Download presentation
Presentation is loading. Please wait.

1
Advances Ib Ob/Gyn Cross Sectional Imaging

2
JASLOK HOSPITAL AND RESEARCH CENTRE,
DR. SONAL GARG JASLOK HOSPITAL AND RESEARCH CENTRE, MUMBAI

3
MRI evaluation of Pelvic floor disorders
Urinary and anal incontinence affects a large proportion of the female population MRI is now the modality of choice for preop planning of pelvic floor repairs Superior soft tissue evaluation of viscera, pelvic musculature and fascial investments Guides detailed evaluation of repair in cases that do not resolve with conservative Rx. MRI has led to a breakthrough in the evaluation of pelvic floor disorders. It accurately identifies the prolapsing organ and unsuspected defects in pelvic floor support.

4
Normal position of the bladder base, vaginal vault and ano- rectal junction at rest
Normal position of the bladder base, vaginal vault and ano- rectal junction with Valsalva

5
ANAL SPHINCTER INJURIES
Internal and External Sphincter trauma seen in obstetric injuries leads to fecal incontinence. Pelvic floor denervation secondary to vaginal delivery may lead to perineal descent and posterior compartment deficits.

6
MRI of the ANAL SPHINCTERS
Recent advances in MRI technologies using the endoanal coil, rapid sequencing, and cinematic display have enabled dynamic defecography. Used to evaluate both muscular and connective tissue supports of the pelvis. Muscular defects along with POP and perineal descent can be assessed.

7
At rest, the bladder base and Cervix is normal.
The anal sphincter is open with an abnormally low placed anorectal junction The evacuation phase shows a large descending cystocele and Severe descending perineal syndrome

8
Dynamic MRI in Stress Urinary Incontinence
Used to asses the functional and anatomic changes that occur during stress incontinence Dynamic MRI guides management options- response with pessary or need for surgery

9
Dynamic MRI A- MRI without pessary B- MRI with pessary
(line represents the pubococcygeal line)
")
10
Fast MRI with and without pessary while performing Valsalva
A- Valsalva with pessary B- Valsalva without pessary (line represents posterior urethro-vesical angle)
")
11
FETAL MRI- A Developing technique for the Developing patient

12
What does it provide? Offers complete evaluation of the fetus even in difficult situations like oligohydramnios, maternal obesity, limitations of fetal position etc. Overcomes the problems of Calvarial and bone calcification which may obscure detail. Gives more information to guide management and counselling when an abnormality is detected on ultrasound

13
FETAL MRI- Advantages Excellent spatial soft tissue resolution
Large field of view-Detailed evaluation of fetal and extra-fetal structures. Three dimensional information with multiplanar imaging. Established safety in second trimester Limitations of fetal movement has been overcome by using HASTE sequences Fast due to use of HASTE sequences. Maternal or fetal sedation not required

14
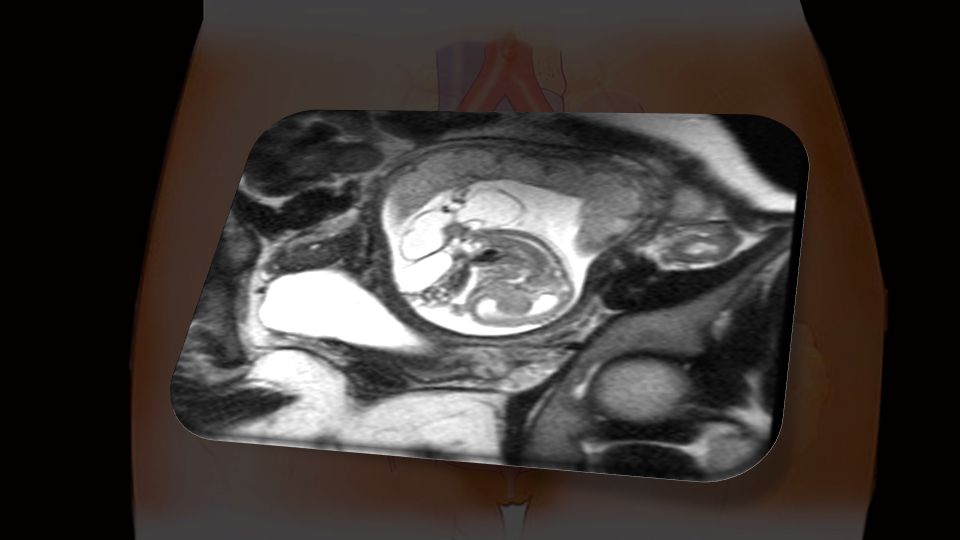
CASE 1- RECURRENT PREGNANCY LOSS

18
FETAL MRI- Applications
Central nervous system and spine pathologies: Evaluation of Colpocephaly Agenesis of the Corpus Callosum Posterior fossa anomalies- is there Dandy Walker malformation? Intra-axial and extra-axial mass lesions and fluid collections Destructive brain lesions and haemorrhage Spinal dysraphism- delineates the extent and level Sacrococcygeal teratoma- Intrapelvic and abdominal extent of tumor, mass effect on adjacent organs Caudal- low sacral NTD maybe missed on ultrasound MR imaging plays a critical role in characterizing the contents of the herniated sac and assessing the intracranial anatomy, findings that have a critical role in diagnosis, counseling, management, and prognosis..In cases of encephalocele, MR imaging can show the underlying brain to appear normal (see Fig. 18A) or abnormal (see Fig. 18B). In some cases, because of fetal position, the encephalocele itself may be difficult to visualize with ultrasound, but is better seen with MR imaging (see Fig. 18C). The additional information provided by MR imaging can help identify cases with more favorable prognosis and cases with poor prognosis. Even when ultrasound shows the findings well, MR imaging is helpful for the patients and the neurologists counseling the patients in terms of better visualizing and understanding the anomalies present.
 or abnormal (see Fig. 18B). In some cases, because of fetal position, the encephalocele itself may be difficult to visualize with ultrasound, but is better seen with MR imaging (see Fig. 18C). The additional information provided by MR imaging can help identify cases with more favorable prognosis and cases with poor prognosis. Even when ultrasound shows the findings well, MR imaging is helpful for the patients and the neurologists counseling the patients in terms of better visualizing and understanding the anomalies present.")
19
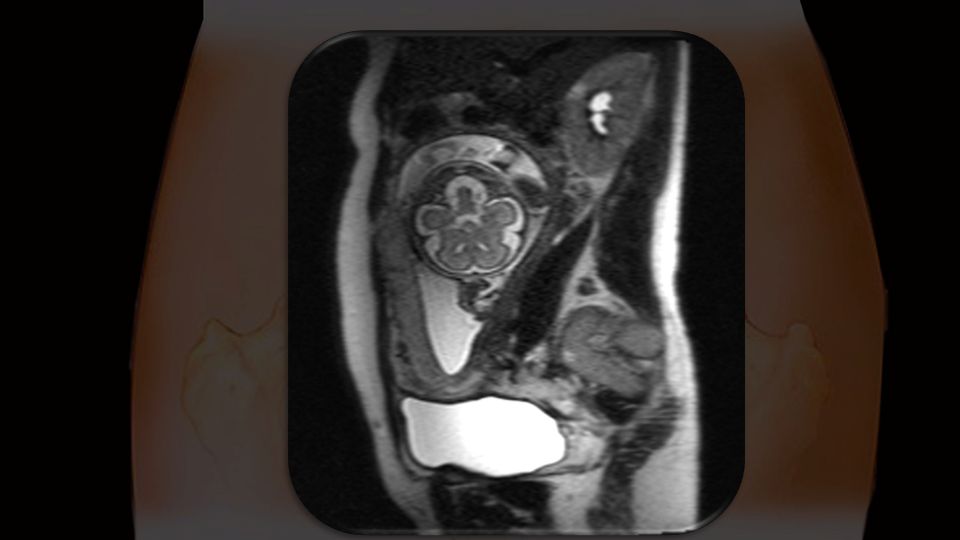
CASE 1- PERSISTENT COLPOCEPHALY

21
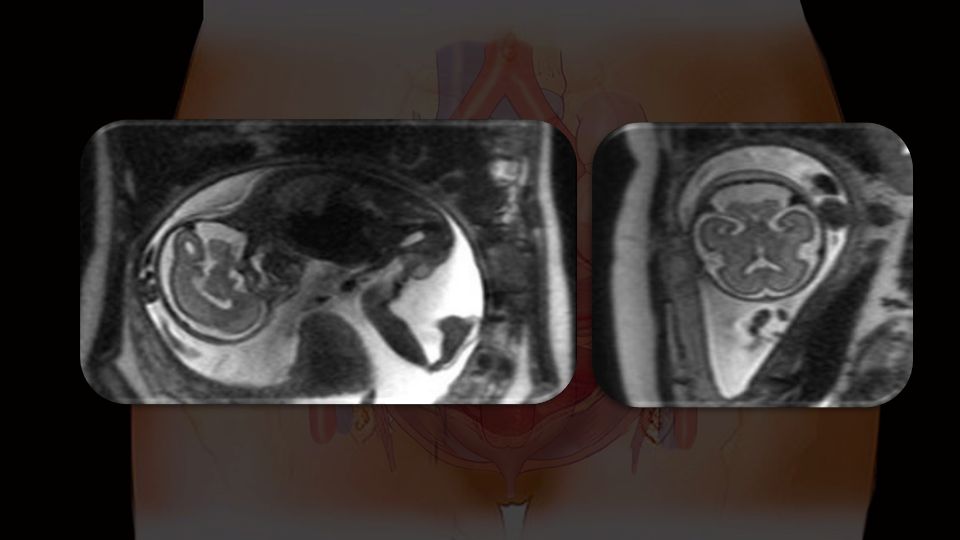
CASE 2- PROMINENT POSTERIOR CISTERNA MAGNA

25
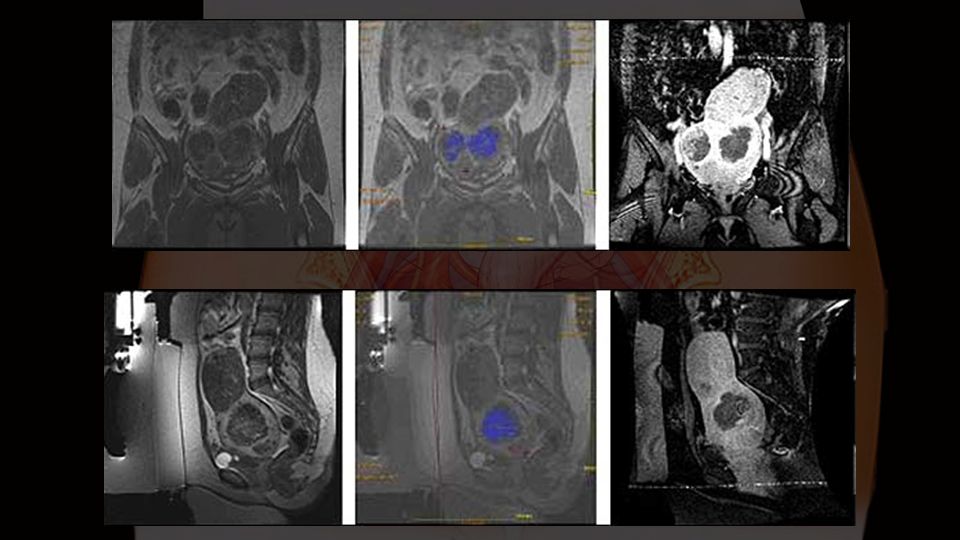
CASE 3- PRECIOUS PREGNANCY WITH SUSPECTED ARNOLD CHIARI MALFORMATION

26
FETAL MRI- Applications
Intrathoracic lesions: CCAM- cystic nature, differentiates it from Congenital diaphragmatic hrenia containing bowel loops Pulmonary sequestration Congenital diaphragmatic hernia- extent, severity scores such as lung volumetry

27
FETAL MRI- The future Diffusion tensor imaging and Perfusion studies:
Extremely sensitive and specific sequences to detect cerebral ischemia Can determine the onset of ischemia and detailed extent of neural damage for prognosis and guiding management

28
MRI guided High Intensity Focused Ultrasound- The New Kid on the Block

29
What is HIFU? Thermal ablation technique
Sound waves focused to deliver heat Results in tissue necrosis and cell death During the procedure you lie on your stomach on a patient table that fits into a standard MRI scanner. First, the doctor identifies the fibroid(s) on MR images taken of your pelvic region. Then, after detailed planning, high energy focused ultrasound waves heat a small spot in the uterine fibroid to a temperature of up to 85oC. During the pulse or sonication, which lasts about 15 seconds, the doctor monitors the progress and reviews temperature-sensitive images. Since each sonication treats a very small volume, this process will be repeated until the required volume is treated, typically about 50 times. The procedure lasts about 3 hours depending upon the size and number of fibroids treated. Following the treatment the body gradually removes the treated tissue over a period of months, providing symptom relief.
 on MR images taken of your pelvic region. Then, after detailed planning, high energy focused ultrasound waves heat a small spot in the uterine fibroid to a temperature of up to 85oC. During the pulse or sonication, which lasts about 15 seconds, the doctor monitors the progress and reviews temperature-sensitive images. Since each sonication treats a very small volume, this process will be repeated until the required volume is treated, typically about 50 times. The procedure lasts about 3 hours depending upon the size and number of fibroids treated. Following the treatment the body gradually removes the treated tissue over a period of months, providing symptom relief.")
32
What does the MR guidance provide?
3D multiplanar imaging of the fibroid Clearly identifies the position and extent of the fibroid, what portion has to be treated Provides real time information about temperature changes of the treated fibroid to ensure ablation. Clear visualization of the fibroid

33
MrgFUS- What are the advantages?
Non-invasive, does not require hospital stay Uterus conserving Offers good symptom relief and excellent quality of life

34
MrgFUS- Inclusion Criteria
Women between 18 and 59 years Weight less than 140 kg Uterine size less than 24 weeks Symptomatic fibroids- bleeding, pressure, pain, urinary symptoms etc.

35
MrgFUS- Exclusion Criteria
Extensive scarring along the lower abdominal wall or surgical clips in the direct path of the beam. Not yet approved for women seeking fertility Pregnant patients

36
THANK YOU

Similar presentations












>")






 is a condition in which a woman's uterus (womb) sags or slips out of its normal position. The uterus.>")




