that partner is not bound to protect confidentiality Contact partner promptly Find a private place for discussion Help partner understand seriousness of HIV Refer the partner for services Anticipate and handle partner’s reactions Follow-up to confirm notification occurred and to make alternate plan when necessary is ideal patient care and should occur when ever possible. Patient Referral PCRS Plan and Coaching

26
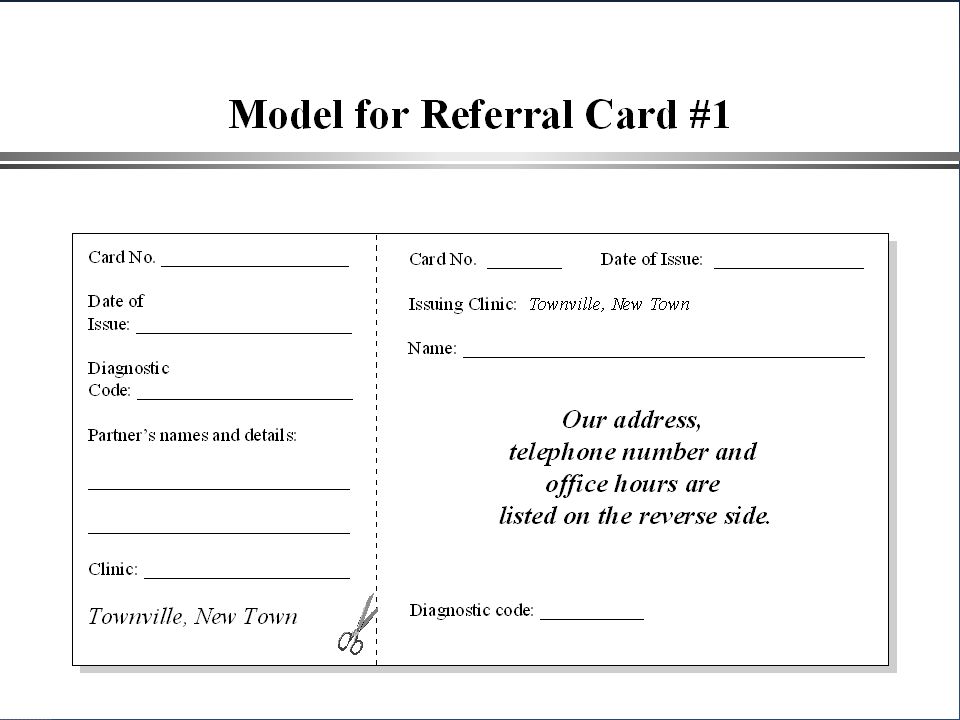
What if the Patient Wants to Inform the Partner Without Revealing His/Her Identity? Not an ideal situation, however possible if no other options Can use a referral card, which may be mailed to partner or dropped off at the house Instructs recipient to present to local clinic for evaluation because of exposure to communicable disease Use a code recognizable by providers on all islands, indicating exposure to HIV

29
Contract Referral The infected person has mutually agreed upon aset time period (usually a few days) to notify his or her partner(s). If by the agreed date, the partners have not been notified of possible exposure and of the need for counseling and testing, they are confidentially contacted by clinic staff

30
Dual Referral The infected person elects to notify their partner(s) in the presence of the provider The patient understands he/she is waiving their right to anonymity Typically done in a clinic or office setting A discussion around boundaries and session management is required prior to meeting with partners
 in the presence of the provider The patient understands he/she is waiving their right to anonymity Typically done in a clinic or office setting A discussion around boundaries and session management is required prior to meeting with partners")
31
Tapu Tapu initially says he wants to inform his wife himself (patient referral) At the next clinic visit, he admits he has not done so He agrees to find a good time to inform her, and if he is not successful within the next week, he agrees to let the provider inform her (contract referral)
 At the next clinic visit, he admits he has not done so He agrees to find a good time to inform her, and if he is not successful within the next week, he agrees to let the provider inform her (contract referral)")
32
Tapu, the Next Week Tapu has still not informed his wife He doesn’t want clinic staff going to his house, but he agrees to bring his wife in to the clinic and inform her in the presence of the provider (dual referral) She comes with him to clinic the next visit, and agrees to have HIV testing Tapu refuses to reveal the names or locations of his occasional partners on other island, but agrees to send them referral cards
 She comes with him to clinic the next visit, and agrees to have HIV testing Tapu refuses to reveal the names or locations of his occasional partners on other island, but agrees to send them referral cards")
33
Tapu, Continuing Follow-up Tapu’s wife tests negative initially, and is still negative on repeat testing 3 months later No need to test the children since the wife is negative Tapu is doing well, and continues to come to the clinic every 3 months for follow-up 6 months after his diagnosis, he is asked again about other sex partners He admits to still having contact with one of his previous partners, but says she has been tested and they are using condoms 100% of the time

34
Additional Resources Local Health Department HIV/AIDS Programs – http://www.cdc.gov/nchstp/dstd/Public_Health_dept.htm http://www.cdc.gov/nchstp/dstd/Public_Health_dept.htm National Alliance of State and Territorial AIDS Directors (NASTAD) – www.nastad.org Advancing HIV Prevention: Interim Technical Guidance for HIV Partner Counseling and Referral Services (Centers for Disease Control and Prevention) www.cdc.gov/hiv/partners/Interim/partnercounsel.htm State STD Program Managers – see handout National Coalition of STD Directors – www.ncsddc.orgwww.ncsddc.org HIV Criminal Law and Policy Project - www.hivcriminallaw.orgwww.hivcriminallaw.org STD HIV Prevention Training Center – Partner Management and Program Support Services Training – www.stdhivpreventiontraining.org STD Program Managers Handout and Resource Handout
 – Advancing HIV Prevention: Interim Technical Guidance for HIV Partner Counseling and Referral Services (Centers for Disease Control and Prevention) State STD Program Managers – see handout National Coalition of STD Directors – HIV Criminal Law and Policy Project - STD HIV Prevention Training Center – Partner Management and Program Support Services Training – STD Program Managers Handout and Resource Handout")
Similar presentations