Download presentation
Presentation is loading. Please wait.

1
Follow-up after training and supportive supervision The IMAI District Coordinator Course

2
Strengthening Health Systems District focus: Fills gaps and complements existing training/modules for specialized doctors, higher resource settings; for home-community District focus: Fills gaps and complements existing training/modules for specialized doctors, higher resource settings; for home-community Builds on and strengthens routine health services Builds on and strengthens routine health services Focus on building a district system with Focus on building a district system with Clinical teams Clinical teams Referral, back-referral; improved communication Referral, back-referral; improved communication

3
Regional Referral Hospital District Hospital Health Centre First-level health workers Clinical team may include nurse and ART Aid at first-level and doctor at second-level Second-level health workers

4
CENTRAL / PROVINCIAL Specialised referral (physicians, pediatricians, subspecialists) Referral, back- referral, clinical mentoring Patient monitoring Drugs, diagnostics, commodities, logistics support National, Regional and District ART Management
 Referral, back- referral, clinical mentoring Patient monitoring Drugs, diagnostics, commodities, logistics support National, Regional and District ART Management")
5
Individualised care for patients A Public Health approach facilitates broad coverage and enables the majority to access care and ART Some patients will develop complex problems and need specialist input to their clinical or psychosocial management Mentoring: Specialists in apex or tertiary centres linked with district generalist clinicians Referral: complex cases referred upwards for specialist care and management It is not either specialist services or a public health approach – it is both together

6
Planning for scale up Planning for scale up Preparing the community Preparing the community Establishing collaboration with partners Establishing collaboration with partners Planning capacity building Planning capacity building Establishing distance communication for clinical team support Establishing distance communication for clinical team support Follow-up support and supervision after training Follow-up support and supervision after training Medicines, diagnostics and health supplies Medicines, diagnostics and health supplies Patient monitoring Patient monitoring Orienting and optimizing entry points Orienting and optimizing entry points Prevention acceleration Prevention acceleration The IMAI district coordinator course: Administrative and managerial tasks

7
Preparation before training Training Follow-up after training: District/regional management- supportive supervision to sites: clinical, drug supply management patient monitoring Clinical supervision Facility accreditation Health worker certification Team to team exchange Other QA methods

8
Community/PLHA/stakeholder/other programme involvement Setting targets and choice of sites for HIV Care/ART Preparation IMAI training Choose clinical teams, plan training by cadres Logistics: maintaining the supply of drugs, diagnostics, equipment Establish good communication for clinical team support Patient monitoring system: registers, reports, data use IMAI Training by cadre and team On-site visits after training Mentorship Team to team support Prevention acceleration Orient and optimize entry points Evaluation

9
Patient Monitoring Supportive supervision Supportive supervision Collection/aggregation of reports Collection/aggregation of reports

10
Regional Office District Coordinator Hospital HC Monthly report, cohort analysis Aggregate data National Office

12
Aim of Clinical Mentorship As part of emergency HIV care/ART scale-up, mentorship is aimed to: As part of emergency HIV care/ART scale-up, mentorship is aimed to: Support decentralized delivery of HIV care, ART and prevention with quality of care at all levels Support decentralized delivery of HIV care, ART and prevention with quality of care at all levels Build capacity of primary-care providers to manage unfamiliar or complicated cases by consultation and on-site management where appropriate Build capacity of primary-care providers to manage unfamiliar or complicated cases by consultation and on-site management where appropriate Promote and facilitate ongoing learning, skill development and quality promotion Promote and facilitate ongoing learning, skill development and quality promotion

13
Health Centre Regular mentoring visits provided by experienced clinicians at the regional level Regional Referral Hospital Regular supportive supervision provided by the existing district management team (e.g. district medical officer, district matron) Basic administrative subunit: the district External mentors (e.g. expatriate) paired with local mentors on initial visits if sufficient expertise does not exist at regional level District Hospital
 Basic administrative subunit: the district External mentors (e.g. expatriate) paired with local mentors on initial visits if sufficient expertise does not exist at regional level District Hospital.")
14
Observe case management and reinforce skills Clinical case review Clinical team meeting Review patient monitoring system Document the visit Sequence of steps in the clinical mentoring visit

15
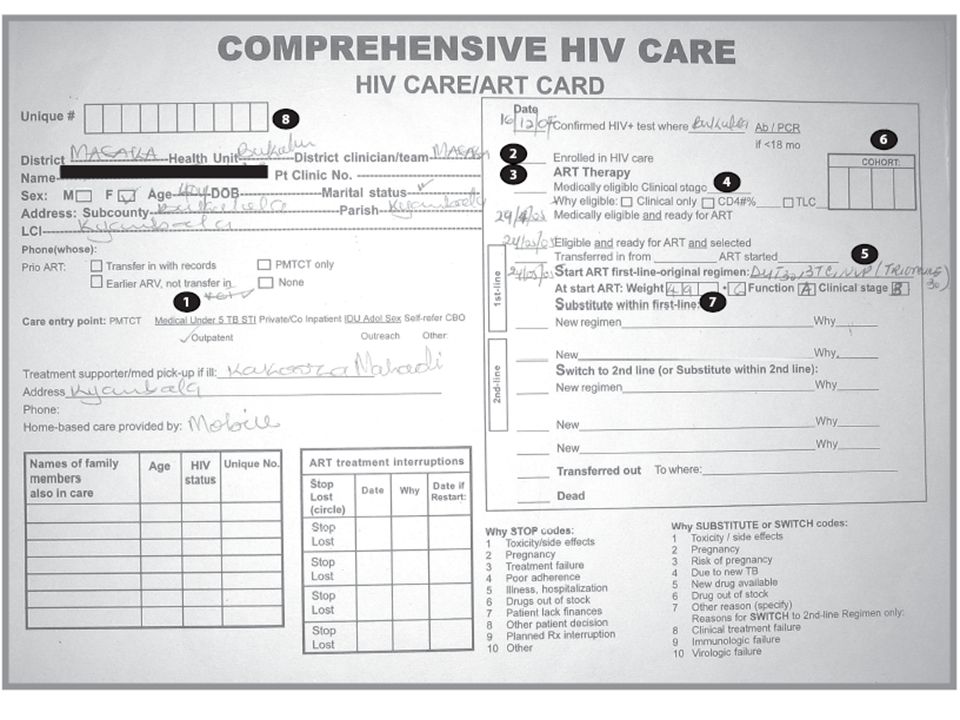
Agreed minimum essential data elements What happens to the data Indicators or other aggregated data 1.Entry point 2.Why eligible for ART 3.Reasons for: Substitution within first-line Switch/Substitution to or within second-line STOP ART 1.Number and weeks of each ART treatment interruption 2.Pregnancy status 3.Start/stop dates of prophylaxis: Cotrimoxazole Fluconazole INH 1.TB treatment 2.Adherence on ART Source: II. HIV Care, III. ART Summary, IV. Patient Encounter and Family Status Transferred to pre-ART or ART register but used only by clinical team /district ART coordinator—not transferred to quarterly report or cohort analysis Indicators for patient and programme management at the facility/district level: Distribution of entry points in patients enrolled in HIV care Why eligible for ART: clinical only, CD4 or TLC Distribution of patients not yet on ART by clinical stage Distribution of reasons for substitute, switch, stop to investigate problems; whether substitutions and switches are appropriate (use in context reviewing medical officer log) ART treatment interruptions: Number/Percentage of patients Number weeks Percentage of pregnant patients linked with PMTCT interventions (or simply use to generate lists to assure linkage) Number on cotrimoxazole, fluconazole, INH prophylaxis at end of quarter (for ordering prophylaxis drugs) Number/Percentage of patients on both TB treatment and ART 3b. % patients with good adherence to ART
 ART treatment interruptions: Number/Percentage of patients Number weeks Percentage of pregnant patients linked with PMTCT interventions (or simply use to generate lists to assure linkage) Number on cotrimoxazole, fluconazole, INH prophylaxis at end of quarter (for ordering prophylaxis drugs) Number/Percentage of patients on both TB treatment and ART 3b. % patients with good adherence to ART.")
Similar presentations







 – Executive Team Friday, 7 October 2011.>")


>")





: What Will it Take to Eliminate MTCT? Jessica Rodrigues Presentation for UNICEF Written.>")

>")
