Download presentation
Presentation is loading. Please wait.

1
Leontine Eskola, RN, BSN, CCRN Karen Alles, RN, BSN, CPN

2
Institute for Healthcare Improvement (IHI) 2006: 5 million lives campaign and prevention of Failure to Rescue Led initiative focused on reducing unnecessary mortality, AKA Failure to Rescue
 2006: 5 million lives campaign and prevention of Failure to Rescue Led initiative focused on reducing unnecessary mortality, AKA Failure to Rescue")
3
2005: RRT was rolled out for all of OHSU Adult Rapid Response Teams were well thought out, proper education and training provided The program at DCH was rolled out as an afterthought to the program on the adult side, little to no training or education

4
Lacked the education and structure to support successful implementation Deteriorated the informal support networks previously held between units Acute care and critical care did not like the formal RRT system

5
Needs Assessment What are our colleagues doing? Review of Literature

7
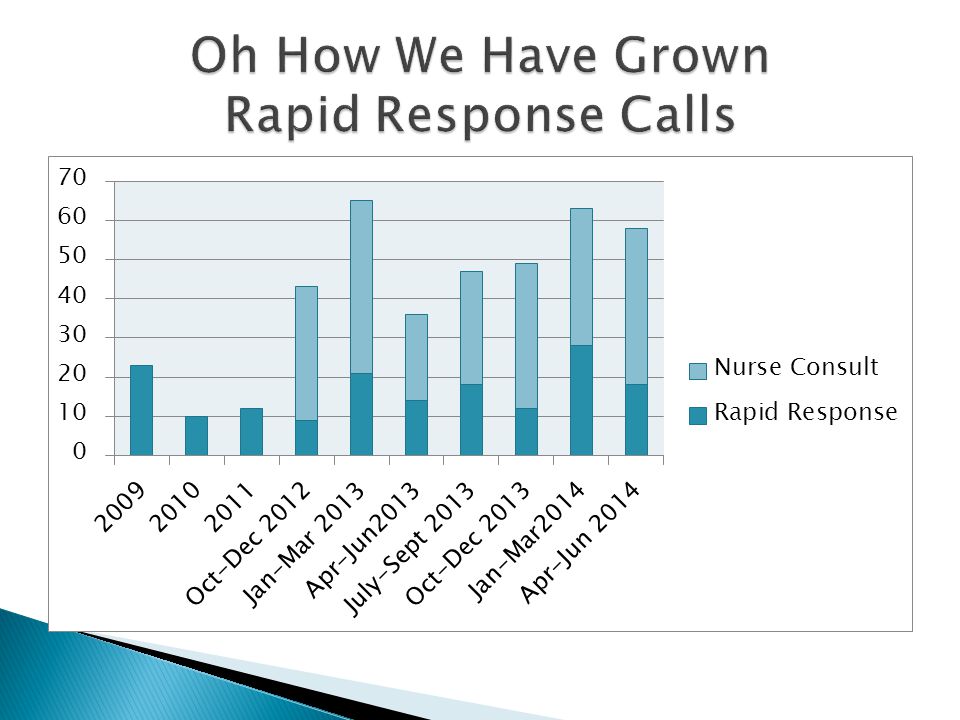
Nurse Consult 1 st Degree of Rescue Proactive Daily Rounds on each Acute Care unit Follow up on all recent PICU transfers PICU RN responder only 30-60minute response time Coordinate follow up acute care RN Rapid Response 2 nd Degree of Rescue Deteriorating patient PICU RN and RT Respond Notify primary team RRT was activated Respond urgently, within 10 min Follow up 4 hours after response Code Blue 3 rd Degree of Rescue Unresponsive Patient or Acute Deterioration Code Blue Team Responds (RN, RT, Intensivist) Immediate Response Time Transfer to ICU
 Immediate Response Time Transfer to ICU")
8
Manager Support Education for callers and responders Streamlined documentation with dot phrases in HER Simplified activation process: one pager for all calls Created an RRT assignment in the PICU 1 lower acuity patient Nurse consult/RRT Allowed time proactive interactions with units Rounding with charge nurses from units Responding to calls Follow up with staff and families from previous calls

9
Rollout with our Road Show

11
Responder Comments After I am just expected to know what to do I am not sure what to do if the patient isn't coding I like that it prevents a code Sometimes it provides great teaching moments Every page interrupts my work flow I actually don't feel like many people understand their roles I want more education for all involved I would make 2 levels of RRT, one which is not urgent, but a chance to huddle and troubleshoot Sometimes I am simply supporting what the RN is already doing. Good communication is never a bad thing I feel it breaks down barriers between the RNs on other units and the PICU RNs I think it allows us to collaborate on care and gain a better perspective of everyone's different jobs/roles and environment it is very helpful to get to know the pt BEFORE they are sicker I am just expected to know what to do I am not sure what to do if the patient isn't coding I like that it prevents a code Sometimes it provides great teaching moments Every page interrupts my work flow I actually don't feel like many people understand their roles I want more education for all involved I would make 2 levels of RRT, one which is not urgent, but a chance to huddle and troubleshoot Responder Comments Before Sometimes I am simply supporting what the RN is already doing. Good communication is never a bad thing I feel it breaks down barriers between the RNs on other units and the PICU RNs I think it allows us to collaborate on care and gain a better perspective of everyone's different jobs/roles and environment It is very helpful to get to know the patient BEFORE they are sicker

13
Expanded responder to all PICU RNs who expressed interest 4 hour class for all responders Personal Interactions Adjusted the PICU patient assignment (lower acuity) Addressed concerns about MD backup, and availability of supplies in acute care areas Charting expectations
 Addressed concerns about MD backup, and availability of supplies in acute care areas Charting expectations")
14
What is an appropriate patient to be on the watch list? Patients can be on the watch list due to heightened nursing concern. The watch list is also an appropriate place for patients outside of the ICU who have high risk, low frequency issues. This could include ventilated patients, patients with mediastinal chest tubes, or patients outside of a floor's area of expertise. What does it mean to be on the watch list? The RRT nurse knows that there is a patient in DCH that has a potential to need intervention, there is not a concern at this time. The RRT nurses will follow up with the patient's nurse and charge nurse during rounds if a patient is on the watch list. Watch list patients are not being followed by the PICU nurse with physical assessments OR chart assessments - these things happen with a nurse consult. How can I have a patient put on the watch list? Any pages to the RRT nurse to place a patient on the list need to include a nurse's name and phone number for a follow up conversation - no FYI pages for this.

15
Be tolerant of false alarms- we want to encourage a “if you think you need help ask for it” attitude. Get the word out- both initially and continually. Keep up education with new hires, reminding folks during training and competency days. Create an all in one resource for responders Thank you cards or follow up to callers acknowledging their role in advocating for their patient. Be open to new evolution of the system, i.e. the watch List Continued evaluation of current system.

16
"The names of the patients whose lives we save can never be known. Our contribution will be what did not happen to them. And, though they are unknown, we will know that mothers and fathers are at graduations and weddings they would have missed, and that grandchildren will know grandparents they might never have known, and holidays will be taken, and work completed, and books read, and symphonies heard, and gardens tended that, without our work, would never have been." Donald M. Berwick, MD, MPP Former President and CEO Institute for Healthcare Improvement

Similar presentations