Download presentation
Presentation is loading. Please wait.

1
Hyperglycemic Crises in Adult Patients with Diabetes
American Diabetes Association July 2009 Avigail Martha Pastoral

2
Diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state (HHS) are acute complications of diabetes associated with absolute or relative insulin deficiency, volume depletion, and acid-base abnormalities.
 and hyperglycemic hyperosmolar state (HHS) are acute complications of diabetes associated with absolute or relative insulin deficiency, volume depletion, and acid-base abnormalities.")
3
The triad of uncontrolled hyperglycemia, metabolic acidosis, and increased total body ketone concentration characterizes DKA. HHS is characterized by severe hyperglycemia, hyperosmolality, and dehydration in the absence of significant ketoacidosis.

4
Epidemiology: DKA ages of 18 and 44 years (56%) and 45 and 65 years (24%), with only 18% of patients <20 years of age. Two-thirds: type 1 diabetes and 34% to have type 2 diabetes 50% were female 45% were nonwhite DKA is the most common cause of death in children and adolescents with type 1 diabetes and accounts for half of all deaths in diabetic patients younger than 24 years of age (5,6) Death relates to the underlying precipitating illness rather than complications of hyperglycemia
 Death relates to the underlying precipitating illness rather than complications of hyperglycemia.")
5
Diabetic ketoacidosis
Symptoms Nausea/vomiting Thirst/polyuria Abdominal pain Shortness of breath Physical findings Tachycardia Dehydration / hypotension Tachypnea / Kussmaul respirations/respiratory distress Abdominal tenderness (mimics acute pancreatitis or surgical abdomen) Lethargy /obtundation / cerebral edema / possibly coma
 Lethargy /obtundation / cerebral edema / possibly coma.")
6
Hyperglycemic Hyperosmolar State
The prototypical patient with HHS is an elderly individual with type 2 DM, with a several week history of polyuria, weight loss, and diminished oral intake that culminates in mental confusion, lethargy, or coma. The physical examination reflects profound dehydration and hyperosmolality and reveals hypotension, tachycardia, and altered mental status. Notably absent are symptoms of nausea, vomiting, and abdominal pain and the Kussmaul respirations characteristic of DKA.

7
Epidemiology: HHS Mortality attributed to HHS is considerably higher than that attributed to DKA, with recent mortality rates of 5–20% (10,11).
.")
8
Inc glucose production and impaired glucose utilization
Pathogenesis Inc glucose production and impaired glucose utilization

9
plasma insulin adequate to prevent excessive lipolysis and subsequent ketogenesis but not hyperglycemia (4).
.")
10
Increasing evidence indicates that hyperglycemic crises is associated with a severe inflammatory state which return to near-normal values with insulin therapy and hydration within 24 h. The procoagulant and inflammatory states may be due to nonspecific phenomena of stress and may partially explain the association of hyperglycemic crises with a hypercoagulable state (21).
.")
11
Laboratory and Clinical Characteristics
Table 1—Diagnostic criteria for DKA and HHS DKA Mild Moderate Severe HHS Plasma glucose (mg/dl) >250 >250 >250 >600 Arterial pH – –7.24 < >7.30 Serum bicarbonate (mEq/l) 15– to <15 <10 >18 Urine ketones* Positive Positive Positive Small Serum ketones* Positive Positive Positive Small Effective serum osmolality (mOsm/kg)† Variable Variable Variable >320 Anion gap‡ >10 >12 > Variable Alteration in sensoria or mental Obtundation Alert Alert/drowsy Stupor/coma Stupor/coma Total water deficits (l) Water deficits (ml/kg)† –200
 >250 >250 >250 >600. Arterial pH 7.25– –7.24 <7.00 >7.30. Serum bicarbonate (mEq/l) 15–18 10 to <15 <10 >18. Urine ketones* Positive Positive Positive Small. Serum ketones* Positive Positive Positive Small. Effective serum osmolality. (mOsm/kg)† Variable Variable Variable >320. Anion gap‡ >10 >12 >12 Variable. Alteration in sensoria or mental. Obtundation Alert Alert/drowsy Stupor/coma Stupor/coma. Total water deficits (l) 6 9. Water deficits (ml/kg)† –200.")
12
Precipitating Factors
INFECTION- most common precipitating factor (pneumonia/UTI/gastroenteritis/sepsis) Others: CVA, MI, Trauma, Pancreatitis, alcohol abuse, drugs (steroids, thiazides, pentamidine, sympathomimetics) Pregnancy Inadequate insulin administration Inc glucose (stress), dec insulin possible crises idiopathic type 1 diabetes, atypical diabetes, “Flatbush diabetes,” type 1.5 diabetes, and more recently, ketosis-prone type 2 diabetes
 Others: CVA, MI, Trauma, Pancreatitis, alcohol abuse, drugs (steroids, thiazides, pentamidine, sympathomimetics) Pregnancy. Inadequate insulin administration. Inc glucose (stress), dec insulin possible crises. idiopathic type 1 diabetes, atypical diabetes, Flatbush diabetes, type 1.5 diabetes, and more recently, ketosis-prone type 2 diabetes.")
13
Ketosis prone type 2 Diabetes
DKA cases without precipitating cause Presents acutely as DKA but eventually improves after a short period of insulin therapy prolonged remission is often possible, with eventual cessation of insulin treatment and maintenance of glycemic control with diet or oral antihyperglycemic agents. Fasting C-peptide levels of >1.0 ng/dl (0.33 nmol/l) and stimulated C-peptide levels >1.5 ng/dl (0.5 nmol/l) are predictive of long-term normoglycemic remission in patients with a history of DKA (28,32).
 and stimulated C-peptide levels >1.5 ng/dl (0.5 nmol/l) are predictive of long-term normoglycemic remission in patients with a history of DKA (28,32).")
14
Diagnosis History of polyuria, polydipsia, polyphagia, weight loss, vomiting, abdominal pain (only in DKA) dehydration, weakness, clouding of sensoria, and finally coma. Physical findings may include poor skin turgor, Kussmaul respirations (in DKA), tachycardia, hypotension, alteration in mental status, shock, and ultimately coma (more frequent in HHS).
 dehydration, weakness, clouding of sensoria, and finally coma. Physical findings may include poor skin turgor, Kussmaul respirations (in DKA), tachycardia, hypotension, alteration in mental status, shock, and ultimately coma (more frequent in HHS).")
15
Diagnosis Up to 25% of DKA patients have emesis, which may be coffee-ground in appearance and guaiac positive; Leukocytosis may be present and is attributed to stress and maybe correlated to elevated levels of cortisol and norepinephrine

16
Diagnosis The initial laboratory evaluation plasma glucose,
blood urea nitrogen/creatinine, serum ketones, electrolytes (with calculated anion gap)hypoNa,hyperK, hyperP osmolality, urinalysis, urine ketones by dipstick initial arterial blood gases complete blood count with differential, electrocardiogram Bacterial cultures of urine, blood, and throat, etc., if infection is suspected. HbA1c Serum sodium concentration is usually decreased because of the osmotic flux of water from the intracellular to the extracellular space in the presence of hyperglycemia Serum potassium concentration may be elevated because of an extracellular shift of potassium caused by insulin deficiency, hypertonicity, and acidemia. HbA1c may be useful in determining whether this acute episode is the culmination of an evolutionary process in previously undiagnosed or poorly controlled diabetes or a truly acute episode in an otherwise well-controlled patient. HyperP: Insulin deficiency, hypertonicity, and increased catabolism all contribute to the movement of phosphate out of cells.
hypoNa,hyperK, hyperP. osmolality, urinalysis, urine ketones by dipstick. initial arterial blood gases. complete blood count with differential, electrocardiogram. Bacterial cultures of urine, blood, and throat, etc., if infection is suspected. HbA1c. Serum sodium concentration is usually decreased because of the osmotic flux of water from the intracellular to the extracellular space in the. presence of hyperglycemia Serum potassium concentration may be elevated because of an extracellular shift of potassium caused by insulin deficiency, hypertonicity, and acidemia. HbA1c may be useful in determining whether this acute episode is the culmination of an evolutionary process in previously undiagnosed or poorly controlled diabetes or a truly acute episode in an otherwise well-controlled patient. HyperP: Insulin deficiency, hypertonicity, and increased catabolism all contribute to the movement of phosphate out of cells.")
17
Note on Ketones Detected using nitroprusside reaction:
semiquantitative estimation of acetoacetate and acetone levels; highly sensitive, but does not recognize the presence of β-hydroxybutyrate, the main metabolic product in ketoacidosis (4,12) Accumulation of ketoacids results in an increased anion gap metabolic acidosis.
 Accumulation of ketoacids results in an increased anion gap metabolic acidosis.")
18
Differential Diagnosis
1. Starvation ketosis and alcoholic ketoacidosis (AKA): plasma glucose concentrations that range from mildly elevated (rarely 250 mg/dl) to hypoglycemia. may have profound acidosis, but HCO3 usually not lower than 18 mEq/l An ethanol load in a fasting, healthy individual is likely to produce transient hypoglycemia within 6–36 h, secondary to the acute actions of ethanol on gluconeogenesis. This can temporarily result in abnormal glucose tolerance tests (with a resulting erroneous diagnosis of diabetes mellitus) until the alcoholic has abstained for 2–4 weeks.
: plasma glucose concentrations that range from mildly elevated (rarely 250 mg/dl) to hypoglycemia. may have profound acidosis, but HCO3 usually not lower than 18 mEq/l. An ethanol load in a fasting, healthy individual is likely to produce transient hypoglycemia within 6–36 h, secondary to the acute actions of ethanol on gluconeogenesis. This can temporarily result in abnormal glucose tolerance tests (with a resulting erroneous diagnosis of diabetes mellitus) until the alcoholic has abstained for 2–4 weeks.")
19
Diagnosis 2. Other causes of high–anion gap metabolic acidosis, including lactic acidosis, drug ingestion (salicylate, methanol, ethylene glycol, and paraldehyde) and chronic renal failure
 and chronic renal failure.")
20
Diagnostic Criteria Criteria DKA HHS blood glucose >250 mg/dl
arterial pH <7.3 >7.3 bicarbonate <15 mEq/l >15 mEq/l ketonuria or ketonemia moderate Mild effective serum osmolality >320 mOsm/kg H2O

21
Management

23
Fluid therapy In the absence of cardiac compromise, PNSS is infused at a rate of 15–20 ml/kg/h or 1–1.5 L during the first hour. Fluid replacement should correct estimated deficits within the first 24 h. Aggressive rehydration with subsequent correction of the hyperosmolar state has been shown to result in a more robust response to low-dose insulin therapy (54).
.")
24
Fluid Therapy During treatment of DKA, hyperglycemia is corrected faster than ketoacidosis. Hyperglycemia resolved in 6h; ketoacidosis in 12 h 5% dextrose should be added to replacement fluids to allow continued insulin administration until ketonemia is controlled while at the same time avoiding hypoglycemia.

25
Insulin Therapy patients with DKA have shown that insulin therapy is effective regardless of the route of administration infusion preferred: short half-life, easy titration (vs delayed onset of action and prolonged half-life of subcutaneous regular insulin) patients with severe DKA, hypotension, anasarca, or associated severe critical illness should be managed with intravenous regular insulin in the ICU
 patients with severe DKA, hypotension, anasarca, or associated severe critical illness should be managed with intravenous regular insulin in the ICU.")
26
Potassium 20–30 mEq potassium in each liter of infusion fluid is sufficient to maintain a serum potassium concentration within the normal range.

27
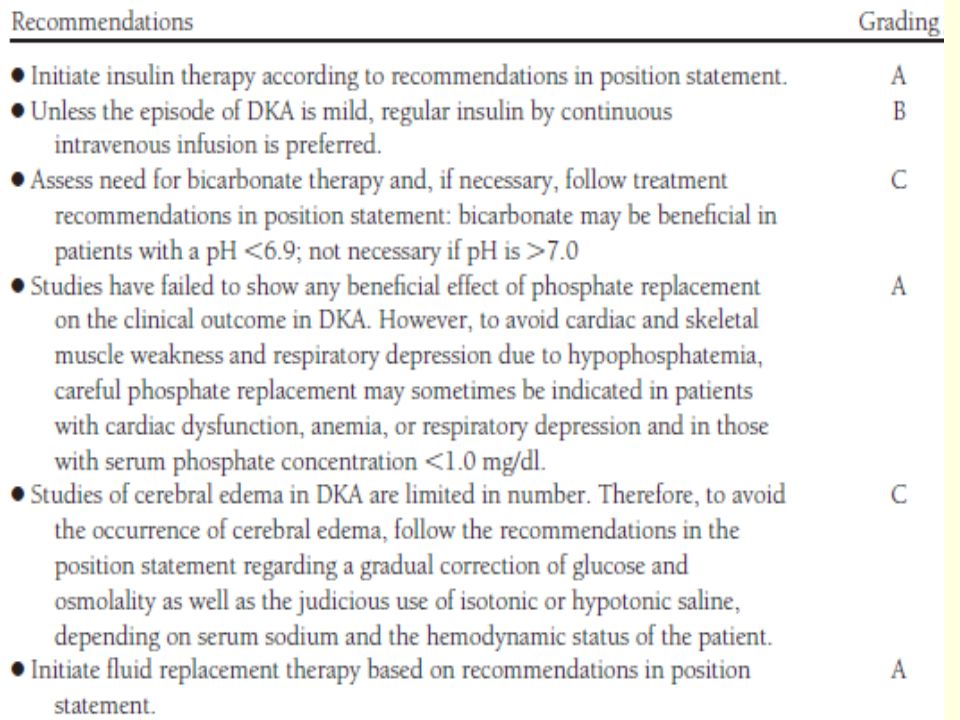
Bicarbonate Severe metabolic acidosis impaired myocardial contractility, cerebral vasodilatation and coma, and several gastrointestinal complications pH : HCO3 has no advantage in improving cardiac or neurologic functions or in the rate of recovery of hyperglycemia and ketoacidosis. A/E: increased risk of hypokalemia, decreased tissue oxygen uptake (65), cerebral edema (65), and development of paradoxical central nervous system acidosis.
, cerebral edema (65), and development of paradoxical central nervous system acidosis.")
28
Bicarbonate pH <6.9 give 100 mmol NaHCO3 (two ampules) in 400 ml sterile water with 20 mEq KCI given at a rate of 200 ml/h for 2 h until the venous pH is >7.0. If the pH is still <7.0 after this is infused, repeat infusion every 2 h until pH reaches >7.0
 in 400 ml sterile water with 20 mEq KCI given at a rate of 200 ml/h for 2 h until the venous pH is >7.0. If the pH is still <7.0 after this is infused, repeat infusion every 2 h until pH reaches >7.0.")
29
Phosphate NO beneficial effect of phosphate replacement on the clinical outcome in DKA Overzealous phosphate therapy can cause severe hypocalcemia (46,68). To avoid potential cardiac and skeletal muscle weakness and respiratory depression due to hypophosphatemia, careful phosphate replacement may sometimes be indicated in patients with cardiac dysfunction, anemia, or respiratory depression and in those with serum phosphate concentration <1.0 mg/dl (4,12).
. To avoid potential cardiac and skeletal muscle weakness and respiratory depression due to hypophosphatemia, careful phosphate replacement may sometimes be indicated in patients with cardiac dysfunction, anemia, or respiratory depression and in those with serum phosphate concentration <1.0 mg/dl (4,12).")
30
Phosphate When needed, 20–30 mEq/l potassium phosphate can be added to replacement fluids. The maximal rate of phosphate replacement generally regarded as safe to treat severe hypophosphatemia is 4.5 mmol/h (1.5 ml/h of K2 PO4) (69). No studies are available on the use of phosphate in the treatment of HHS.
 (69). No studies are available on the use of phosphate in the treatment of HHS.")
31
Transition to Subcutaneous Insulin
Criteria for resolution of ketoacidosis include a blood glucose <200 mg/dl and two of the following criteria: a serum bicarbonate level ≥15 mEq/l, a venous pH >7.3, and a calculated anion gap ≤12 mEq/l. Resolution of HHS is associated with normal osmolality and regain of normal mental status.

32
Transition to Subcutaneous Insulin
Allow an overlap of 1–2 h between discontinuation of intravenous insulin and the administration of subcutaneous insulin More recently, basal-bolus regimens with basal (glargine and detemir) and rapid-acting insulin analogs (lispro, aspart, or glulisine) have been proposed as a more physiologic insulin regimen in patients with type 1 diabetes (vs NPH and regular insulin).
 and rapid-acting insulin analogs (lispro, aspart, or glulisine) have been proposed as a more physiologic insulin regimen in patients with type 1 diabetes (vs NPH and regular insulin).")
33
Complications The most common complications of DKA and HHS include:
hypoglycemia due to overzealous treatment with insulin, hypokalemia due to insulin administration and treatment of acidosis with bicarbonate, Hyperchloremic non–anion gap acidosis, during the recovery phase of DKA, is self-limited (caused by loss of ketoanions and excess fluid infusion of chloride containing fluids during treatment) Cerebral edema is a rare but frequently fatal complication of DKA, occurring in 0.7–1.0% of children with DKA Hyperchloremic non–anion gap acidosis, during the recovery phase of DKA, is self-limited (caused by loss of ketoanions, which are metabolized to bicarbonate during the evolution of DKA and excess fluid infusion of chloride containing fluids during treatment)
 Cerebral edema is a rare but frequently fatal complication of DKA, occurring in 0.7–1.0% of children with DKA. Hyperchloremic non–anion gap acidosis, during the recovery phase of DKA, is self-limited (caused by loss of ketoanions, which are metabolized to bicarbonate during the evolution of DKA and excess fluid infusion of chloride containing fluids during treatment)")
35
Prognosis The prognosis of both conditions is substantially worsened at the extremes of age in the presence of coma, hypotension, and severe comorbidities (1,4,8, 12,13).
.")
36
Prevention Many cases of DKA and HHS can be prevented by better access to medical care, proper education, and effective communication with a health care provider during an intercurrent illness. 1. Early contact with the health care provider. 2. Emphasizing the importance of insulin during an illness and the reasons never to discontinue without contacting the health care team. 3. Review of blood glucose goals and the use of supplemental short- or rapid-acting insulin. 4. Having medications available to suppress a fever and treat an infection. 5. Initiation of an easily digestible liquid diet containing carbohydrates and salt when nauseated. 6. Education of family members: documenting temperature, blood glucose, and urine/blood ketone testing; insulin administration; oral intake; and weight. Supervision and staff education to prevent dehydration among elderly individuals (HHS)
")
37
Thank you.

Similar presentations


>")
>")









 DKA or Hyperglycemia coma is defined when blood sugar 300- 800mg/dl Is primarily seen in I.D.DM - can be seen in NIDDM. DKA.>")
. 2 Hyperglycaemia Learning objectives >Can state what hyperglycaemia is >Is aware of the short term and.>")





