Download presentation
Presentation is loading. Please wait.

1
The Goldilocks Quandary: How much patient contact is just right? NAACCR Annual Conference 2013 C. Janna Harrell, M.S. Senior Research Analyst Utah Cancer Registry

2
Too little contact

3
Too much contact

4
The Goldilocks Quandary Too Little High

5
Overview Cancer registry research policies The sample The analysis (models and methods) The results The grand finale- o How much contact is just right?
 The results The grand finale- o How much contact is just right")
6
Recruitment through US Cancer Registries 1. Researcher initiates contact with patient 2. Registry initiates contact with patient Opt-out approach Opt-in approach 3.Physician notification required Beskow, L. M., R. S. Sandler and M. Weinberger (2006). "Research recruitment through US central cancer registries: balancing privacy and scientific issues." Am J Public Health 96(11): 1920-1926.
. Research recruitment through US central cancer registries: balancing privacy and scientific issues. Am J Public Health 96(11):")
7
Sample Patients contacted Jan. 2007-Oct. 2012 11 studies Excludes : Deceased patients/next-of-kin studies “Lost” patients Ineligible patients 9,488 patients 75% permission studies 25% consent studies

8
Code Definition Code Definition 100 Mailed 1st letter to patient 205 Spoke with- considering 101 Mailed 2nd letter to patient 206 Spoke with- willing 102 Letter returned w/forwarding addresses 207 Spoke with- Received, already sent to us 103 Letter returned, NO forwarding address 208 Spoke with- too sick 108 Mailed letter to new address as per patient 209 Spoke with- no cancer 110 Mailed additional items 214 Patient left message for Coordinator 200 Left message on machine 215 Spoke with- Refused 201 Left message with person 217 Spoke with- not received 202 No answer 300 Survey returned / no consent form 204 Disconnected/ Wrong number 302 Consent returned/no survey

9
Analysis Bi-variate analyses using chi-square and ANOVA (p value <0.05) Multinomial logistic regression models o 3 models: Everyone (excluding site) & by sex (including site)
 Multinomial logistic regression models o 3 models: Everyone (excluding site) & by sex (including site)")
10
Regression Models Outcome: Response to contact effort –Categorical: yes, no, nonresponsive Predictors: Sex Age at Diagnosis Site Age at Contact Stage Time from diagnosis to first contact attempt

11
Demographics: Sex & Study Type Response n (%) AllYesNo Non- responsive Total 9488 5416 (57%) 2284 (24%)1788 (19%) Sex* Female 5749 (61%)3278 (57%)1238 (22%)1232 (21%) Male 3739 (39%)2138 (57%)1046 (28%)555 (15%) Study Type* Permission 7108 (75%)3956 (56%)1619 (23%)1533 (22%) Consent 2380 (25%)1460 (61%)665 (28%)255 (11%) *P value <0.0001 chi squared test Consent studies only included prostate cancers
 AllYesNo Non- responsive Total (57%) 2284 (24%)1788 (19%) Sex* Female 5749 (61%)3278 (57%)1238 (22%)1232 (21%) Male 3739 (39%)2138 (57%)1046 (28%)555 (15%) Study Type* Permission 7108 (75%)3956 (56%)1619 (23%)1533 (22%) Consent 2380 (25%)1460 (61%)665 (28%)255 (11%) *P value < chi squared test Consent studies only included prostate cancers")
12
Demographics: Site Characteristics Response n (%) All Yes No Nonresponsive Total 9488 5416 2284 1788 Sex* Female 5749 (61 %) 3278 (57 %) 1238 (22%) 1232 (21 %) Male 3739 (39 %) 2138 (57 %) 1046 (28 %) 555 (15 %) Site* Breast 4260 (45 %) 2515 (59 %) 810 (19 %) 935 (22 %) Prostate 2380 (25 %) 1460 (61 %) 665 (28 %) 255 (11 %) Colorectal 1531 (16 %) 736 (48 %) 507 (33 %) 288 (19 %) CLL/SLL 659 (7 %) 318 (48 %) 147 (22 %) 194 (29 %) MM 175 (2 %) 95 (54 %) 58 (33 %) 22 (13 %) Ovary /female genital 358 (4 %) 228 (64 %) 83 (23 %) 47 (13 %) Childhood cancer 125 (1 %) 64 (51 %) 14 (11 %) 47 (38 %) Site* Response n (%) AllYesNo Non- responsive Breast 4260 (45%)2515 (59%)810 (19%)935 (22%) Prostate 2380 (25%)1460 (61%)665 (28%)255 (11%) Colorectal 1531 (16%)736 (48%)507 (33%)288 (19%) CLL/SLL 659 (7%)318 (48%)147 (22%)194 (29%) MM 175 (2%)95 (54%)58 (33%)22 (13%) Ovary /female genital 358 (4%)228 (64%)83 (23%)47 (13%) Childhood cancer 125 (1%)64 (51%)14 (11%)47 (38%) *P value <0.0001 chi squared test ICCC coded
 All Yes No Nonresponsive Total Sex* Female 5749 (61 %) 3278 (57 %) 1238 (22%) 1232 (21 %) Male 3739 (39 %) 2138 (57 %) 1046 (28 %) 555 (15 %) Site* Breast 4260 (45 %) 2515 (59 %) 810 (19 %) 935 (22 %) Prostate 2380 (25 %) 1460 (61 %) 665 (28 %) 255 (11 %) Colorectal 1531 (16 %) 736 (48 %) 507 (33 %) 288 (19 %) CLL/SLL 659 (7 %) 318 (48 %) 147 (22 %) 194 (29 %) MM 175 (2 %) 95 (54 %) 58 (33 %) 22 (13 %) Ovary /female genital 358 (4 %) 228 (64 %) 83 (23 %) 47 (13 %) Childhood cancer 125 (1 %) 64 (51 %) 14 (11 %) 47 (38 %) Site* Response n (%) AllYesNo Non- responsive Breast 4260 (45%)2515 (59%)810 (19%)935 (22%) Prostate 2380 (25%)1460 (61%)665 (28%)255 (11%) Colorectal 1531 (16%)736 (48%)507 (33%)288 (19%) CLL/SLL 659 (7%)318 (48%)147 (22%)194 (29%) MM 175 (2%)95 (54%)58 (33%)22 (13%) Ovary /female genital 358 (4%)228 (64%)83 (23%)47 (13%) Childhood cancer 125 (1%)64 (51%)14 (11%)47 (38%) *P value < chi squared test ICCC coded")
13
Demographics: Stage Stage* Response n (%) AllYesNo Non- responsive In situ855 (9%)496 (58%)169 (20%)190 (22%) Local5033 (53%)2893 (57%)1248 (25%)892 (18%) Regional2366 (25%)1354 (57%)576 (24%)436 (18%) Distant973 (10%)515 (53%)243 (25%)215 (22%) Unstaged261 (3%)158 (61%)48 (18%)55 (21%) *P value <0.001 chi squared test SEER Summary Stage 2000
 AllYesNo Non- responsive In situ855 (9%)496 (58%)169 (20%)190 (22%) Local5033 (53%)2893 (57%)1248 (25%)892 (18%) Regional2366 (25%)1354 (57%)576 (24%)436 (18%) Distant973 (10%)515 (53%)243 (25%)215 (22%) Unstaged261 (3%)158 (61%)48 (18%)55 (21%) *P value <0.001 chi squared test SEER Summary Stage 2000")
14
Demographics: Time Time* AllYesNo Non- responsive MeanRangeMean (S.D.) Age at Diagnosis 520-9451 (11.6)55 (12.0)50 (12.7) Age at Contact 6118-10160 (10.7)64 (10.8)58 (11.4) Years from Diagnosis to First Contact 8.50-398.4 (6.0) 9 (6.4) *P value <0.001 ANOVA S.D.- standard deviation
 Age at Diagnosis (11.6)55 (12.0)50 (12.7) Age at Contact (10.7)64 (10.8)58 (11.4) Years from Diagnosis to First Contact (6.0) 9 (6.4) *P value <0.001 ANOVA S.D.- standard deviation")
15
Basic Model- both sexes Comparison Reply (ref=yes) Odds Ratio (C.I.) Distant vs. Local Stage* No0.69 (0.56-0.83) Male vs. Female* Non- responsive 1.24 (1.05-1.45) Age at Diagnosis*No1.04 (1.04-1.05) Age at Diagnosis* Non- responsive 0.99 (0.987-0.998) Years from Diagnosis to First Contact Attempt* No1.04 (1.03-1.05) *P value < 0.05
 Male vs. Female* Non- responsive 1.24 ( ) Age at Diagnosis*No1.04 ( ) Age at Diagnosis* Non- responsive 0.99 ( ) Years from Diagnosis to First Contact Attempt* No1.04 ( ) *P value <")
16
Females: Site Comparison (ref=colorectal) Reply (ref=yes) Odds Ratio (C.I.) Breast* No 0.62 (0.50-0.77) Breast* Non- responsive 0.74 (0.59-0.93) CLL/SLL* No 0.59 (0.38-0.93) CLL/SLL* Non- responsive 2.35 (1.48-3.73) Ovary/Genital Organ* No 0.61 (0.44-0.86) Ovary/Genital Organ* Non- responsive 0.49 (0.33-0.73) *P value < 0.05
 Reply (ref=yes) Odds Ratio (C.I.) Breast* No 0.62 ( ) Breast* Non- responsive 0.74 ( ) CLL/SLL* No 0.59 ( ) CLL/SLL* Non- responsive 2.35 ( ) Ovary/Genital Organ* No 0.61 ( ) Ovary/Genital Organ* Non- responsive 0.49 ( ) *P value < 0.05")
17
Females Comparison Reply (ref=yes) Odds Ratio (C.I.) Distant vs. Local* Non- responsive 0.67 (0.45-0.99) Age at Diagnosis*No1.04 (1.03-1.05) Age at Diagnosis* Non- responsive 0.99 (0.979-0.996) Years from Diagnosis to First Contact Attempt* No 1.01 (0.998-1.021) *P value < 0.05
 Age at Diagnosis*No1.04 ( ) Age at Diagnosis* Non- responsive 0.99 ( ) Years from Diagnosis to First Contact Attempt* No 1.01 ( ) *P value <")
18
Males Comparison Reply (ref=yes) Odds Ratio (C.I.) CLL/SLL vs. Colorectal* No0.42 (0.22-0.81) Age at Diagnosis* No1.05 (1.04-1.07) Age at Diagnosis* Nonresponsive0.98 (0.969-0.997) *P value < 0.05
 Age at Diagnosis* No1.05 ( ) Age at Diagnosis* Nonresponsive0.98 ( ) *P value <")
19
All Contact Attempts

20
Contact Attempts by Response

21
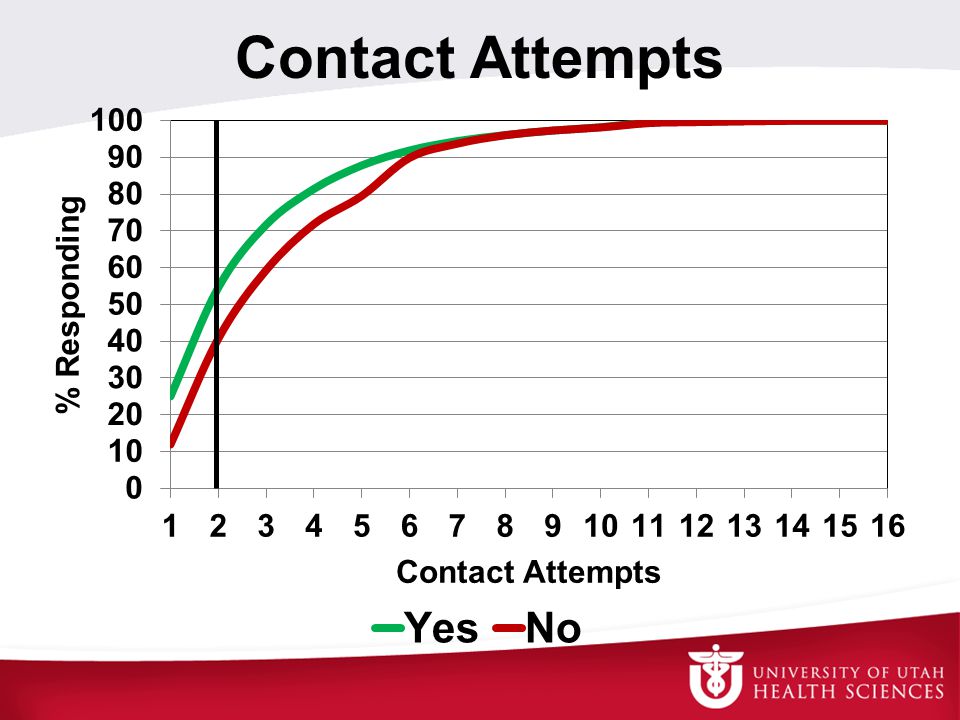
Contact Attempts

25
Conclusions Only men get prostate cancer After 8 contact attempts 95% of those who will respond, have responded As age increases, refusals increase and nonresponders decrease Younger ages were more likely to be nonresponders

26
Limitations Contact protocol varied by study Consent studies lack diversity Population lacks diversity Geography and SES Generalizability –Limited sites considered –Are Utahns more willing to participate? Simmons, R.G., A.L. Yuan-Chin, et al. (2013). “Examining the challenges of family recruitment to behavioral intervention trials…” Trials 14:116
. Examining the challenges of family recruitment to behavioral intervention trials… Trials 14:116.")
27
Future Research & Considerations Adjust contact effort based on target population Additional analysis with a diverse population including additional variables Examine relationship between registry policies, participation rates, and study’s response rate –Simmons, R.G., A.L. Yuan-Chin, et al. (2013). “Examining the challenges of family recruitment to behavioral intervention trials…” Trials 14:116
. Examining the challenges of family recruitment to behavioral intervention trials… Trials 14:116.")
28
Acknowledgment: The UCR Team Co-authors: Susan VanRoosendaal, Kim Herget, Nan Stroup UCR Operations Staff Patient Contact Staff

29
Acknowledgment Research was supported by the Utah Cancer Registry, which is funded by Contract No. HHSN261201000026C from the National Cancer Institute's SEER Program with additional support from the Utah State Department of Health and the University of Utah

30
Contact me http://UCR.utah.edu Janna Harrell, M.S. Senior Research Analyst Utah Cancer Registry 801-581-8407 Janna.Harrell@hsc.utah.edu

31
Thank you for your time and attention.

Similar presentations







>")













