Download presentation
Presentation is loading. Please wait.

1
Clinical perspective on pharmacogenetic labeling

2
Some drugs have such a wide therapeutic range that individualizing the dose is not important

3
Predicated upon the assumption that getting the right dose of the drug for this disease is important Probability of response and/or adverse effects related to drug dosing Titrating drug dose to response is not an optimal approach –Disease too serious to risk period of under-tx –Adverse effects too serious to risk them –Response or adverse effects are delayed or too difficult to monitor

5
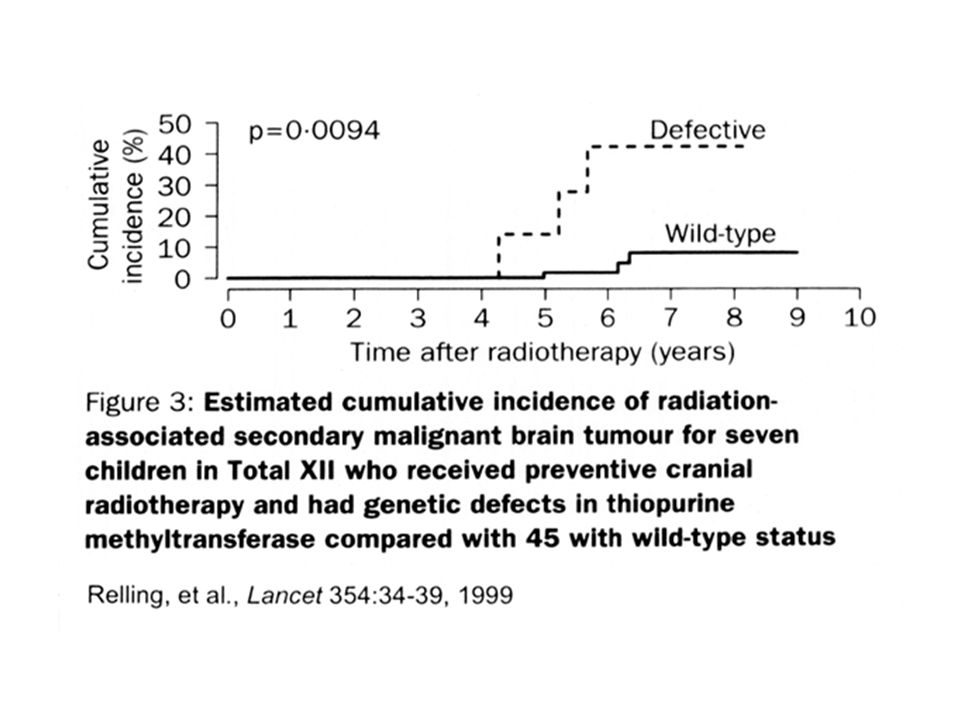
Phenotypes in ALL All: myelosuppression VCR: peripheral neuropathy Prednisone: avascular necrosis MTX: Delayed neurotoxicity Cyclophosphamide: sterility, obesity, growth All: Cure vs relapse Etoposide: 2nd tumors onset

6
E. Vessell

7
Decision-Making What do I want to know? How sure do I need to be? What am I willing to assume?

8
What do I want to know? Do specific genetic polymorphisms influence the probability of response or adverse effects? –A general effect of genetics on drug response, without any target genes ID’d, unlikely to be of use for individual prescribing

9
What do I want to know? How do polymorphisms affect drug response? (change absorption, metabolism, excretion, distribution, or pdy of the drug) Tell me this info in the context of other info on factors that affect probability of response/adverse effects (e.g. if metabolism is subject to polymorphism plus other metabolized-drugs on board….)
 Tell me this info in the context of other info on factors that affect probability of response/adverse effects (e.g. if metabolism is subject to polymorphism plus other metabolized-drugs on board….).")
10
What do I want to know? Tell me what doses/routes were tested –Low doses/long exposures don’t saturate enzymes –Hepatic metabolism may be more relevant for oral or prolonged exposures (e.g. MTX, teniposide)
.")
11
What am I willing to assume? In vitro, preclinical data can be helpful…. Enzymes saturate: There will likely be competition, and thus possible saturation, if > 1 drug share the same gene products (e.g. low CYP3A activity might be more problematic in a pt taking > 1 CYP3A- substrate/drug than in a pt taking 1 CYP3A- substrate/drug---e.g. VCR, erythromycin, azole) Effects of polymorphisms gleaned from one drug may have relevance for an independent drug that shares the same gene product (e.g. CYP2D6 PM status should be mentioned for ~all CYP2D6 substrates)
 Effects of polymorphisms gleaned from one drug may have relevance for an independent drug that shares the same gene product (e.g. CYP2D6 PM status should be mentioned for ~all CYP2D6 substrates).")
12
Dose recommendations in relation to P450 genotype Drug Average PM EM UMEnzyme dose (mg) Propafenon 45040%130%CYP2D6 Amitriptyline 15050 %120% -”- Tropisetron 1030%130% -”- Nortriptyline 15050% 140% 230% -”- Metoprolol 10030%140% -”- Lansoprazole 4020%110% CYP2C19 Omeprazole 4020%110% CYP2C19 S-Warfarin 320%130%CYP2C9 Kirchheiner et al., Acta Psyciatr Scand 104: 173-192, 2001.
 Propafenon 45040%130%CYP2D6 Amitriptyline %120% - - Tropisetron 1030%130% - - Nortriptyline 15050% 140% 230% - - Metoprolol 10030%140% - - Lansoprazole 4020%110% CYP2C19 Omeprazole 4020%110% CYP2C19 S-Warfarin 320%130%CYP2C9 Kirchheiner et al., Acta Psyciatr Scand 104: , 2001.")
13
What do I want to know? What is the frequency of the specific genotypes in the 3 largest ethnic/racial groups (whites, blacks, Asians)? –AA, homozygous common or wild-type –Aa, heterozygotes –aa, homozygous variant or defective Could give allele frequencies, but most clinicians won’t be familiar with calculating genotypic frequencies
. –AA, homozygous common or wild-type –Aa, heterozygotes –aa, homozygous variant or defective Could give allele frequencies, but most clinicians won’t be familiar with calculating genotypic frequencies.")
14
Hardy-Weinberg P = frequency of wild-type allele(s) Q = frequency of variant allele(s) 1 = p + q P 2 = frequency of wild-type genotype Q 2 = frequency of variant genotype 2pq = frequency of heterozygote genotype
 Q = frequency of variant allele(s) 1 = p + q P 2 = frequency of wild-type genotype Q 2 = frequency of variant genotype 2pq = frequency of heterozygote genotype")
15
What is the difference between phenotype and genotype? Phenotype is the bottom line, but phenotype can be influenced by concurrent drugs, diet etc DNA is DNA is DNA (except for allogeneic BMT recipients and if source of DNA is tumor) Genotype has to be studied only once (unless technology changes to capture more variants and pt was originally genotyped as < homoz. Variant) Genotype more susceptible to false negatives than phenotype
 Genotype has to be studied only once (unless technology changes to capture more variants and pt was originally genotyped as < homoz. Variant) Genotype more susceptible to false negatives than phenotype.")
16
Genotyping Tests (1) Multiple types of “variant” and “wild-type” alleles exist for every gene False negatives: A genotyping test can’t reveal any information about areas of the gene not interrogated by the test (e.g. one can only know that the pt is “wild-type” at the loci tested) Number of false negatives depends on proportion of inactivating variants accounted for by the tested variants (must be disclosed by the test)
 Number of false negatives depends on proportion of inactivating variants accounted for by the tested variants (must be disclosed by the test).")
17
Genotyping Tests (2) If a pt is “heterozygote” at > 1 polymorphic site in a gene, must understand whether those polymorphisms are allelic (and thus the pt is a likely “heterozygote”) or are likely on separate alleles (and thus the pts is homozygous variant)—but the genotyping test should disclose this False positives: should not be a problem
 If a pt is heterozygote at > 1 polymorphic site in a gene, must understand whether those polymorphisms are allelic (and thus the pt is a likely heterozygote ) or are likely on separate alleles (and thus the pts is homozygous variant)—but the genotyping test should disclose this False positives: should not be a problem")
18
Some knowledge of genetics/molecular biology helpful… Heterozygote phenotypes are generally in between those of the 2 homozygote genotypes Homozygous variant defined by presence of 2 different variant alleles in many cases Gene duplications are possible and may “offset” a variant allele

19
Frequency Low Enzyme activity/ drug clearance High Stop codons Deletions Missense SNPs Splice defects Heterozygous deleterious SNPs Unstable protein Conserved aa substitutions Promoter/3´- 5´SNPs Gene duplication Induction Possible Drug Metabolism Phenotypes and Genotypes

20
Is this too much to expect? To monitor effects of imatinib, we need to follow t(9;22) –Can be assessed by cytogenetics or FISH or RT-PCR Presence of G6PD deficiency predisposes to MetHB for several drugs; –Activity affected by concurrent drugs, hematocrit Hepatic dosing using Child-Pugh scores Cardiac output vs CVP for pressors
 –Can be assessed by cytogenetics or FISH or RT-PCR Presence of G6PD deficiency predisposes to MetHB for several drugs; –Activity affected by concurrent drugs, hematocrit Hepatic dosing using Child-Pugh scores Cardiac output vs CVP for pressors.")
21
What do I want to know? –Phenotype: in general how the test is done (with a blood sample, name of the test) direction (e.g. low activity is associated with the variant allele and with greater risk of adverse effects) what interferes with test –Genotype: estimate of the number of inactivating variants their approximate frequencies proportion of phenotype accounted for by the genotypes (e.g. the *5, *19, and *22 inactive/variant alleles account for 85%, 92%, and 90% of low-activity alleles among whites, blacks, and Asians)
 direction (e.g. low activity is associated with the variant allele and with greater risk of adverse effects) what interferes with test –Genotype: estimate of the number of inactivating variants their approximate frequencies proportion of phenotype accounted for by the genotypes (e.g. the *5, *19, and *22 inactive/variant alleles account for 85%, 92%, and 90% of low-activity alleles among whites, blacks, and Asians).")
22
What do I want to know? Negative results can be helpful (e.g. this drug is not a substrate for the genetically regulated CYP2D6 or CYP2C19 enzymes)
.")
23
How sure do I need to be? Give me some real data…. Avg/s.d. (median +/- CI) dose in AA vs Aa vs aa pts = 30, 50, and 80 mg/m2 50% (95% CI) of pts with vs 10% (95% CI) of pts without toxicity (e.g. QT widening) were AA vs Aa/aa pts Given a dose of 50 mg, 10%, 30%, and 80% (95% CI) of AA, Aa, and aa pts displayed evidence of response/toxicity
 dose in AA vs Aa vs aa pts = 30, 50, and 80 mg/m2 50% (95% CI) of pts with vs 10% (95% CI) of pts without toxicity (e.g. QT widening) were AA vs Aa/aa pts Given a dose of 50 mg, 10%, 30%, and 80% (95% CI) of AA, Aa, and aa pts displayed evidence of response/toxicity.")
24
Greater oral mucositis index (OMI) after low-dose MTX among BMT patients with mutant MTHFR C677T genotypes than among patients with C677C genotypes Ulrich et al Blood 98:231-4, 2001 50%40%10%
 after low-dose MTX among BMT patients with mutant MTHFR C677T genotypes than among patients with C677C genotypes Ulrich et al Blood 98:231-4, %40%10%")
25
Effect of the CYP2C9 genotype on the daily dose of warfarin to achieve target INR Warfarin, mg/day wt/wt wt/mut wt/varvar/var Wadelius et al., 2002

26
Cure rates for H. pylori infections may depend upon CYP2C19 genotypes 62 pts with duodenal or gastric ulcer treated with omeprazole 20 mg and amoxicillin 20% of Asian and 4% of whites are homo. variant N = 28 25 9 Ann Intern Med 1998;129:1027-30

27
Evans et al, SJCRH, 2000 Polymorphism in TPMT leads to 3 distinct phenotypes, Who differ in their 6MP dosage requirements

28
Cumulative incidence (CI) of Dosage Decrease based on Genotype Relling et al JNCI, 1999
 of Dosage Decrease based on Genotype Relling et al JNCI, 1999")
29
Labeling Description Clinical Pharmacology Indications and Usage Contraindications Warnings Precautions (general, info for pts, lab tests, drug interxs, carcinogenesis, pregnancy, nursing mothers, pediatrics) Adverse reactions Overdosage Dosage and administration (general, renal, hepatic) How supplied References
 Adverse reactions Overdosage Dosage and administration (general, renal, hepatic) How supplied References")
30
Labeling: include cross references among sections Clinical Pharmacology: include mechanism of how polymorphism affects the drug and some references Warnings: if indicated Precautions: include lab test information Adverse reactions: include frequency among different genotypes Overdosage: mention if genetics likely to affect Dosage and administration (general, renal, hepatic, and genetic)
")
31
Terminology Use colloquial terms where relevant (EMs, PMs, ultra-rapid, fast, slow, etc) Avoid “mutant” (prefer variant or defective) Avoid “normal” (prefer wild-type or common or descriptive, e.g. high-activity allele) Map HUGO nomenclature-designations to “wild-type/common” or “variant/defective” in the label
 Map HUGO nomenclature-designations to wild-type/common or variant/defective in the label.")
32
Decision Tree for Pgenetics

Similar presentations

 By Oksana Ekkert>")












 July 27, 2010.>")

, experimented on peas Mendelian inheritance, single (or very few) genes controlling certain expressed.>")

 New Life College Of Nursing Karachi 11/7/20141Antimicrobial medications.>")
